










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A new reusable device created by the Johns Hopkins University can help women with breast cancer in lower income countries by using carbon dioxide, a widely available and affordable gas, to power a cancer tissue-freezing probe instead of industry-standard argon.
A study detailing the tool’s success in animals was published this month in PLOS One.
“Innovation in cancer care doesn’t always mean you have to create an entirely new treatment, sometimes it means radically innovating on proven therapies such that they’re redesigned to be accessible to the majority of the world’s population,” says Bailey Surtees, a recent Johns Hopkins University biomedical engineering graduate and the study’s first author.
“This project is a remarkable example of success from the Biomedical Engineering Design Program,” says Nicholas Durr, an Assistant Professor of Biomedical Engineering at Johns Hopkins and the study’s senior author.
“This team of undergraduates has been so successful because they created a practical solution for the problem after really understanding the constraints that needed to be met to be impactful.”
The largest cause of cancer-related mortality for women across the globe, breast cancer disproportionately affects women in lower-income countries due to lack of treatment. While the survival rate for women in the United States is greater than 90%, they are significantly lower at 64%, 46% and 12% in Saudi Arabia, Uganda and The Gambia, respectively.
“Instead of saying ‘She has breast cancer,” the locals we met while conducting focus groups for our research said ‘She has death,’ because breast cancer is often considered an automatic death sentence in these communities,” adds Surtees.
In lower-income countries, the main barriers to treating breast cancer are inadequate treatment options – with surgery, chemotherapy and radiation being impractical or too expensive – and long travel times to regional hospitals where efficient treatment is available.
Even if a woman is able to travel to a hospital for treatment, she may not be seen and recovery times will keep her out of work for an additional few weeks.
Killing cancerous tissue with cold, or cryoablation, is preferable to surgically removing tumors in these countries because it eliminates the need for a sterile operating room and anesthesia, thus making it possible to local clinics to perform the procedure.
It’s also minimally invasive, thereby reducing complications such as pain, bleeding and extended recovery time.
Animation demonstrating how a new device from the Johns Hopkins University uses carbon dioxide to power a cancer tissue freezing device instead of argon. Credit: Kubanda Cryotherapy
Current cryoablation technologies, however, are too expensive, with a single treatment costing upwards of $10,000, and are dependent on argon gas, which typically isn’t available in lower-income countries, to form the tissue-killing ice crystals.
With these barriers in mind, the student-led research team, named Kubanda (which means “cold” in Zulu), wanted to create a tissue-freezing tool that uses carbon dioxide, which is already widely available in most rural areas thanks to the popularity of carbonated drinks.
The research team tested their tool in three experiments to ensure it could remain cold enough in conditions similar to the human breast and successfully kill tumor tissue.
In the first experiment, the team used the tool on jars of ultrasound gel, which thermodynamically mimics human breast tissue, to determine whether it could successfully reach standard freezing temperatures killing tissue and form consistent iceballs.
In all trials, the device formed large enough iceballs and reached temperatures below -40 degrees Celsius, which meets standard freezing temperatures for tissue death for similar devices in the United States.
For the second experiment, the team treated 9 rats with 10 mammary tumors.
Afterwards, they looked at the tissue under a microscope and confirmed that the tool successfully killed 85% or more tissue for all tumors.
Finally, the team tested the tool’s ability to reach temperatures cold enough for tissue destruction in the normal liver of a pig, which has a temperature similar to a human breast.
The device was successfully able to stay cold enough during the entire experiment to kill the target tissue.
“When we started the project, experts in the area told us it was impossible to ablate meaningful tissue volumes with carbon dioxide.
This mindset may have come from both the momentum of the field and also from not thinking about the importance of driving down the cost of this treatment,” says Durr.
While the results are promising, the device still requires additional experiments before it’s ready for commercial use.
Mainly, the research team’s next steps are to ensure it can consistently kill cancer tissue under the same heat conditions as human breast tissue.
In the near future, the team hopes to continue testing their device for human use, and expand its use to pets.
Malignant tumors are the primary cause of death from disease in developed nations (1). The main treatment options for tumors are surgery and chemo- and radiation therapy (2), which yield good results (3).
