










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A worldwide effort to lower people’s blood pressure, cut their sodium intake, and eliminate trans fat from their diet could dramatically reduce the incidence of premature death from cardiovascular disease (CVD) over a quarter century, according to a new study led by Harvard T.H. Chan School of Public Health.
“Focusing our resources on the combination of these three interventions can have a huge potential impact on cardiovascular health through 2040,” said lead author Goodarz Danaei, associate professor of global health at Harvard Chan School.
The study will be published online June 10, 2019 in the journal Circulation.
A large human study was initiated in year 2010 whose purpose was to assess whether targeting a reduction of systolic blood pressure below 120 mmHg was superior to the current standard of reducing it to below 140 mmHg.
The doctors focused on the systolic (top) number because it is a better predictor of heart attack and stroke. The “systolic” reading reflects the amount of pressure placed on the arterial system with each heartbeat.
The name of this study is Systolic Blood Pressure Intervention Trial, also known as SPRINT.1 It was published in the New England Journal of Medicine in 2015 and garnered huge media coverage.
The SPRINT study was supposed to last 5 years, but was stopped after 3.26 years because it was abundantly clear that the group whose blood pressure was reduced to a target systolic range under 120 mmHg were dying 26% less frequently.
What impressed the study’s researchers the most was a striking 43% lower relative risk of cardiovascular death in those whose blood pressure was aggressively reduced.
The SPRINT study also found that heart failure rates plummeted by 38% in patients whose target blood pressure aimed below 120 mmHg.
Heart failure occurs when the heart cannot pump enough blood and oxygen to support other organs in one’s body. It is a leading cause of hospitalizations and costs this nation an estimated $32 billion each year.4
Heart disease happens to be the number one cause of death in the United States, killing about 610,000 Americans each year.5 The dramatic (43%) drop in cardiovascular deaths shown in the SPRINT study motivated mainstream cardiologists to question their long-standing practice of largely ignoring their patient’s blood pressure until readings exceeded 139/89 mmHg.
Based on widespread media coverage and physician concurrence, it appears the medical establishment has finally woken up to what readers of this publication were told to do in the 1980s.
Historic Failures to Recognize Disease Causation
It is regrettable that practicing clinicians did not bother to observe that patients with blood pressure readings over 120/80 mmHg had elevated rates of cardiac death. But then again, it took decades of research to raise suspicion of a causative role of cigarette smoking in the development of lung cancer.
Physicians in the 1930s were certainly aware that respiratory illnesses happened with greater frequency in smokers. Yet it took decades of published research for the tobacco-disease causation issue to be raised, and it wasn’t until 1964 that the Surgeon General stated that smoking increases risk for a host of deadly illnesses.6
A similar scenario has occurred with the debate as to what the safe upper limit for blood pressure should be. Persuasive evidence and common sense long ago indicated that Life Extension’s recommendation of 115/75 mmHgwould spare many lives compared to the establishment’s position that blood pressure readings up to 139/89 mmHgwere alright.
Our Delicate Vasculature
The extremely fragile nature of our vascular system remains an unappreciated phenomenon.
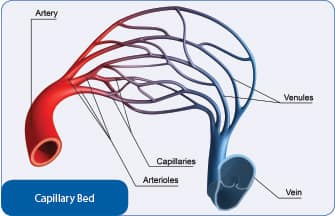
In youth, our arteries are flexible and readily expand and contract with each heartbeat as do our delicate capillary beds. As you can see by the illustration on this page, arteries narrow into smaller arterioles that eventually thin further down to microscopic capillaries. These capillaries are so tiny that red blood cells often have to bend their shape just to squeeze through and be returned to the venous system.
With each heart beat there is blood pressure exerted on arteries, arterioles, and delicate capillary beds. When blood pressure is in a perfect range, oxygen/nutrient enriched blood is delivered to all the body’s cells and returned to the heart with minimal damage to the vascular system.
Any increase in the pressure beyond what is needed to push blood through the vascular network causes additional stress and endothelial damage. This can manifest acutely in the form of a cerebral hemorrhage, where an arteriole in the brain ruptures and may quickly lead to death.
In most cases of higher-than-needed blood pressure, however, silent damage is constantly inflicted on the inner arterial lining (the endothelium) including the delicate capillaries.8 The result is a progressive loss of blood flow and cellular functionality that can manifest as ischemic heart disease,9-11 ischemic stroke,12-14 renal failure,15,16 and/or dementia.17-21
It was this fundamental understanding of the delicate structure of the vascular system that prompted Life Extensionto recommend lower blood pressure ranges in the 1980s.
