










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A minimally invasive treatment for retinal detachment gives patients sharper vision, less distortion and reduced side-effects, according to the findings of a randomized controlled trial performed at St. Michael’s Hospital in Toronto.
The findings have been published in Ophthalmology, the journal of the American Academy of Ophthalmology.
“The most commonly offered treatment for a retinal detachment in North America is an operating room surgery called a vitrectomy.
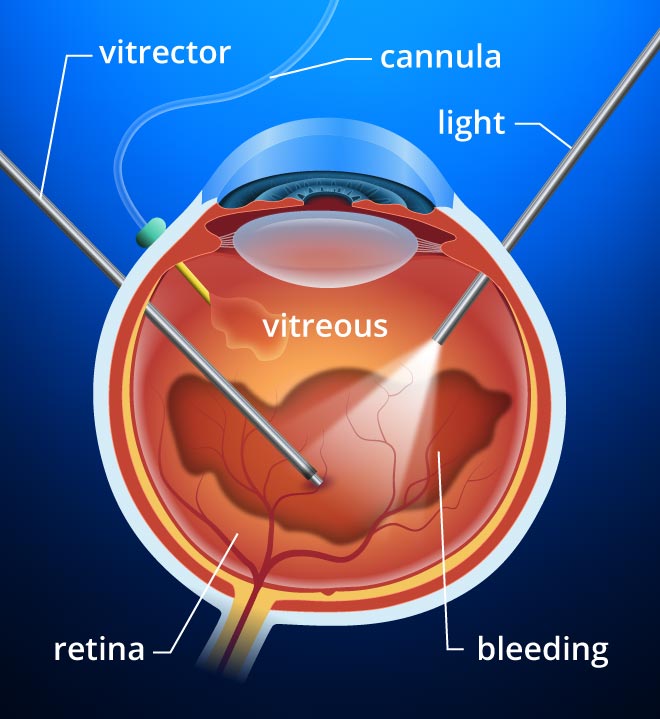
The results of this study clearly demonstrate that many retinal detachments will have better results for patients with an alternative minimally invasive office procedure,” said co-principal investigator Dr. Rajeev H. Muni, a vitreoretinal surgeon at St. Michael’s and researcher at the hospital’s Li Ka Shing Knowledge Institute.
“Although the better vision with the minimally invasive treatment (called pneumatic retinopexy, or PnR) is the most important finding of the study—and it should change how most retina specialists treat simple retinal detachments—we cannot ignore that PnR is also significantly less expensive to perform than vitrectomy (PPV), and offers significant hope to patients with retinal detachments in developing countries who would otherwise not be able to access care,” said Dr. Muni.
Pneumatic retinopexy was introduced by Hilton and Grizzard in 1986 as an outpatient procedure to repair rhegmatogenous retinal detachments. It supplemented the preexisting operative procedures used to repair rhegmatogenous detachments including scleral buckling and pars plana vitrectomy. It is an effective, non-invasive method of retinal detachment repair in selected cases.
Operation
-
Retinal reexamination with confirmation of all areas of pathology.
-
Local anesthesia administered for patient comfort. Use 2% lidocaine subconjunctivally or give a retrobulbar block if needed.
-
Cryotherapy is applied to pathology in detached retina. Highly elevated breaks may be flattened by a steamroller maneuver. Care should be taken to avoid excess cryotherapy to prevent possible release of RPE cells and subsequent PVR formation.[6] Laser photocoagulation can be used in attached areas of retina. Pseudophakic and high risk eyes may benefit from 360-degree laser.
-
Prepare intraocular gas. Use either SF6 or C3F8 drawn into a tuberculin syringe through the filter to provide tamponade of the detachment. Use the smallest bubble needed to cover the pathology, keeping in mind that the gas volume needed to cover a given arc of retina will increase with myopia. Pre-fill the system to remove dead space before drawing up the amount of gas to be injected and attaching a 30-gauge needle. SF6 will expand 2x and lasts for 1-2 weeks, wheras C3F8 will expand 4x and lasts 4-8 weeks.
-
Set up a sterile stand or towel near the eye for placing instruments. 10% Betadine drops are placed onto the eye. Some surgeons prefer to do a modified lid scrub. In patients with an allergy to Betadine, a broad-spectrum topical antibiotic may be used.
-
An anterior chamber paracentesis can be performed safely at this stage, and is especially useful in patients with glaucoma. The eye is stabilized with a cotton-tip swab, and a 27-gauge needle attached to a tuberculin syringe is used to enter the anterior chamber at the limbus. 0.2 – 0.4cc of fluid is usually withdrawn from the anterior chamber.
