











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Family doctors are in the best position to identify aging patients at risk of frailty early enough to stop – or even reverse – mobility and other function loss, say University of Alberta researchers.
In a recently published study, U of A elder-care specialist Marjan Abbasi, family physician Sheny Khera and their research team recommend primary care physicians check their electronic medical records to identify patients who are at risk of frailty so they can prescribe early intervention.
Frailty is a combination of physical, psychological and social deficits linked to falls, disability, hospital admission and death.
Twenty-five percent of Canadians over age 65 are considered frail, and 50 percent over 80 have the condition.
While it is easy to identify bedridden individuals with end-stage frailty, the best time to start treatment is much earlier, when two or more deficits begin to accumulate, said Abbasi, who is also an associate clinical professor in the Division of Care of the Elderly.
“With mild or even moderate frailty, intervention actually has more impact,” she explained. “As frailty progresses there is increased vulnerability and less reversibility.”
The researchers tested three tools: a walk test, a questionnaire completed by patients, and a 36-point review of the patient’s electronic health record to plot them on an “electronic frailty index.”
They found the review was most convenient for doctors, and thus most likely to be used.
“All the tools were valid and reliable,” said Marjan.
“But our experience indicated the electronic frailty index is going to be more accepted and more feasible.”
In the study, the researchers reported that most frailty identification tools currently in use were developed for research or specialist settings and require additional time, training or specialized equipment to use in a family doctor’s office.
The researchers found that while most family doctors know their patients well, they need an objective tool to help flag the accumulation of early signs of frailty, including hearing loss and foot problems, high blood pressure, osteoporosis and social isolation.
“Primary care has the unique position of seeing people when they are well and helping them to maintain that wellness,” said Khera.
Abbasi said patients respond best when the conversation is framed as a way to maintain their health, rather than stop a decline.
“Patients don’t want to hear about frailty,” she said.
“But if you frame it as what can be done to increase their vitality, then their response is, “OK, what can I do?””
Abbasi and Khera did their research at the Seniors’ Community Hub, which was named the top innovation of 2018 by the Canadian Frailty Network. Started as a pilot program at Covenant Health’s Misericordia Family Medicine Centre with six family physicians, it has now been adopted by the Edmonton Oliver Primary Care Network, where 170 doctors serve more than 200,000 patients.
Abbasi said patients report improvements in their ability to do day-to-day chores, walking speed and mood, and she expects to see a reduction in ER visits and hospital admissions as well.
The model will now be offered to 20 locations across the country, thanks to funding from the Canadian Frailty Network and Canadian Foundation for Healthcare Improvement.
Abbasi and Khera will coach staff at the new clinics and share the best practices they’ve developed at the Seniors’ Community Hub to engage patients in exercise programs, review food intake and streamline medications.
The multidisciplinary team includes primary care physicians, pharmacists, nutritionists, chronic disease management nurses, mental health therapists and kinesiologists, and also connects patients with community resources such as the SAGE Seniors Association.
“I always say, “Don’t ask for more funding, ask for more integration,”” said Abbasi. “We need to make sure the resources that we have are working at their best potential.”
Abbasi and Khera are now working with U of A computer scientists to automate the review of medical records for frailty in Canada.
She said it is standard procedure in Britain, where any patient who scores moderate or higher for frailty triggers an in-depth assessment and intervention.
“Frail people have the most impact on the cost of the health-care system in terms of use of resources,” said Abbasi.
She said early intervention can save both personal and system costs.
“Frailty is associated with aging, but it’s definitely not an inevitable part of aging. You can see people who are 85, 90 years old, still doing exercise, and we have 40- and 50-year-olds who are losing function,” Abbasi said.
“There’s no typical old age.”