Nonetheless, these treatments also have various side effects (4). Therefore, there is a need for novel antitumor therapies that are not associated with side effects or complications.
Carbon dioxide (CO2) has been mainly used as a treatment for peripheral vascular disorders (5). The benefits of a carbonated spa have long been known in Europe (6), and are still enjoyed in many countries (7).
Bathing in artificial CO2-enriched water has been shown to improve ischemic limb symptoms (8).
CO2 exerts therapeutic effects by stimulating blood flow and microcirculation (9) to increase partial O2 pressure in local tissue, which is known as the Bohr effect (10).
We previously investigated whether the Bohr effect can be induced by transcutaneous CO2 application using 100% CO2 gas and CO2 absorption-enhancing hydrogel in humans (11).
We showed that transcutaneous application of CO2 to the lower limbs in rats for three months activated the expression of peroxisome proliferator-activated receptor gamma co-activator 1α in the tibialis anterior muscle, and increased the number of mitochondria in skeletal muscles, even in malignant tumor tissues (12–14).
We also found that this CO2 treatment could induce mitochondrial apoptosis in human malignant fibrous histiocytoma/undifferentiated pleomorphic sarcoma (MFH/UPS) (13), murine osteosarcoma (15), and human oral squamous cell carcinoma (14) without any side effects such as loss of body weight and induction of metastasis.
These results suggest that percutaneous CO2 treatment can be used as an antitumor therapy. However, before initiating clinical trials, the optimal conditions, including the duration and frequency of transcutaneous CO2 application, must be established to decrease tumor volume and induce apoptosis in tumor cells.
The present study represents a preclinical test to investigate the antitumor effects of transcutaneously applied CO2, against three types of human tumors, with regard to treatment conditions including duration, frequency, and site of CO2 exposure, in mouse xenograft models.
Materials and methods
Cell lines
MDA-MB-231 human breast cancer cells (American Type Culture Collection (ATCC), Rockville, MD, USA) (16), MG63 human osteosarcoma cells (ATCC) (17), and Nara-H human MFH/UPS cells (ScienStuff Co., Nara, Japan) (13,18) were maintained in Dulbecco’s modified Eagle’s medium supplemented with 10% (v/v) fetal bovine serum and 100 U/ml penicillin/streptomycin solution (all from Sigma-Aldrich, St. Louis, MO, USA) at 37°C in a humidified atmosphere of 5% CO2.
Animal models
Male, athymic BALB/c nude mice (5–8 weeks old) were obtained from CLEA Japan (Tokyo, Japan). The animals were maintained under pathogen-free conditions; experiments were performed in accordance with the Guidelines for Animal Experimentation of Kobe University Graduate School of Medicine and Kobe University Animal Experimentation Regulations (permission nos. P110905-R1 and P-101203) and were approved by the Institutional Animal Care and Use Committee. To create human tumor xenograft models, MDA-MB-231 (3.0×106), MG63 (5.0×106), and Nara-H (5.0×106) cells in 500 µl of phosphate-buffered saline (PBS) were injected into the dorsal subcutaneous area of mice, as previously described (13–15).
CO2 treatment was initiated after cell implantation when the tumors were of a measurable size. T
umor volume and body weight were monitored twice weekly until the end of the treatment. Tumor volume was calculated as described previously (13,18), using the formula: V = π/6 × a2 x b, where a and b represent the shorter and longer dimensions of the tumor, respectively.
Transcutaneous CO2 application
For treatment, CO2 was administered transcutaneously, as described previously (12–15). Briefly, the area of skin around the implanted tumor was treated with a CO2 hydrogel. The area was then sealed with a polyethylene bag, and 100% CO2 gas was delivered into the bag.
Effect of treatment duration on different tumor types
Based on the average tumor volume after the tumors reached a measurable size, 24 mice for each cell line were randomly divided into four groups of six mice each; these groups received the treatment for 0, 5, 10, or 20 min per application, with the applications performed twice weekly for 2 weeks (12–15). Results are shown as the ratio of the final tumor volume to the corresponding pre-treatment value.