-
Intraocular gas injection. This is done through an entry site in a quadrant away from the detachment. Enter the eye vertically 3.5 – 4mm from the limbus, depending on the lens status, and inject the gas at a moderate pace. Injection of gas too quickly can cause a “fish eggs” phenomenon, which may require gentle tapping on the eye or positioning the bubbles away from the break for 24 hours to allow them to coalesce and avoid subretinal gas. To minimize the chance of fish eggs, it is helpful to pull the needle back a millimeter after the injection has begun to maintain one large gas bubble. Another potential complication is gas injection into the Canal of Petit, in which case it can be seen floating behind the lens as a “donut sign” or “sausage sign”; management may include overnight face-down positioning, which is usually effective, or passive drainage with a 27-gauge needle on a tuberculin syringe partially filled with BSS. Lastly, gas in the anterior chamber likely represents anterior migration due to ruptured zonules and can be managed by pupillary dilation followed by face-down positioning or by AC paracentesis with a 27-gauge needle.
-
Evaluation of IOP. Carefully evaluate the central retinal artery and confirm light perception. Loss of pulsations lasting longer than a few minutes requires decompression through an anterior chamber paracentesis.
-
Antibiotic or combination antibiotic/steroid ointment is applied to the eye and it is patched.
“There are many countries where patients simply don’t get treated in time because they can’t afford it. There are places where people with a detached retina just go blind.”
Dr. Roxane J. Hillier, the trial’s other co-principal investigator who is now based in the United Kingdom, said Europe has not yet fully embraced PnR primarily because of traditional practice patterns and misconceptions about the minimally invasive procedure.
“These findings cannot be ignored, by physicians and patients alike,” said Dr. Hillier.
“The next step is to educate surgeons worldwide about the ‘art’ of this elegant procedure, so that the excellent outcomes achieved in this trial can be replicated worldwide.”
The trial involved 176 patients who were randomly assigned to either PnR or PPV after being diagnosed with a retinal detachment.
The primary outcome being researched was visual acuity one year after treatment, as well as a metamorphopsia score for visual distortion, and anatomical success.
Patients who underwent PnR scored an average of 4.9 letters better on a standardized visual acuity test compared to those who had PPV, and had less visual distortion. A greater proportion of patients who had PnR achieved driving vision (20/40) in the affected eye (90.3 percent vs 75.3 percent). Although patients who had PPV treatment did have higher rates of primary anatomical success (93.2 percent versus 80.8 percent), patients who failed PnR still had very good visual outcomes, with secondary anatomical success being virtually identical between the groups.
Patients in the PnR group also reported quicker recoveries and better quality of life in the six months after being treated.
“One downside of PPV is that many patients will require a second operation, cataract surgery, within a year. This significantly delays visual recovery and can be avoided for the most part with PnR,” said Dr. Hillier.
Dr. Paul E. Tornambe, past president of the American Society of Retina Specialists, congratulated Drs. Muni and Hillier and the rest of their team “for completing a well-conceived and well-done” prospective randomized clinical trial.
“It is rare to prove a procedure (in this case PnR) not only results in better vision, is less invasive, restores the anatomy of the eye to its pre-detachment state, and avoids the operating room, but also costs significantly less than the more commonly used operation,” said Dr. Tornambe.
Dr. Muni also highlighted that the trial was the first to demonstrate that PnR can minimize visual distortion following retinal detachment repair and potentially avoid the so-called “Picasso effect,” which causes some patients to suffer significant impairments to their vision.
“It can be debilitating, patients can read the letters on the eye chart, but everything is warped,” Dr. Muni said.
“Many people end up learning to completely ignore the involved eye.
The issue of distortion is very important for patients, and the fact that it can be minimized with PnR is likely related to the better quality of retinal reattachment obtained with the procedure.”
Dr. Hillier and Dr. Muni also have ongoing studies trying to explain specifically why patients with PnR seem to have a better quality retinal reattachment, and they expect to present convincing data within the next year that compares the two treatments from an anatomical perspective at the microscopic level.
“Our group at St. Michael’s is taking this work one step further and currently enrolling patients in another randomized controlled trial comparing the two treatments in more complex retinal detachments,” said Dr. Muni.
More information: Roxane J. Hillier et al, The Pneumatic Retinopexy versus Vitrectomy for the Management of Primary Rhegmatogenous Retinal Detachment Outcomes Randomized Trial (PIVOT), Ophthalmology (2018). DOI: 10.1016/j.ophtha.2018.11.014
Journal reference: Ophthalmology search and more info website
Provided by: St. Michael’s Hospital search and more info



{kind=link}