Frailty is broadly seen as a state of increased vulnerability and functional impairment caused by cumulative declines across multiple systems.1–4
Frailty has multiple causes and contributors5 and may be physical, psychological, social, or a combination of these. Frailty may include loss of muscle mass and strength, reduced energy and exercise tolerance, cognitive impairment, and decreased physiological reserve, leading to poor health outcomes and a reduced ability to recover from acute stress.6
Overall, frailty exists on a spectrum.7While frailty is often chronic and progressive, it is also dynamic and some patients may be able to improve their frail status.8
Risk Factors
With aging, there is a gradual decline in physiological reserve. However, aging is a complex process; evaluation of frailty and its severity is a better indicator of health status than chronological age. Risk factors for frailty include:
| advanced agepolypharmacy | functional declinepoverty and/or isolation | poor nutrition and/or weight lossmedical and/or psychiatric comorbidity |
Frailty risk and its severity increases with deficit accumulation.9 Physiological reserve may be further decreased by factors such as exacerbation of chronic disease, acute illness, injury, hospitalization, or a change in social supports, leading to increased vulnerability. Consequently, minor stressors may cause a disproportionate change in health status and function.10
Figure 1: Vulnerability of frail older adults to external stressors
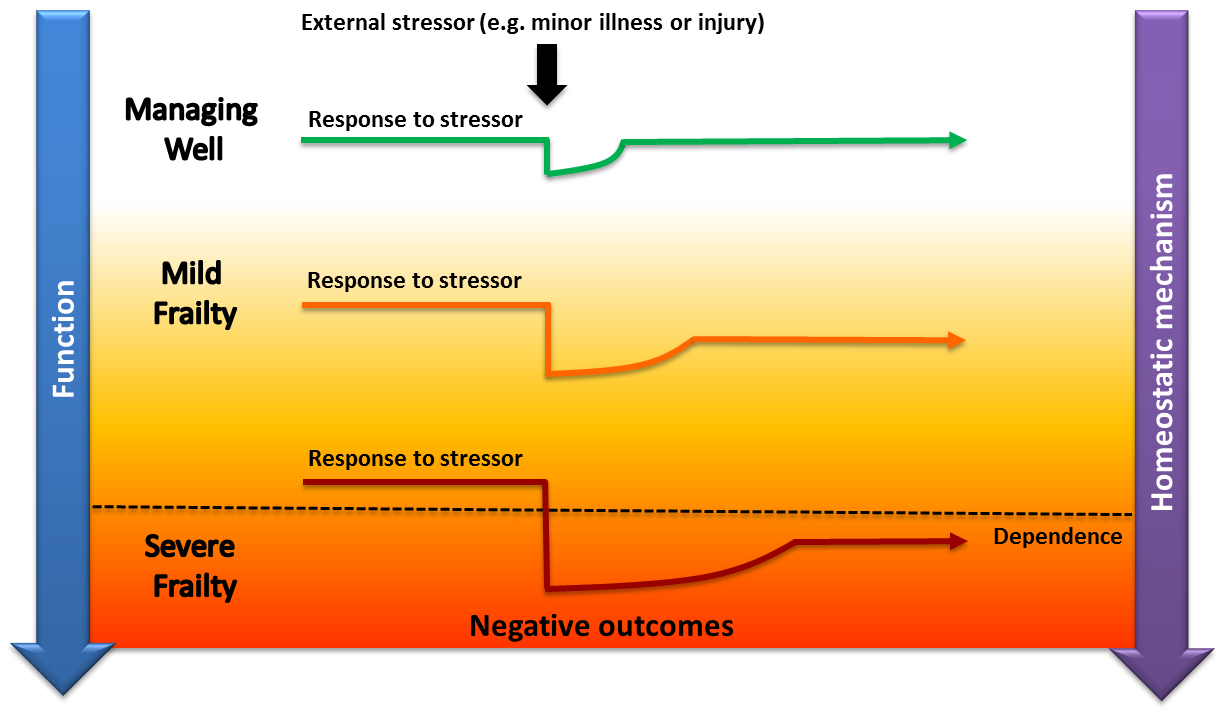
Managing well: A fit older adult who, following a minor stressor, experiences a minor deterioration in function and then returns to homeostasis.