Effect of treatment frequency and interval
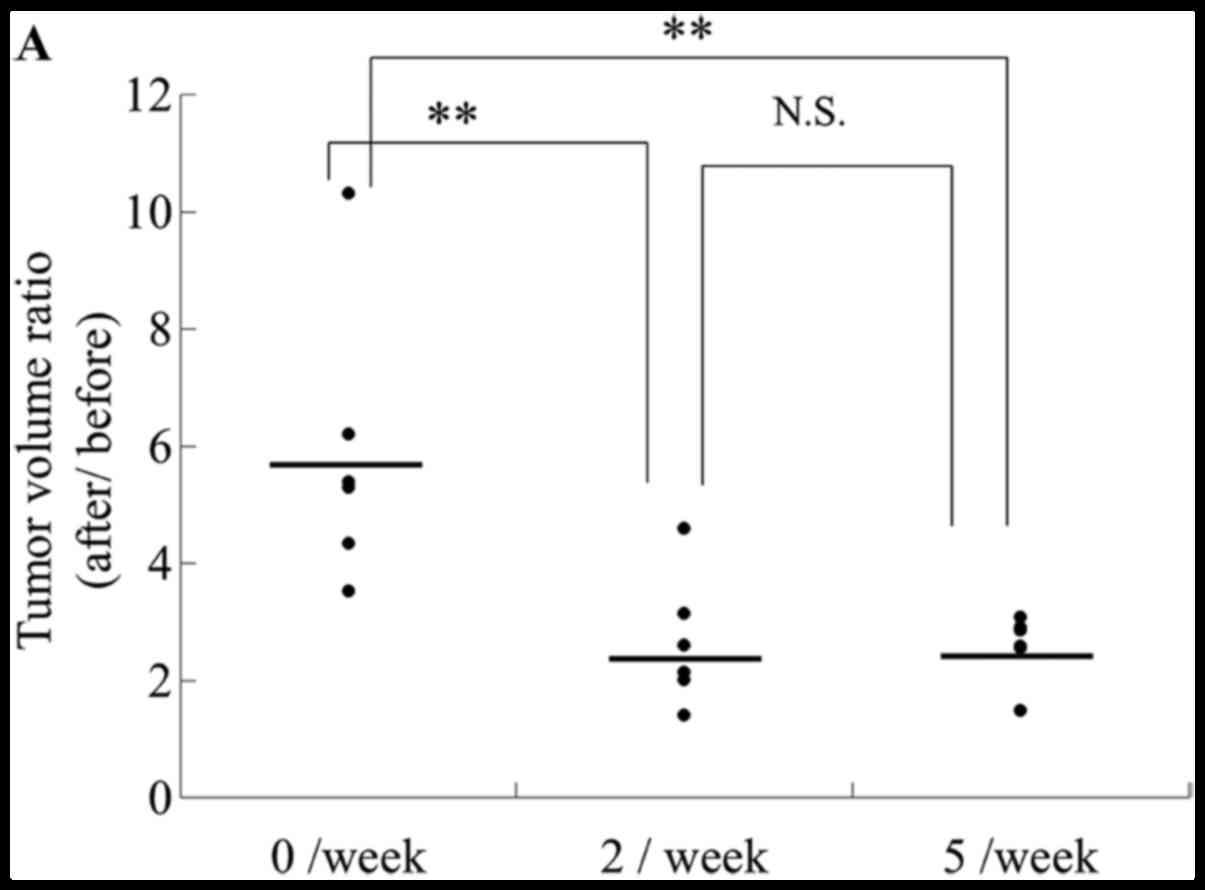
In total, 18 mice with Nara-H cell implantation were randomly divided into three groups of six mice each; one group was a control, whereas the other groups received the treatment twice per week or five times per week. Mice were treated with CO2 for 10 min at the specified frequency for 1 week starting 4 days after cell implantation (Fig. 1A). At the completion of treatment, the ratio of tumor volume after the treatment compared to that before the treatment was calculated.
