









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



If you’re a parent, you know the looks.
The looks you get when your child is acting out in public — causing a scene over candy at the grocery store or wailing over a toy in the mall.
But here’s the thing: Most parents have a clear idea of what triggered the behavior (a Snickers bar, for example, or Fingerlings).
Now imagine what it would be like if your child could spark into an uncontrollable meltdown at any time, often for no discernible reason.
Or no predictable reason, anyway.
After Michele Kong’s son Abram was diagnosed with autism at age 4, “we realized very quickly that trivial inputs such as bright lights or a crying baby or a barking dog could result in a verbal outburst or a meltdown,” she said. Kong is a pediatrician at the University of Alabama at Birmingham and Children’s Hospital and a founder of KultureCity, a nonprofit that works to “create acceptance and inclusion for all individuals with unique abilities,” according to its mission statement.
‘It’s not just autism ’
Isolation is the opposite of inclusion.
And that’s exactly where many parents of children with autism spectrum disorders find themselves, because anywhere from 80 to 100 percent of people with an autism diagnosis experience meltdowns.
Public meltdowns often convince parents to stay home.
When bystanders see someone acting out, they tend to think, or say, something like “control your child!” or “control yourself!”
It may not look like it, but that’s exactly what’s happening, Kong says: a “stim” — referring to stereotyped or repetitive motor movements, use of objects, or speech — can be the brain’s way of trying to tune out sensory overload and regain control of a chaotic situation.
The root causes of meltdowns are the sensory processing difficulties in the brains of people with ASD, Kong says.
“And we’re realizing that it goes beyond autism,” she added.
Individuals with ADHD, Down syndrome, PTSD, cerebral palsy, fetal alcohol syndrome and several other conditions often experience sensory integration problems as well.
These sensitivities can quickly lead to sensory overload in noisy, active environments such as restaurants, playgrounds, stores and sporting events.
Kong prefers the term “come-apart,” rather than meltdown, she said.
“It’s not just children; it can be a 30-year-old veteran with PTSD who may experience the same issue with sudden loud noises as a 5-year-old with autism at an NBA game.”
She likes to illustrate the point with a YouTube video:
Some people with autism have difficulty processing intense, multiple sensory experiences at once.
This animation gives the viewer a glimpse into sensory overload, and how often our sensory experiences intertwine in everyday life. Credit: Alkurhah.
“This is what it means to have sensory sensitivity or dysregulation,” as Kong explains during her public talks.
Brains and filters
The brain acts somewhat like a coffee filter, Kong says.
It focuses attention on a limited set of stimuli and moves redundant inputs into the background.
But if you have a sensory integration issue, “your brain can’t regulate all the different input coming at it,” she said.
“It can be extremely disorienting.”
These “sensory gating” difficulties affect sight, sound, touch, taste, and smell.
They also interfere with proprioception and vestibulation, related parts of the sensory system “that let you know where you are in space,” Kong said.
Some have described feelings of floating in space and being ungrounded.
This is why, for some people, weighted vests or blankets are calming, and for others, being in a corner or having their back against the wall is regulating.”
Researchers are making progress in understanding the mechanisms behind sensory dysfunction.
In a review paper published in 2018, Rajesh Kana, Ph.D., Melissa Thye and other members of Kana’s Cognition, Brain and Autism Laboratory at UAB wrote that “while prior research has often focused on the sensory and social features of ASD independently of one another, new theoretical and empirical evidence suggests a stronger relationship between the two than previously thought.”
(See “Social sensing: How sensory processing differences may contribute to autism symptoms.”)
Translating for today
This research is fascinating and promising, Kong says.
But as a parent of a child with autism, she has a pressing question:
“How can we translate this understanding into something that we can do today?”
That question led Kong and her husband, Julian Maha, who is also a physician, to found KultureCity.
The nonprofit’s Sensory Inclusive initiative trains venues on how to be welcoming to guests with sensory processing issues and their caregivers.