Fallacy of “Prehypertension”
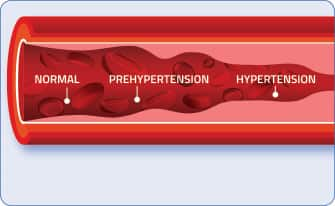
This graphic depicts a normal arteriole with red blood cells
flowing through and then the focal narrowing that occurs in
response to elevating blood pressures.
Not all physicians have been oblivious to the increased vascular risks in people with higher systolic blood pressure.
The term “prehypertension” was introduced to alert people that systolic pressure between 120 and 139 mmHg was reason to initiate lifestyle changes or modest drug therapy.
The problem with using the term prehypertension is that it caused patients and physicians to not take seriously the dangers it represents.
A systematic review on the clinical relevance of prehypertension was published in 2013 and revealed more increases in vascular risk than the carefully controlled SPRINT study.
The authors of this 2013 review performed an analysis of 18 previous studies that included a whopping 468,561patients. They found that patients with prehypertension had a:22
- 55% increased risk of cardiovascular disease,
- 50% increased risk of coronary heart disease,
- 71% increased stroke risk.
The authors went a step further and looked at people in the low prehypertension range, defined by systolic blood pressure of just 120 to 129 mmHg. Risk of cardiovascular disease in this prehypertension group was 46% higher than for individuals with systolic blood pressure levels below 120 mmHg.
According to this very large analysis, even lower-range prehypertension has a significant impact on morbidity and mortality, which is why Life Extension has urged for so long that optimal blood pressure readings are 115/75 mmHg.
Based on the totality of the evidence, the term “prehypertension” should be discarded and most adults with systolic blood pressure over 119 mmHg should face the reality that they are hypertensive from a medical definition standpoint, i.e., they are at an increased risk of health problems.
This is analogous to the term prediabetes, which is used today to describe people with fasting glucose between 100–125 mg/dL. These individuals should instead be diagnosed as “diabetic” and treated accordingly. This includes lifestyle modifications that safely reduce blood glucose levels to optimal ranges.
Please know that upper-level acceptable systolic blood pressure readings at one time were considered a startling high of 160 mmHg. They were later reduced to 150 mmHg, then to 140 mmHg, and mercifully now down to 120 mmHg.
Do Not Rush to Lower Blood Pressure
The SPRINT study was released in 2015 and is likely to be a game-changer as it relates to better guidelines for blood pressure control. There were, however, limitations that cause us to urge caution before initiating steps to drastically lower your blood pressure.
The SPRINT study was of relatively short duration and longer term side effects from the aggressive drug therapies may not be fully understood.
Type II diabetics were excluded from SPRINT because a previous trial on diabetics called ACCORD failed to show a benefit in aggressively reducing their blood pressure.23 This failure may reflect the devastating impact on the vascular system inflicted by the elevated glucose levels seen in diabetics. Said differently, the severity of the endothelial damage that diabetics sustain might overwhelm the beneficial effects of aggressively lowering their systolic blood pressure.
Those who have had chronic higher blood pressure levels often suffer considerable damage to their delicate endothelial linings.8,24 An unfortunate consequence for some individuals is that they need to maintain somewhat higher blood pressure levels to provide adequate blood flow to the capillaries in their brain, kidneys and other tissues.
We have discussed this problem in previous issues of this publication, whereby those with severely damaged capillary beds require higher blood pressure to sustain organ/tissue function, even though over the longer term this higher pressure on the arterial system inflicts additional damage to the endothelium.25
The sad case for some individuals is that taking overly aggressive steps to push down blood pressure levels could create side effects such as hypotension, which causes one to faint.
A more serious effect observed in the SPRINT study was that there was almost a 3.5-fold increased risk of kidney damage in those aggressively treated for hypertension using multiple drugs. It is not known if it was the multiple drugs or overly aggressive lowering of the blood pressure that caused this kidney damage.
The authors of the SPRINT study were quick to point out that the huge reductions in morbidity and mortality in the aggressively-treated hypertensive group far outweighed the side effect risks observed. As one outside doctor who critiqued the study stated, “If there is a problem with an individual patient, you can always back off.”26
OUR PRECIOUS ENDOTHELIUM
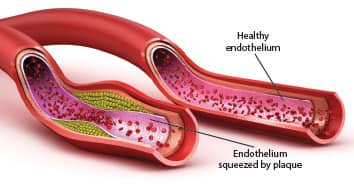
Our inner arterial lining is called the endothelium.
