










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A pair of researchers at Cornell University has developed a new way to monitor vital signs in patients—one that does not require direct contact with the skin.
In their paper published in the journal Nature Electronics, Xiaonan Hui and Edwin Kan describe the nature of the device and how it can be used.
The new device is based on RFID chip technology—the same technology used in key fobs. It works by sending a radio signal into the body and then listening to the signal that comes back (rather like sonar) and relaying what it finds to a nearby processing unit.
Hui and Kan discovered that the simple technology could be used to monitor vital signs if programed in specific ways.
By sending a signal into the chest, for example, and noting slight disturbances in the signal that is sent back, the device is able to monitor breathing activity.
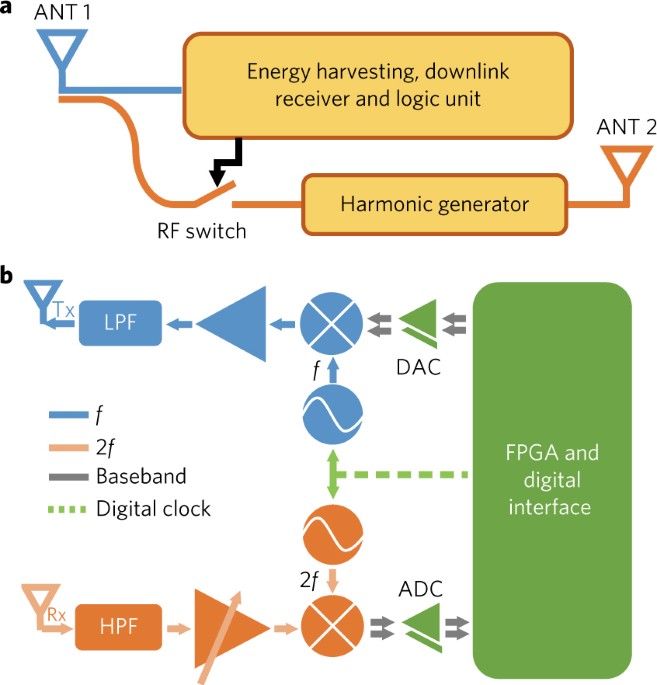
a, Passive harmonic RFID tag. The harmonic tag receives the downlink RF signal (at frequency f) from the reader. It goes through the tag Antenna 1 (ANT 1) and splits into two parts: one provides d.c. power for tag circuits by energy harvesting and the other is fed into the passive harmonic generator (at frequency 2f) to be re-emitted from Antenna 2 (ANT 2). b, Schematic of the harmonic RFID reader. The digital clock is fed into two frequency synthesizers at f and 2f for coherent demodulation at 2f. The digital module performs the code-division multiple-access (CDMA) protocol. The downlink commands from the reader to tags are modulated by the digital-to-analogue converter (DAC) and then upconverted by the mixer (blue) to the carrier at f. The harmonic tag backscatters to the reader at 2f, which is downconverted to the base band by the coherent local oscillator at 2f and sampled by the quadrature analogue-to-digital converter (ADC). Tx, transmitter; Rx, receiver; LPF, low-pass filter; HPF, high-pass filter; FPGA, field programmable gate array.
In roughly the same way, it can also monitor the heartbeat.
And by placing another of the devices near the wrist, it can be used to measure blood pressure by calculating elapsed time between heartbeats.
Because the device is so small, the researchers note, it could be sewn into a hospital gown or a bed sheet.
In such an arrangement, each patient would be monitored by one or more of the devices without attaching anything to the body.
They point out that the technology could actually be used to monitor more than one patient if need be.
And they further note that because the hardware already exists, using it to monitor patients would be inexpensive and easy to use by hospital staff.
They claim the devices are hardy, as well—they sent some through a clothes-washing machine a few times, and report that it still worked perfectly.
![Researchers demonstrate that lung stem cells can help regenerate injured lungs in laboratory mice [rejected]](https://3c1703fe8d.site.internapcdn.net/newman/gfx/news/2017/5a1d4fd3e104a.jpg)
Analyses of the NCS signal
The phase modulation is very sensitive to the physical location of the tag with respect to the reader. Hence, when Antenna 2 of the tag is placed on the chest, the breath information can be derived from the phase in the quadrature scheme, as shown in Fig. 3a with raw and low-pass-filtered waveforms.
Based on the backscattered phase information, the positions of multiple tags can be calculated with millimetre resolution (Supplementary Fig. 5), which can further derive the respiratory effort. Although the phase variation caused by the chest movement is much stronger than the internal movement of the heartbeat and wrist pulse, it is a ‘common component’ for NCS.
During our experiments, the NCS heartbeat signal was modulated on amplitude and is thus immune to the breath movement. Multiple frequencies, improved signal processing and reflection structure (Supplementary Fig. 6) can further help mitigate heavy multipath interference. As shown in Fig. 3b, we first retrieved the heart rate from the instantaneous period (blue solid line) and from the counts within 10 s (pink dashed line). The green markers were measured with a commercial blood pressure monitor (OMRON BP760N). Note that the breath and heartbeat information is independently derived from the quadrature demodulation, and no special filtering or pattern recognition as in the conventional microwave backscattering is required.