“We approached it from the family and individual angle,” Kong said.
“We want to change the mindset of our communities.
We want the message to be: ‘We want you here.
We are going to meet you in the middle.’
We felt that was the fastest way to have the biggest and most direct impact.”

The root causes of meltdowns are the sensory processing difficulties in the brains of people with ASD, Kong says. The image is in the public domain.
KultureCity has provided training to venues across the United States and in several countries around the globe.
It has worked with more than 200 stadiums, arenas, museums and other venues across the United States, including the homes of the New York Mets, Pittsburgh Steelers, Golden State Warriors and more. KultureCity is an official NBA partner and has hosted special events for the NFL at the Super Bowl and Pro Bowl and for Major League Baseball during the All-Star Weekend.
This year, KultureCity was named one of the World’s Most Innovative Companies by the magazine Fast Company.
Stopping before they start
What’s their secret?
“Our focus is on prevention,” Kong said.
“We teach how to prevent a guest from having a sensory overload.
Because it’s always easier to prevent a come-apart than to try to de-escalate once the overload has happened.”
1. Know what to look for
Sensory Inclusive training starts by teaching staff “what sensory sensitivity looks like,” Kong said.
Staff members are taught the value of being proactive versus reactive.
That includes seeing the attraction or event through new eyes.
“If they know it’s going to be a really loud environment” at one point in a game or show, for instance, “they can let the guest know that that is a time when they can step out to go to a quiet space,” Kong said.
KultureCity encourages venues to waive “no re-entry” policies and let guests with sensory issues step outside for a few minutes to recover before going back in.
2. Know what to say
Communicating with guests who have ASD or another sensory processing disorder requires some simple changes, Kong said.
“You need to use simple, direct language.” For example, in a medical setting, pediatric nurses might tell a child that an upcoming test is “a piece of cake,” she explained.
“But for a child with autism, they will be expecting a literal piece of cake.”
People don’t realize how much they use “softening” language in everyday speech, “and that can be confusing,” Kong added.
A museum docent might say,
“We don’t want to be too loud, do we?” Kong said.
But that polite suggestion to be quiet can go right over the head of a concrete-thinking person with ASD, Kong said.
“It is OK to say ‘You need to be quiet.’ It is also important to always use direct language.”
3. Share the tools
Sensory Inclusive venues have special bags available for guests that contain noise-reducing headphones, a weighted lap pad, and other helpful items.
They also include KultureCity VIP badges that unobtrusively let staff know that a patron has a sensory processing issue.
The venues also have Social Stories personalized to the location.
They explain, in child-friendly words and pictures, what to expect. (A list of all Sensory Inclusive venues, along with their Social Stories, is on the KultureCity app.)
“Knowing what’s going to happen beforehand has the potential to decrease anxiety,” Kong said. “The idea is to pre-expose them to the experience.”
These efforts can make a big difference to parents.
“To know that it’s going to be OK that your child is going to get up and walk around — it’s hard for me to put into words how life-changing it is,” said one parent in a KultureCity video.
“Inclusion and accessibility mean everyone,” Kong said. “We want everyone to be part of the community.”
Social sensing: Studies suggest how sensory processing differences may contribute to autism symptoms
In a 2018 paper, researchers in UAB’s Cognition, Brain and Autism Laboratory summarized the growing number of studies suggesting links between sensory processing differences and social behaviors in ASD.
These behaviors, the authors write, “may arise from a common underlying mechanism and/or may exert reciprocal influence on each other in the course of a child’s development.”
Speech recognition:
Many individuals with ASD are highly attuned to changes in pitch, for example.
But recent studies indicate that, while this is true for non-speech sounds, such as music, the ability does not carry over to speech sounds.
“Enhanced auditory processing of pitch and oversensitivity to loudness can result in heightened awareness of simple perceptual features of auditory information at the exclusion of complex auditory input such as speech,” the UAB researchers write.