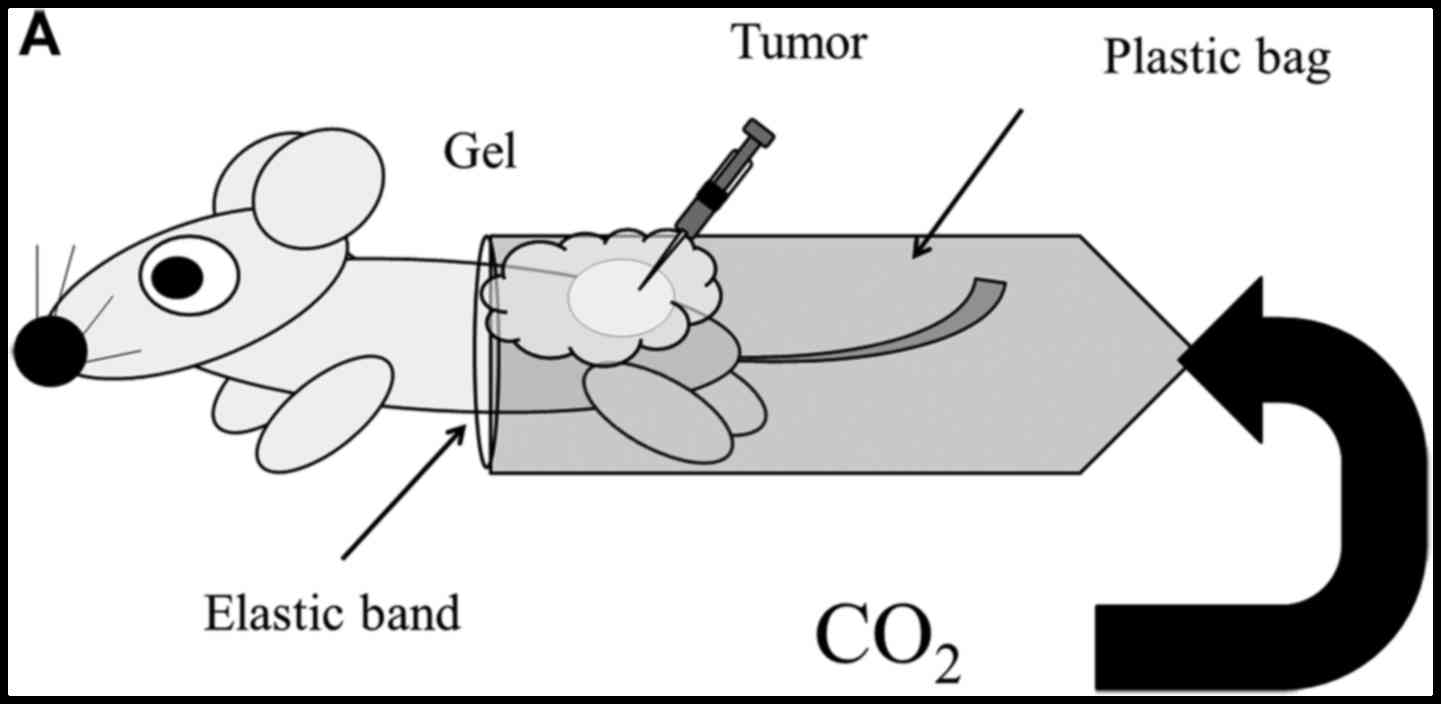
Experimental conditions of CO2 application. (A) General tumor implantation site and CO2 application. (B) Time schedule of CO2 treatment intervals. (C) Tumor implantation into the dorsal subcutaneous area and CO2 application to the ventral area.
To assess the effect of treatment interval, CO2-treatment was performed twice per week for 2 weeks, using two different treatment intervals: 2 and 5 day intervals (2 + 5 interval group) or 3 and 4 day intervals (3 + 4 interval group), as shown in Fig. 1B. For each treatment interval, 18 mice with Nara-H cell implantation were divided into two groups of nine mice each as follows: control group for the 2 + 5 interval (n=9), CO2-treatment group for the 2 + 5 interval (n=9), control group for the 3 + 4 interval (n=9), and CO2-treatment group for the 3 + 4 interval (n=9). At the completion of treatment, the ratio of tumor volume relative to that of the control was calculated.
Effect of treatment application site
We also investigated whether CO2 application had antitumor effects at distant sites. Nara-H cells were implanted into the upper back of 12 mice, and the mice were randomly divided into two groups of six mice each: the control and CO2 groups. After 4 days of cell implantation, treatment with CO2 or air (as control) was applied to the abdominal region, which was a location completely different from that of the implanted tumor (Fig. 1C). CO2-treatment was performed transcutaneously for 10 min each, twice weekly for 2 weeks.