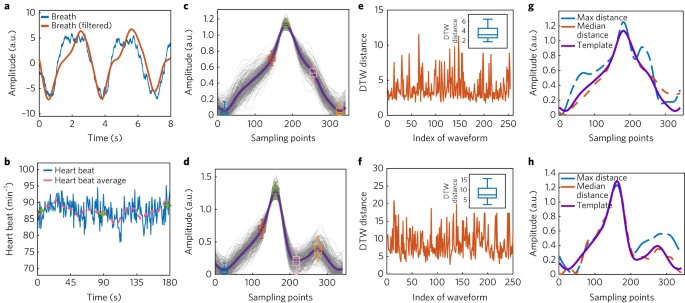
a, Raw breath signal and waveform after the low-pass filter. b, Raw heart rates and the average from the moving window of 10 s. Green markers show measurements from the OMRON blood pressure monitor mounted on the left forearm. c,d, Waveforms of heartbeat (c) and wrist pulse (d) during data collection for 3 min. The purple lines are the average waveforms of the 3-min data. The box-whisker plots in c are the statistical results at the minimum point (blue), rising deflection point (red), maximum point (green), falling deflection point (pink) and local minimum point (yellow). The box-whisker plots in d are at the minimum point (blue), rising deflection point (red), maximum point (green), local minimum point (pink), and local maximum point (yellow). e,f, DTW waveform analyses show the distance in each waveform of the heartbeat (e) and the wrist pulse (f). Insets: box–whisker distributions. g,h, Comparison of median- and maximum-distance waveforms with respective DTW template for the heartbeat (g) and wrist pulse (h). Sampling rate for the waveforms: 500 Sps.
Because the internal vital signals are retrieved from NCS, the interferometer-like structure significantly increases the sensitivity to enable collection of the motion waveform, similar to a ballistocardiogram (BCG). We recorded data from the chest and wrist tags simultaneously for 3 min. The experiments were conducted with the PCB tag and the reader antenna was ~1.5–2 m away from the person under test. The harmonic signal converted by the tag was about –20 dBm at 1.9 GHz (2f). To analyse the waveform variation, each period was overlaid to obtain the average and box-whisker deviation of the heartbeat and wrist-pulse waveforms (Fig. 3c,d). The waveforms are normalized to the 90th percentiles of the recorded data and the box-whisker plots show the variations of the feature points. We further applied the dynamic time warping (DTW) to sort the waveforms to derive the detailed features. Figure 3e,f shows the DTW distance for the heart and pulse waveforms and the insets show the variations. Figure 3g,h, presents a comparison of the extracted template waveforms with the maximum-distance and median-distance waveforms; the latter still closely resemble the template and keep most of the major features, such as the recoil peak in the wrist pulse. The detailed motion waveform analysis can be a cardiogram candidate for arrhythmia and aortic valvular diseases. A real-time waveform recording is shown in Supplementary Fig. 7 and Supplementary Video 2.
The CDMA protocol enables simultaneous monitoring of multiple persons and also multiple points on the same person. The allowable number of CDMA tags is limited by the baseband data rate and is shown in Supplementary Fig. 8. Comparison of the waveform timing from different body positions offers estimates of the blood pressure (BP) through the pulse transit time (PTT), which can be extracted from the feature points of the proximal and distal arterial waveforms. Our non-contact sensing of blood pressure presents significant advantages over direct pressure-based methods, which cause discomfort and disrupt the circadian rhythm, especially in long-term monitoring of elderly patients. We recorded the chest tag signal as the proximal waveform and the left wrist tag signal as the distal waveform for 3 min, as shown in Fig. 4a. PTT can be readily extracted from the major peaks of the two waveforms. Figure 4b shows the probability density of the PTT during the 3 min recording.
The distribution of the PTT may be affected by sampling jitter and waveform distortion. We can obtain one PTT sample for each heartbeat, and the moving average or other signal-processing methods can be readily applied to minimize the PTT variation.
Figure 4c,d shows the blood pressures calculated from the PTT as well as comparison points from the commercial blood pressure monitor (OMRON BP760N)
The data in Fig. 4c were collected when the person under test sat on a chair for about 30 min, while the data in Fig. 4d were collected after moderate activity.
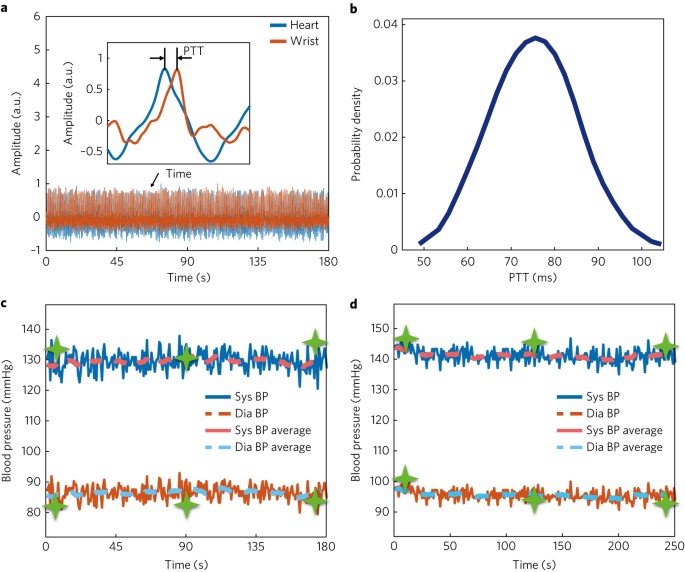
a, Pulse transit time (PTT) estimated from the synchronized heartbeat (blue) and wrist pulse (red) waveforms. Inset: one period of the signals and the extracted PTT. b, Probability density distribution of the PTT over 3 min. c,d, Blood pressure extracted from the PTT when the person under test is seated (c) and when the person under test goes through moderate activity and is standing (d). Green markers show blood pressures measured using a commercial blood pressure monitor. Blue and red solid lines are systolic (Sys) and diastolic (Dia) pressures (BP) of every heartbeat. Pink and light blue dashed lines are moving averages from 14 sampling points around 10 s.



{kind=link}