Vision:
Visual processing differences are now recognized “as one of the earliest stable markers of ASD,” the researchers explain. In brain imaging studies of infants later diagnosed with ASD, investigators have found lower-than-typical activation in several regions involved in visual processing, including the fusiform face area, superior temporal sulcus, and the occipital face area.
“It is possible that pre-existing visual processing deficits may disrupt developing social skills by preventing the perception of visual cues that signal social rewards, making the cause and effect of social interactions unpredictable,” the UAB scientists write.
“Over time, these infants might begin to lose interest in the ‘unpredictable’ social interactions, and instead seek out repetitive and predictable non-social stimulation.”
Touch:
Touch, the UAB authors point out, plays a key role in social bonding.
“Positive tactile stimuli (touch, warmth, odors) can release oxytocin, the neuropeptide primarily involved in social bonding,” they write.
“However, the behavioral and neural effects of oxytocin [are] negatively correlated with autistic-like traits.
This may lead to a limited seeking of touch in the interpersonal interactions of individuals with ASD.”
Putting it all together:
Even beyond these individual sensory issues, the brain’s ability to turn a bundle of sensory input into a cohesive picture of the world seems to be damaged in many people with ASD.
“The automatic integration of multimodal stimuli creates a predictable social environment out of ‘noise’ and inevitably influences how an individual interacts socially within that environment,” the UAB authors write.
“For example, infants at high risk for ASD do not show differential looking during congruent and incongruent speech and lip-movement; this indicates difficulty matching auditory and visual information.”
One theory posits a “temporal binding window” that is dysfunctional in ASD.
“Timing information is crucial to binding and integrating associated stimuli,” the UAB authors write.
“A longer temporal binding window could create a ‘fuzzier,’ unpredictable sensory environment as unrelated stimuli become bound together.
Throughout development, important social cues may fail to become integrated or salient.
For example, the concurrent lip-movement and the voice of a parent calling a child’s name may not become salient over the other co-occurring stimuli in the environment.
This would affect social responses and potentially lead to a preference for restrictive, repetitive behaviors as a refuge from the unpredictable social environment.”
Sensory Processing in Children
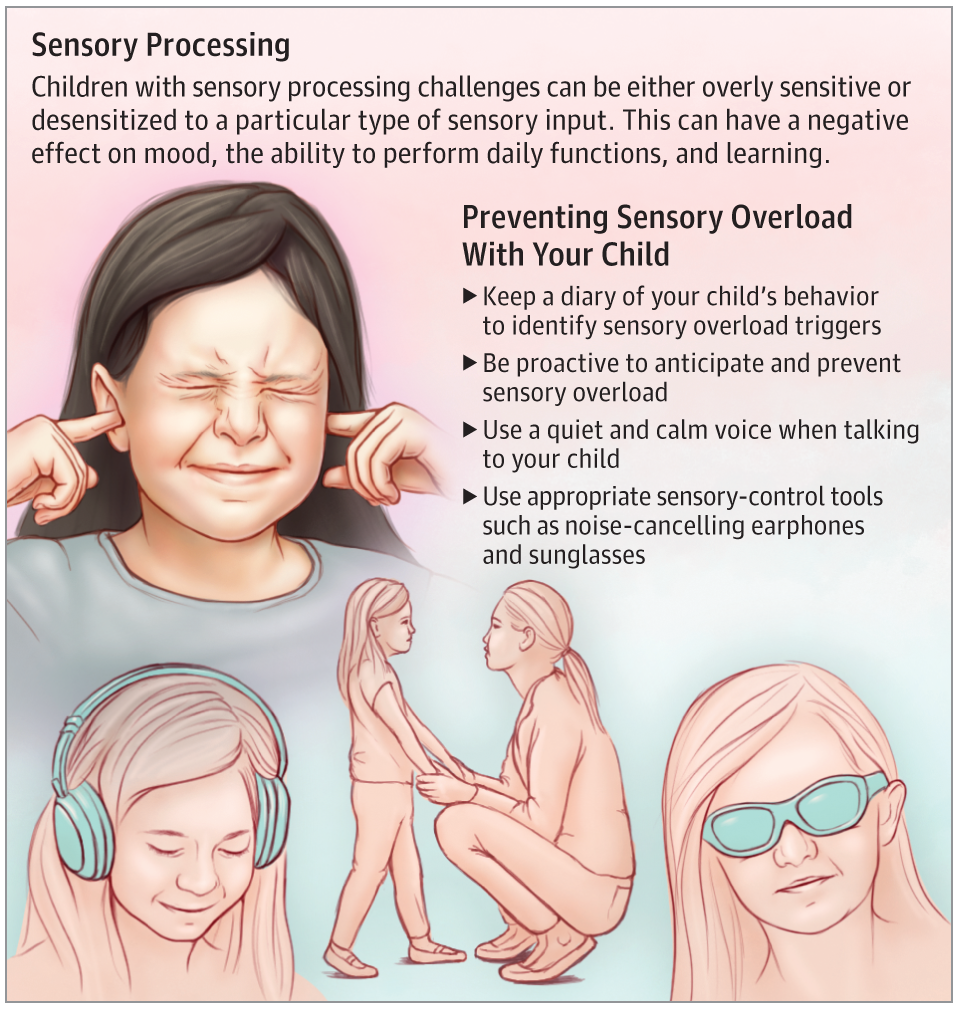
Sensory processing relates to the way our brain manages the information received from our sensory organs to create an appropriate response to incoming stimuli.
Our senses include 5 external senses: touch, taste, smell, hearing, and sight.