The endothelium is an ultra-thin, one-cell-thick layer of cells. It loses youthful function in response to normal aging.
An underappreciated factor in the development of cardiovascular disease is endothelial dysfunction. The consequences of endothelial dysfunction are diminished circulation, high blood pressure, thrombosis, and atherosclerosis, all of which are major causes of stroke and heart attack.27-31
Fortunately, astute scientists have discovered potent natural methods to tackle the underlying causes of endothelial dysfunction.
In addition to nutritional/lifestyle interventions, maintaining optimal blood pressure readings is essential to protect against loss of endothelial function.
Providing You with Real World Guidance
The encouraging news about all this is that if one intelligently embarks on a program to reduce their blood pressure to more optimal ranges, there are simple blood tests available that can identify if adverse effects are occurring in response to overly aggressive drug treatment.
These and other commonsense approaches to achieving optimal blood pressure levels are described in articles contained in this month’s issue. Readers should understand that the more one is willing to make healthier lifestyle changes, the less in the way of antihypertensive drugs they are likely to need, which should translate into a lower side effect risk profile.
We published an article 1.7 years ago that describes the ideal antihypertensive drug to begin with. This drug (telmisartan) not only lowers blood pressure in what we consider the most efficient manner, but has side benefits that include improvements in endothelial function and survival not seen with other antihypertensive medications.
MAJORITY OF ADULTS ARE HYPERTENSIVE AND PREVALENCE INCREASES AS WE AGE!
Most of you reading this article have higher-than-optimal blood pressure, or are effectively treating it.
Whether you treat it successfully or not, you are still classified as a hypertensive patient, just as one with high blood sugar is still a diabetic even though they may take enough medication to bring glucose down to a normal level.
The following chart reveals the huge percentage of noninstitutionalized persons with hypertension (defined as having measured high blood pressure and/or taking antihypertensive medication) between the years 2011-2014.32
| Men | 65-74 years | 63.4% |
| 75 years and over | 72.3% | |
| Women | 65-74 years | 64.3% |
| 75 years and over | 79.9% |
These data clearly show hypertension increasing with age, which makes taking control of one’s blood pressure so critical if one is to avoid the most common causes of death and disability.
References
- Sprint Research Group, Wright JT, Jr., Williamson JD, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373(22):2103-16.
- Available at: http://www.mayoclinic.org/diseases-conditions/high-blood-pressure/basics/definition/con-20019580. Accessed August 22, 2016.
- Available at: http://www.cdc.gov/bloodpressure/facts.htm. Accessed June 14, 2016.
- Huynh-Hohnbaum AL, Marshall L, Villa VM, et al. Self-Management of Heart Disease in Older Adults. Home Health Care Serv Q. 2015;34(3-4):159-72.
- Available at: http://www.cdc.gov/heartdisease/facts.htm. Accessed August 22, 2016.
- Available at: https://profiles.nlm.nih.gov/NN/B/B/M/Q/. Accessed November 28, 2015.
- Available at: http://www.cdc.gov/nchs/fastats/deaths.htm. Accessed August 22, 2016.
- Dharmashankar K, Widlansky ME. Vascular endothelial function and hypertension: insights and directions. Curr Hypertens Rep. 2010;12(6):448-55.
- Rosendorff C, Black HR, Cannon CP, et al. Treatment of hypertension in the prevention and management of ischemic heart disease: a scientific statement from the American Heart Association Council for High Blood Pressure Research and the Councils on Clinical Cardiology and Epidemiology and Prevention. Circulation. 2007;115(21):2761-88.
- Mukherjee D, Campbell CL. Optimal management of hypertension in patients with ischemic heart disease. Cardiovasc Hematol Agents Med Chem. 2009;7(3):198-205.
- Agbor-Etang BB, Setaro JF. Management of Hypertension in Patients with Ischemic Heart Disease. Curr Cardiol Rep.2015;17(12):119.
- Johansson BB. Hypertension mechanisms causing stroke. Clin Exp Pharmacol Physiol. 1999;26(7):563-5.
- Chalmers J, Todd A, Chapman N, et al. International Society of Hypertension (ISH): statement on blood pressure lowering and stroke prevention. J Hypertens. 2003;21(4):651-63.
- Available at: http://www.medscape.com/viewarticle/473113. Accessed August 23, 2016.
- Bidani AK, Griffin KA. Long-term renal consequences of hypertension for normal and diseased kidneys. Curr Opin Nephrol Hypertens. 2002;11(1):73-80.
- Whitworth JA. Progression of renal failure — the role of hypertension. Ann Acad Med Singapore. 2005;34(1):8-15.