DNA fragmentation assay
DNA fragmentation was evaluated using the APO-Direct kit (BD Biosciences, Franklin Lakes, NJ, USA) according to the manufacturer’s protocol. Briefly, upon completion of the treatments, the implanted tumors were excised, minced, and filtered through a cell strainer (BD Biosciences) to obtain single-cell suspensions. Erythrocytes were lysed in lysis buffer (BD Biosciences), and the remaining cells were pelleted and re-suspended in PBS. Single-cell suspensions were fixed with 1% (v/v) paraformaldehyde and re-suspended in 70% (v/v) ice-cold ethanol at a concentration of 1×106 cells/ml. Each cell pellet was re-suspended in 51 µl of DNA labeling solution, and was incubated for 60 min at 37°C. FITC dUTP-labeled cells were analyzed using a FACS Calibur flow cytometer (BD Biosciences) with a 488 nm argon laser (12,13,18).
Statistical analysis
Analysis of variance with a post-hoc test was performed to compare continuous values. Differences were considered significant at P<0.05. Data are presented as the mean ± standard error (SE). For normally distributed data, the two-tailed t-test was used for comparisons between groups.
Results
CO2 administration for at least 10 min reduces tumor volume
We investigated the optimal CO2 administration time for inhibiting breast cancer, osteosarcoma, and MFH/UPS growth in vivo, using murine xenograft models. CO2-treatment times of 5, 10, or 20 min reduced tumor volume relative to the control group (0 min) in MDA-MB-231 breast cancer and MG63 osteosarcoma mice (P<0.05); however, there were no differences among the three treatment groups