Two additional internal senses include proprioception, which gives us body awareness and a sense of the movements and positions of our body, and vestibulation, which gives us a sense of balance and motion.Who Is Affected by Sensory Processing?
One in 6 children have sensory processing difficulties. In specific populations, the prevalence is estimated to be as high as 80% to 100% and includes children with autism spectrum disorder or who have a history of prematurity, fetal alcohol syndrome, or Down syndrome, just to name a few.What Happens When a Child Has Sensory Processing Difficulties?
A child with sensory processing difficulties can be overresponsive or underresponsive to a particular sensory input.
For instance, in children who are overresponsive to loud noise or bright lights, the noise and light that is tolerable to others is too much for them, and they respond by covering their ears and squinting their eyes.
In contrast, those who are underresponsive to sound may present as children who do not turn to important sounds (for instance, name being called) or have intense rocking and swaying for those who are underresponsive to the proprioceptive and vestibular input.
This is also children who do not feel pain or seek out extra tactile input via touching of objects in their environment.
They can also have sensory defensiveness manifested as, for instance, intolerance to clothing tags or certain food textures.
Children with sensory processing difficulties can also have frequent meltdowns (crying, screaming, kicking, collapsing, having self-injurious behavior, or aggression) that can potentially interfere with daily functioning and their ability to learn.What Can Be Done to Prevent Sensory Overload?
If you suspect that a child is in sensory overload, it is important to use simple, specific, and concrete language. Always use a quiet and calm voice.
If the triggers are known, it is critical that parents take a proactive vs a reactive approach.
To be reactive is to respond to a need when the child is already in trouble, for instance, calming a child who is already in full-blown sensory overload.
To be proactive is to anticipate the sensory overload and take measures to prevent the overload from happening in the first place.
Use sensory tools such as noise-cancelling headphones for those with noise sensitivities or sunglasses for those with light sensitivities. Write social stories that tell the encounter in first-person language to allow the child to have a sense of what will happen before it happens.
What Should You Do If You Suspect That Your Child Might Have Sensory Processing Difficulties?
Keep a sensory diary of what the triggers appear to be for the sensory overload. You will want to call your pediatrician, who will ask you questions related to triggers and events surrounding the sensory overload. You might be referred to a developmental pediatrician or an occupational therapist for further evaluation and management.