- Faraco G, Iadecola C. Hypertension: a harbinger of stroke and dementia. Hypertension. 2013;62(5):810-7.
- Joas E, Backman K, Gustafson D, et al. Blood pressure trajectories from midlife to late life in relation to dementia in women followed for 37 years. Hypertension. 2012;59(4):796-801.
- Skoog I, Lernfelt B, Landahl S, et al. 15-year longitudinal study of blood pressure and dementia. Lancet.1996;347(9009):1141-5.
- Shah NS, Vidal JS, Masaki K, et al. Midlife blood pressure, plasma beta-amyloid, and the risk for Alzheimer disease: the Honolulu Asia Aging Study. Hypertension. 2012;59(4):780-6.
- Ninomiya T, Ohara T, Hirakawa Y, et al. Midlife and late-life blood pressure and dementia in Japanese elderly: the Hisayama study. Hypertension. 2011;58(1):22-8.
- Huang Y, Wang S, Cai X, et al. Prehypertension and incidence of cardiovascular disease: a meta-analysis. BMC Med.2013;11:177.
- Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362(17):1575-85.
- Hausberg M, Lang D, Barenbrock M, et al. Large artery wall properties — what is relevant for the classic management of hypertension?. Dtsch Med Wochenschr. 2005;130(46):2657-61.
- Available at: http://www.lifeextension.com/magazine/2015/3/best-drug-to-treat-hypertension/page-01. Accessed August 23, 2016.
- Available at: http://www.reuters.com/article/us-health-heart-bloodpressure-idUSKCN0SY2F920151109. Accessed August 23, 2016.
- Fordjour PA, Wang Y, Shi Y, et al. Possible mechanisms of C-reactive protein mediated acute myocardial infarction. Eur J Pharmacol. 2015;760:72-80.
- Eelen G, de Zeeuw P, Simons M, et al. Endothelial cell metabolism in normal and diseased vasculature. Circ Res.2015;116(7):1231-44.
- Huveneers S, Daemen MJ, Hordijk PL. Between Rho(k) and a hard place: the relation between vessel wall stiffness, endothelial contractility, and cardiovascular disease. Circ Res. 2015;116(5):895-908.
- Seals DR, Jablonski KL, Donato AJ. Aging and vascular endothelial function in humans. Clin Sci (Lond).2011;120(9):357-75.
- Pearson JD. Endothelial cell function and thrombosis. Baillieres Best Pract Res Clin Haematol. 1999;12(3):329-41.
- Available at: http://www.cdc.gov/nchs/fastats/older-american-health.htm. Accessed August 23, 2016.
Researchers used global data from multiple studies and estimates from the World Health Organization in making their calculations.
They estimated that scaling up treatment of high blood pressure to 70% of the world’s population could extend the lives of 39.4 million people.
Cutting sodium intake by 30% could stave off another 40 million deaths and could also help decrease high blood pressure, a major risk factor for CVD.
And eliminating trans fat could prevent 14.8 million early deaths.
More than half of all delayed deaths, and two-thirds of deaths delayed before age 70, are projected to be among men, who have the highest numbers of noncommunicable disease deaths globally, researchers found. Regions expected to benefit most from the interventions include East Asia, the Pacific, and South Asia, as well as countries in sub-Saharan Africa.
The authors said that a variety of programs and policies would be necessary to reduce premature CVD-related deaths.
One important strategy would be to increase the use of blood pressure medications, many of which are safe and affordable.
The researchers acknowledged that scaling up the three interventions would be a “huge challenge,” requiring countries to commit additional resources to boost health care capacity and quality.
But they added that previous analyses have shown that the interventions are achievable and affordable.
For example, a Kaiser Permanente program in Northern California increased control of hypertension to 90% among thousands of the health system’s patients between 2001 and 2013, using strategies such as improved treatment protocols, patient-friendly services, and healthcare information systems that facilitate tracking people with hypertension.
Similar approaches have been adapted and tested in some low- and middle-income countries, leading to notable improvements in hypertension treatment and control, the authors said.
“These are realistic goals that have been shown to be attainable on smaller scales,” said Danaei. “We need the commitment to scale up the programs to achieve them globally.”
More information: “Three Public Health Interventions Could Save 94 Million Lives in 25 Years,” Vasilis Kontis, Laura K. Cobb, Colin D. Mathers, Thomas R. Frieden, Majid Ezzati, Goodarz Danaei, Circulation, June 10, 2019, DOI: 10.1161/CIRCULATIONAHA.118.038160
Journal information: Circulation
Provided by Harvard T.H. Chan School of Public Health



{kind=link}