using the MDA-MB-231 model (Fig. 2A) or between the 10- and 20-min groups using the MG63 model (Fig. 2B). In the Nara-H MFH/UPS model, a significant difference compared to the control was observed in the 5-, 10-, and 20-min treatment groups, but only at the end of treatment (P<0.05), and there was no significant difference among the groups during the treatments (Fig. 2C). Body weight did not significantly change during the treatments in all mice implanted with any of the cell lines, and there was no evidence of pulmonary metastasis or symptoms of kidney damage such as hematuria (data not shown). These results indicate that CO2 administration has a time-dependent inhibitory effect on breast cancer, osteosarcoma, and MFH/UPS growth in vivo without obvious side effects.
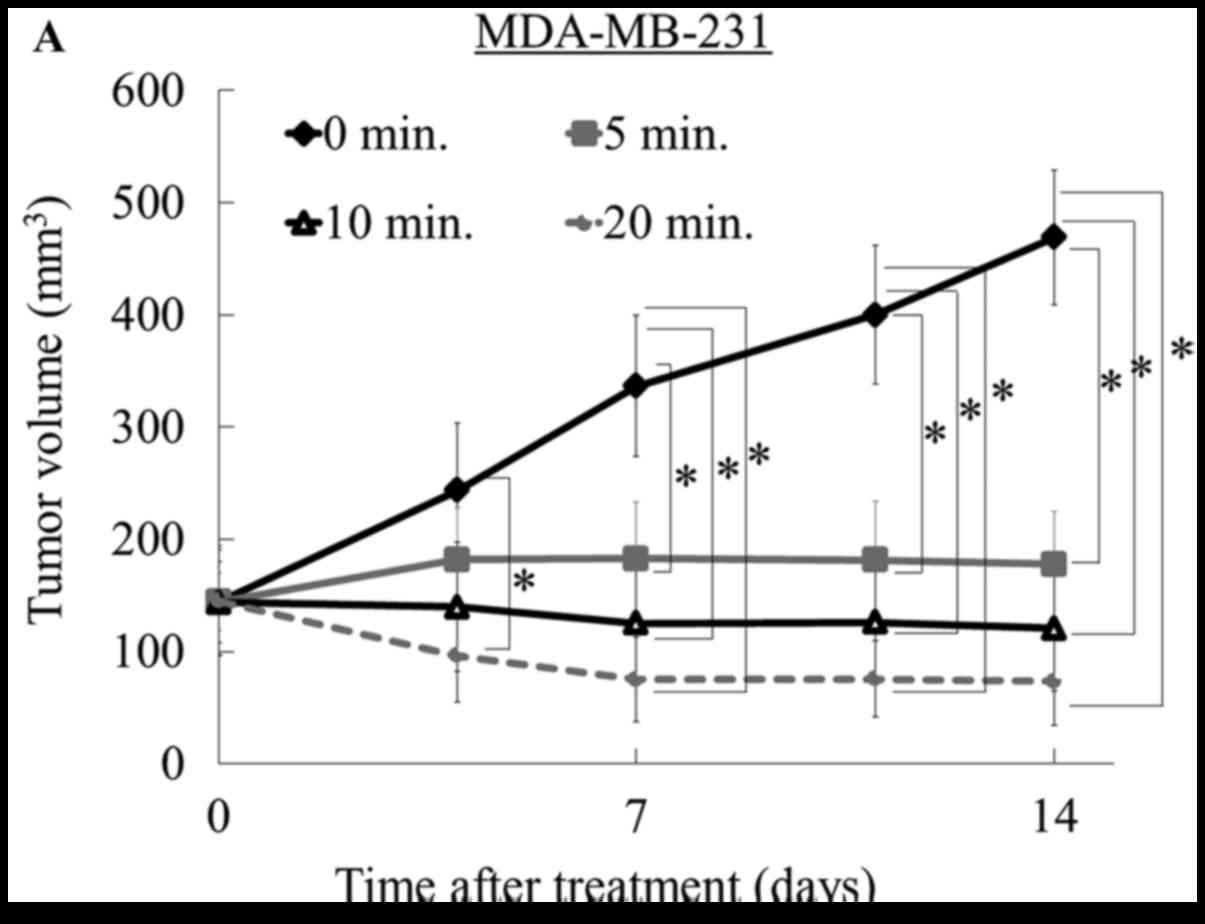
In the current study, the most significant antitumor effect was observed in the MDA-MB-231 breast cancer model. At the end of treatment, all treated tumors in the MDA-MB-231 model were smaller than pre-treated tumors, and notably, two of the six tumors in the 20-min group had disappeared. Similarly, in the osteosarcoma model, tumor volumes in both the 10- and 20-min treatment groups decreased compared to the pre-treatment volume. In contrast, when using the MFH/UPS cell model, the tumor volume was not reduced compared to the pre-treatment volume, although tumor growth was suppressed at all three treatment times relative to that of the control (Fig. 2D and Table I). We assessed the effect of transcutaneous CO2 application on apoptotic activity in the MFH/UPS model and found that CO2-treatment, with all three treatment durations (5, 10, and 20 min), strongly increased the rate of apoptosis, with a greater increase observed with longer treatment durations