For More Information
- https://www.healthychildren.org/English/health-issues/conditions/developmental-disabilities/Pages/Sensory-Integration-Therapy.aspx
- To find this and other JAMA Pediatrics Patient Pages, go to the For Patients collection at jamanetworkpatientpages.com.
The JAMA Pediatrics Patient Page is a public service of JAMA Pediatrics. T
he information and recommendations appearing on this page are appropriate in most instances, but they are not a substitute for medical diagnosis.
For specific information concerning your child’s medical condition, JAMA Pediatrics suggests that you consult your child’s physician.
This page may be photocopied noncommercially by physicians and other health care professionals to share with patients. To purchase bulk reprints, call 312/464-0776.
Current Neuroscience Evidence
Registration and Modulation: Emotion-Related Brain Regions (Previously Referred to as the Limbic System)
As previously stated, Ayres [8] suggested that a collective set of brain regions associated with emotions, often called the limbic system, is responsible, in part, for sensory registration.
She posited that these regions of the brain are atypical in children with ASD and therefore, these children do not register and value stimuli in the same way as TD children.
Moreover, Ayres proposed that, “the more poorly this part (of the brain) is working, the less the autistic child will respond to therapy” (p. 124).
In other words, the more abnormal the limbic system (she did not specify functional or structural differences), the less likely SI therapy will effectively ameliorate sensory processing impairments. Within the last decade, current neuroscience research has affirmed Ayres’ assertions that limbic emotion-processing regions are impaired in individuals with ASD [14,15,16,17,18].
Findings from this research provides evidence to support predictions of impairments of registration, as well as modulation of sensory processing in ASD.
However, to date, there is no research that specifically tests Ayres theories regarding effectiveness of interventions using a SI approach as a function of neural functioning in ASD.
For a review of behavioral outcomes of ASI therapy see [19,20,21,22].
The term, limbic system, refers to a specific set of regions thought to encompass emotion-related brain regions.
The system is comprised of several subcortical nuclei and cortical structures including the insula, hypothalamus, hippocampus, parahippocampal gyrus, amygdala, fornix, mammillary body, septal nuclei, cingulate gyrus and dentate gyrus on both sides of thalamus [23].
These regions are involved in emotion, motivation, learning, memory and certain aspects of sensory processing.
Additional regions outside of the limbic system, such as the prefrontal cortices and ventral and medial sectors, are now known to also be important to emotion processing [24].
Here we will collectively refer to these regions as emotion-related brain regions, a term that is currently preferred [25].
Brain Structure and Function
Consistent with Ayres’ theory, current research has thoroughly documented that individuals with ASD have both structurally and functionally atypical emotion-related brain regions [17,18,26,27,28].
These regions have been observed to be abnormal in size and function across the lifespan [29], however, it is still not clear if volume or responsivity are increased or decreased or how these abnormalities underlie symptomology in ASD.
Structurally, volume size trajectories across development for these regions start out larger in children with ASD than in TD children [30,31].
It is thought that children with ASD have an overgrowth of neurons that diminishes in adolescents [32].
In older adolescence and adulthood, there are mixed findings regarding emotion-related structures.
For example, it has been observed that adults with ASD have reduced amygdala [33] and hippocampus volume compared to typical individuals [34,35,36] while other studies have reported increased hippocampal volume [37] or no differences [38].
In some instances, the cortical and subcortical volume of regions in this system have been related to cognitive functioning (i.e., social processing, attention) [39,40,41].
In general, increased volume in structures has been found to be related to ASD deficits [42].
However, it is not well understood how structural components of this system relate to sensory processing specifically.
A few white matter studies have reported variation in tracts connecting emotion-related brain regions to auditory and cognitive processes [43,44] and white matter volume related to motor skills [45].
Motor impairments in ASD have also been found to be positively correlated with white matter volume in regions of the brain stem, the central tegmental tract/medial lemniscus [46].