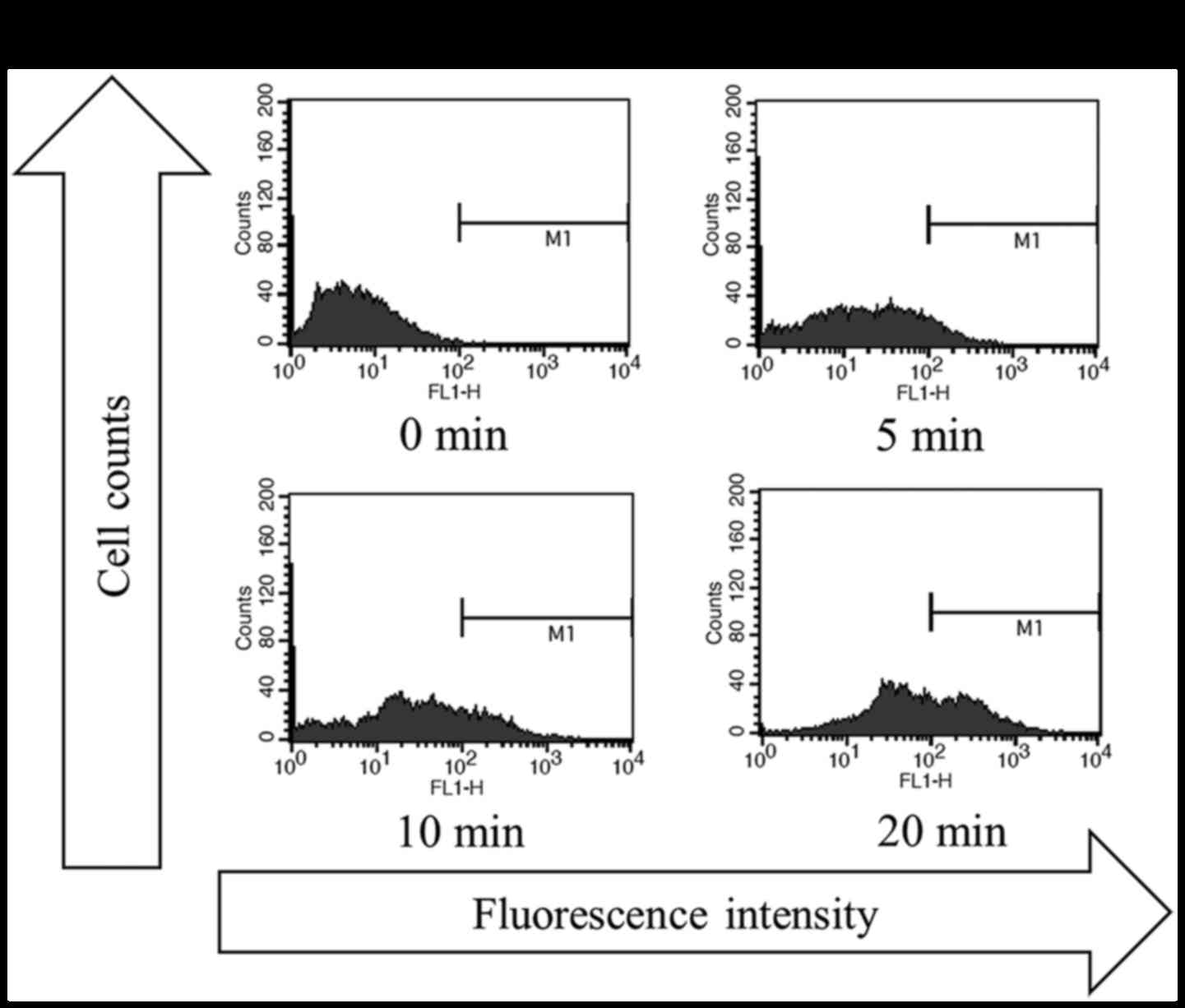
Table I.
Antitumor effect after CO2 application with various treatment durations in each mouse.
Cell line Response 0 min 5 min 10 min 20 min
MDA-MB-231 Reduceda 0/6 2/6 4/6 6/6
(Breast cancer) Lost 0/6 0/6 1/6 2/6
MG63 Reduceda 0/6 2/6 4/6 6/6
(Osteosarcoma) Lost 0/6 0/6 0/6 0/6
Nara-H Reduceda 0/6 0/6 0/6 0/6
(MFH/UPS) Lost 0/6 0/6 0/6 0/6
{ label (or @symbol) needed for fn[@id=’tfn1-or-37-06-3688′] } Effectiveness of transcutaneous CO2 application in reducing the growth of MDA-MB-231, MG63, and Nara-H cell-derived tumors. – a ‘Reduce’ showed before final tumor volume for pre-treatment and ‘Lost’ showed tumor mass disappeared.
Table I. – Antitumor effect after CO2 application with various treatment durations in each mouse.
CO2 administration twice per week at intervals of fewer than 4 days is optimal for inhibiting tumor growth
To determine the optimal frequency of transcutaneous CO2 application, mice were treated with CO2 at a frequency of twice or five times per week. The tumor volumes after treatment twice or five times per week were smaller compared to those of the control mice, and the antitumor effect was not affected by treatment frequency; i.e., the effect was the same regardless of whether the frequency was twice or five times per week (Fig. 4A). These results indicate that transcutaneous CO2 application at twice per week has a significant antitumor effect.