The lemniscus conveys tactile information and proprioception to the cortex via the thalamus.
This finding provides some support for Ayres theory that the brainstem structures are related to sensory motor impairment in ASD.
However, more research is needed to fully understand the specificity of how brain structures are related to sensory impairments in ASD.
Studies of neural activation (function) in emotion-related brain regions have similarly reported abnormal functioning in ASD.
The amygdala in particular has been consistently found to be dysfunctional. Neuroscience research published at the time of Ayres’ career reported that the amygdalae contain a larger proportion of neurons that signal valance than other emotional-related brain regions and are responsive to motivationally significant stimuli [47].
Ayres predictions about the connection between impaired detection and understanding of the meaning of stimuli (registration) and the “limbic system” may indeed, in part, be due to functional disruptions in the amygdalae in ASD.
In Ayres’s lectures and notes, she identified the amygdala as being involved in sensory registration (USC Archives) [11].
The amygdala has since continued to be implicated in recognizing valence in stimuli [48] as well as encoding reward associations of visual stimuli and attention [49].
Moreover, many studies report attenuated amygdala activity when individuals with ASD perform social tasks compared to typical individuals [50,51,52].
Yet, other researchers have found that in individuals with ASD that the amygdala over-activates with eye-gaze compared to typical controls and that in these individuals amygdala activation is correlated to time spent gazing (i.e., looking at eyes) [53,54].
Hyperactivation in the amygdala to eye contact may indicate a modulation dysfunction in ASD in which some have proposed an indication for why individuals with ASD avoid eye contact with others [54,55].
This hypothesis suggests that avoiding eye contact is a motivational response [56], which aligns with Ayres’ understanding of motivation (see Section 3.2).
Alternatively, it also has been posited that individuals with ASD are not aversive to eye-gaze but are indifferent to it; that is, they do not perceive others’ eyes as informative or salient stimuli [57,58,59].
This lack of saliency detection may be why other studies have observed amygdala hypoactivation. In regard to “registration,” Ayres discussed individuals with ASD as having impairments in both the detection of a stimulus at the level of the central nervous system (CNS) and in salience perception.
Current findings support both definitions.
The amygdala has been frequently implicated in attention [49] and recognizing valence in stimuli [48] as well as in encoding reward associations of visual stimuli [49].
In addition to “limbic regions”, Ayres specifically hypothesized that the vestibular nuclei (located in the brain stem) were involved in registering visual input and in helping to make it meaningful to the child [8] (p. 125).
To date, no neuroimaging studies have investigated the vestibular nuclei and “registration” in ASD specifically, however, it is possible that abnormalities in the amygdala—which receives projections from the medial vestibular nucleus via autonomic nuclei and parabrachial nucleus [60]—may play a role in registration disturbances.
The insula is an important emotion-related region not identified by Ayres that is involved in registration deficits in ASD [61].

The insula is important for attention and is a core node of the salience network, which responds to novel and relevant sensory stimuli and is important for cognitive control and switching between default mode networks (introspective functions) to task-based networks [62].
The insula also acts as an integration center for physiological and emotion perception [63]. This cortical region has been repeatedly reported to be altered in ASD [64,65,66].
Insula abnormalities have been observed in individuals with ASD while performing various cognitive tasks, such as social processing tasks, emotion processing, spatial attention [67,68], set-shifting tasks [69] and executive function tasks [64,70,71].
Together, current neuroimaging research supports Ayres’ framework by providing evidence that emotion-related brain regions are structurally and functionally different in individuals with ASD compared to TD individuals.
Further, research findings suggest that these regions are important for registration of sensory information and that they are disrupted in a way that impairs sensory modulation. These differences, however, are multifaceted and may depend upon methodology (i.e., age, stimuli, instruction, etc.).
Individual regions, such as the amygdala or insula, are part of a much larger emotional processing network and are physically and functionally connected to other regions.
The connectivity between these regions and other brain regions also contribute to SI disruptions in ASD and are discussed below. Functional task-based MRI studies that directly investigate how different sensory experiences are processed in ASD are reviewed later.
Functional Connectivity
While characterization of brain regions provide insight into ASD dysfunction, a systems level approach in the last decade has provided additional understanding into how sensory information is communicated within and between networks.
Recent research has examined network functioning of specific regions, including emotion-related brain regions in those who are TD and individuals with ASD.
Although there are some inconsistencies [72], significant evidence to indicates that individuals with ASD have atypical network connectivity.
This has led some to characterize ASD as a disorder of altered brain connectivity [73,74].
These functional connectivity studies identify areas of the brain where activation patterns are synchronized across time.
For example, Rudie et al. [75] observed that children and adolescents with ASD displayed reduced functional connectivity between the amygdala and secondary visual areas while passively viewing emotional expressions compared to the TD control group.
Moreover, the study found that increased ASD symptom severity correlated with decreased connectivity, thereby suggesting that reduced communication between visual input and emotion responsivity is related to ASD symptomatology.
These and similar findings [73,76] also lend support to Ayres’ postulation regarding the severity of abnormal “limbic” functioning and SI by demonstrating that the degree of symptom severity corresponds with the degree of sensory registration disruptions.
Indeed, Ayres did predict that deficits in sensory processing hinder motor planning, which may ultimately result in trouble with more complex behavior, including social and emotional cognition [8] (p. 129). How this network responds to sensory stimulation is discussed later.
In addition to task-based connectivity networks, several functional networks are intrinsic to neural functioning and are thought to be related to different aspects of sensory processing (i.e., default mode network, salience network, motor network, auditory network, etc.).
These networks closely resemble functional networks that are active when performing tasks [77,78] and are often referred to as resting state networks.
Findings from current resting state studies suggest that individuals with ASD have disrupted connectivity in many of these networks. Hypo- or hyper-connectivity findings suggest that individuals with ASD have greater and/or weaker communication with networks compared to typical peers, regardless of specific tasks or stimuli.
Several of the studies correlate behavioral symptomatology to the strength of these network connections, indicating that impairments in neural modulation are not restricted to region specific impairments.
In a recent study Maximo and Kana [79] reported that individuals with ASD demonstrated network dysfunction in many sensory processing networks, including hyperconnectivity in auditory-subcortical, motor-thalamic and lateral visual-basal ganglia networks and hypoconnectivity in medial visual-subcortical networks.
This and other studies indicate that functional networks supporting primary sensory processing are impaired in ASD at the intrinsic level [15,79,80,81,82,83] and may prevent appropriate integration of sensory information in higher order sensory integration regions.
Ayres [8] described individual’s impairments in registration as “capricious” due to neural inefficiencies. Indeed, findings of reduced network efficiency are observed in other types of network analysis, such as graph theory analysis [51,84].
Neural Responses to Aversive or Pleasant Sensory Stimulation
An increasing number of neuroimaging studies examine neural processing during exposure to specific kinds of sensory input (i.e., tactile, auditory, visual) [85,86].
These studies demonstrate that individuals with ASD have differences in “limbic system” responsivity to visual input (flashing checkerboard), auditory input (loud noises) and tactile input (aversive or pleasant material) compared to TD participants [87,88,89].
Cascio and colleagues [89] found tactile pleasantness (determined by a −100 to 100 hedonic rating scale) varied in ASD compared to TD adults.
Although psychophysical or perceived ratings of roughness and pleasantness were largely similar across the two groups, the ASD group gave pleasant (i.e., cosmetic brush) and unpleasant (i.e., plastic mesh) textures more extreme ratings than did controls.
Moreover, ASD participants rated neutral textures with more variance than those in the control group, thus indicating that ASD adults are less consistent when evaluating ambiguous stimulus.