Using a treatment frequency of twice per week, we also evaluated the differences in the antitumor effect according to the treatment interval, i.e., an interval of 2 and 5 days (2 + 5 interval) or 3 and 4 days (3 + 4 interval).
As shown in Fig. 4B, the tumor volume in the 3 + 4 interval group was significantly lower than that in both the control and 2 + 5-interval groups, whereas the volume in the 2 + 5 interval group was not significantly different from that of the control group. These results indicate that the treatment interval of transcutaneous CO2 application should be fewer than 4 days with a treatment frequency of twice per week.
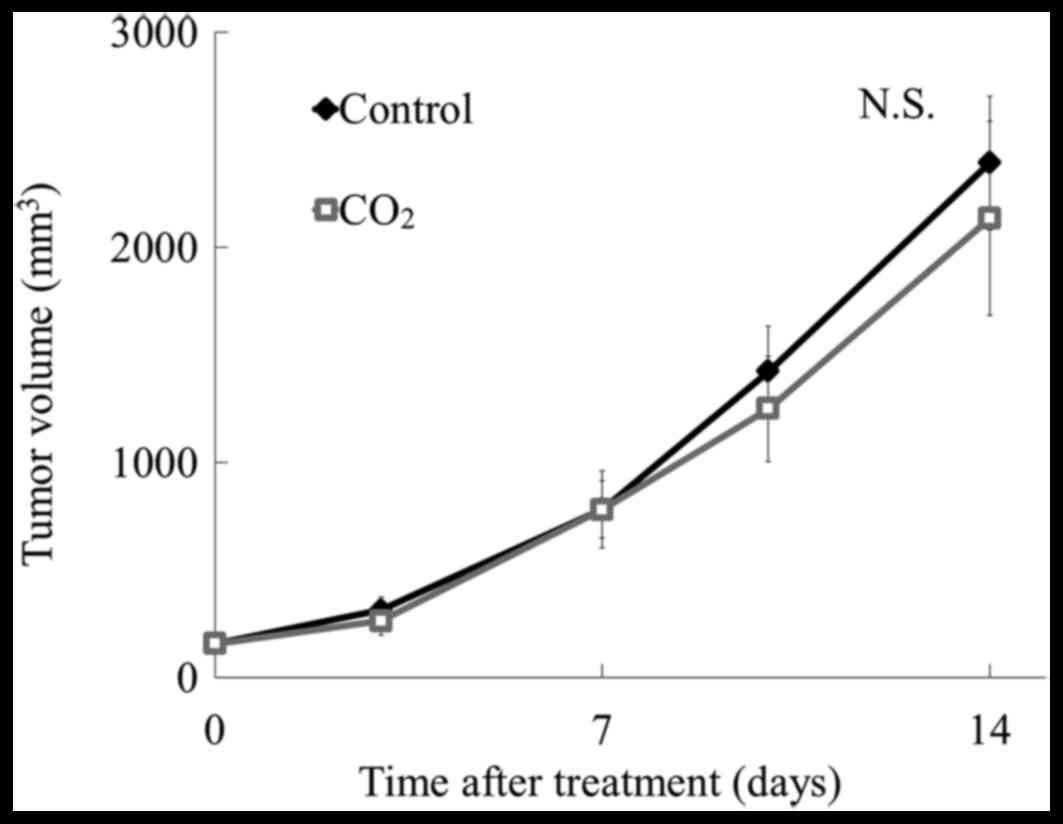
Transcutaneous CO2 exerts an antitumor effect at the site of application
To determine whether transcutaneous CO2 application has local or systemic antitumor effects, tumor cells were injected into the upper back of mice (Fig. 1C), and CO2 was applied to the abdominal region of the body for 10 min, twice per week for 2 weeks. As shown in Fig. 5, there was no reduction in tumor volume with this treatment when compared to that in control mice, indicating that local application of CO2 at the tumor site can induce antitumor effects, but application at a site distant from the tumor cannot induce antitumor effects.
More information: Bailey Surtees et al, Validation of a low-cost, carbon dioxide-based cryoablation system for percutaneous tumor ablation, PLOS ONE (2019). DOI: 10.1371/journal.pone.0207107
Journal information: PLoS ONE
Provided by Johns Hopkins University



{kind=link}