It is possible that this variance in rating reflects the degree of sensitivity and discriminative ability that some individuals with ASD may have.
Further, changes in blood oxygenation level-dependent (BOLD) signal in response to stimulation differed substantially between the groups; the ASD group exhibited diminished responses in the posterior cingulate cortex and the insula, particularly for pleasant and neutral textures, compared to the control group.
For the most unpleasant textured stimuli, the ASD group exhibited greater BOLD response than controls in affective somatosensory processing areas, including the posterior cingulate cortex and the insula.
The insula’s amplitude of response to the unpleasant texture was positively correlated with social impairment as measured by the Autism Diagnostic Interview-Revised (ADI-R [90]).
According to these results, individuals with ASD show diminished response to pleasant and neutral stimuli and exaggerated emotion-related region responses to unpleasant stimuli, providing support for Ayres’ [8] theory of modulation deficits in ASD, both behaviorally and neurologically.
In a set of complementary studies, high-functioning youth with ASD and age- and Intelligence Quotient-equivalent TD youth were presented with adverse sensory stimuli during an functional magnetic resonance imaging (fMRI) scan [86,91,92,93].
In response to the stimuli, ASD participants displayed greater BOLD activation in primary sensory cortical areas and limbic structures including the amygdala, hippocampus and orbital-frontal cortex [92].
In both groups, the level of activity in these areas positively correlated with parent’s ratings of their child’s sensory responsivity on the Sensory Over-Responsivity Scales (SOR) [92,94].
In a more recent study investigating functional connectivity between emotion and sensory brain regions during sensory aversion of auditory and tactile stimuli (white noise and scratchy texture), Green and colleagues [91] found that individuals with ASD displayed aberrant modulation of connectivity between the thalamus (pulvinar nucleus) and sensory-motor regions compared to their TD peers.
Specifically, they posited that increased amygdala-pulvinar connectivity may be related to selective attention in ASD since the amygdala signals the brain to attend to distracting sensory stimuli.
Taken together, these results demonstrate that youth with ASD show neural hyper-responsivity to adverse sensory stimuli and that behavioral symptoms characterized by SOR may be related to both heightened responsivity in primary sensory brain regions and emotion-related brain regions at both the regional and network level.
Again, these findings provide support for Ayres theory of disrupted modulation of sensory stimuli in emotion-related regions in ASD.
In a follow up study, Green and colleagues [86] investigated the effect of adverse sensory distractions on the brain while participants performed a social cognition task involving the interpretation of visual and audio cues (sarcasm task [95]).
When the aversive stimuli (scratchy material) was applied while participants completed the task, individuals with ASD showed decreased activations in language and dorsolateral and dorsomedial prefrontal cortex compared to when no aversive stimulus was applied. Activation in these regions was not correlated with SOR scores, suggesting that the reduced activation was not related to sensory deficits.
When the participants were given instructions to focus on the face and voice during the social task, the addition of the adverse stimulus did not decrease activation in the ASD group but increased activation in the medial prefrontal cortex.
This finding demonstrates that explicit instructions for attention can increase medial prefrontal activation during this sarcasm task.
The researchers of this study theorize that sensory stimuli can disrupt neural networks processing social information in ASD and that instruction may mitigate this effect. All of the fMRI sensory studies described above corroborate Ayres’ [8] postulate that emotion-related brain regions have atypical modulation responses when experiencing different sensory modalities in children with ASD compared to TD individuals.
Source:
University of Alabama at Birmingham
Media Contacts:
Matt Windsor – University of Alabama at Birmingham
Image Source:
The image is in the public domain.
Original Research: Open access
“The impact of atypical sensory processing on social impairments in autism spectrum disorder”.Melissa D. Thye, Haley M. Bednarz, Abbey J. Herringshaw, Emma B. Sartin, Rajesh K .Kana.
Developmental Cognitive Neuroscience. doi:10.1016/j.dcn.2017.04.010



{kind=link}