Frailty: A frail older adult who, following a similar stressor, experiences more significant deterioration and does not return to baseline homeostasis. With more severe frailty, this may lead to functional dependency or death.
Adapted from Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. The Lancet. 2013 Mar;381(9868):752-62 & Lang P-O, Michel J-P, Zekry D. Frailty Syndrome: A Transitional State in a Dynamic Process. Gerontology. 2009;55(5):539-49.
Epidemiology
While many adults living in BC remain robust and active as they age, some older adults develop frailty or are vulnerable to frailty. In 2009/10, an estimated 20.4% of British Columbians aged ≥ 65 years living in the community (128,000 people) were frail.4 The prevalence of frailty increases with advanced age (from 16% at ages 65 to 74, to 52% at age 85 and older) and more often affects women than men.4 However, frailty may also be prevalent in younger adults.11 The number of frail older adults in BC will continue to climb as the population ages. Frailty is associated with an increased risk of adverse outcomes and higher utilization of health care services.4,12 A recent meta-analysis found that frailty was associated with increased risk for several negative health outcomes, which are listed in Figure 2.13
Figure 2: Increased risk of negative outcomes associated with frailty13

Early identification of patients with frailty or vulnerable to frailty provides an opportunity to suggest appropriate preventive and rehabilitative actions (e.g. exercise program, review of diet and nutrition, medication review) to be taken to slow, prevent, or even reverse decline associated with frailty.8 Although women are generally at higher risk of frailty, they have a better chance of frailty improvement and lower mortality than men.8
Identification of Patients with Frailty or Vulnerable to Frailty
Routine frailty screening of the general population of older adults is not recommended.7 Instead, use a case finding approach to identify patients with frailty, particularly in older adults who regularly or increasingly require health and social services (e.g. emergency room visits, ambulance crew attendance, adult day clinics, hospitalization, home support, referral to residential care).7
Encounters with health and social care professionals present an opportunity to identify older adults with frailty or vulnerable to frailty and take steps to reduce or manage associated risks.7,14–18
Signs and Symptoms
Use a diligent case finding approach to identify warning signs of frailty. Older adults may have a number of non-specific concerns that may suggest frailty or vulnerability to frailty. In addition to the review of chronic conditions, some other areas to assess are noted in Table 1 below. Observed changes or concerns expressed in these areas may be early warning signs of frailty, while a combination of impairments may signal progression towards frailty.There are certain signs and symptoms (e.g. falls, delirium, immobility) that may raise a higher level of suspicion that the patient has frailty7 – see Table 1. However, these problems may have causes other than frailty, so it is important to conduct a further review.
Table 1: Possible warning signs of frailty1,7,15,19,20
Signs indicated with bold * may raise a higher level of suspicion of frailty.
| Medical:unintentional weight loss* (esp. if ≥ 10lbs/4.5kg over past year)incontinence*loss of appetiteloss of muscle/strength (sarcopenia)osteoporosisimpaired vision/hearingchronic painrepeated ER visits/hospitalization Psychological:delirium*cognitive impairment/dementia*depressionirrational fears/concernsinappropriate behaviourirregular sleep patterns | Functional:declining functional status*immobility*recent fall(s)*, fear of fallingimpaired balancefatigue or loss of energyreduced physical activity/endurance Medications and alcohol:susceptibility to medication side effects*polypharmacy related issuesincreased alcohol consumption Social and environmental:social isolationtransition in living circumstanceschange in family/caregiver supportcaregiver stress |
Frailty Scoring Tools
Patients with more severe frailty or certain geriatric syndromes may be easily identified. However, identifying mild or early stage frailty may require a formal assessment – consider confirming clinical suspicion of frailty with a scoring tool.
Dozens of different frailty measures have been developed over the years, but there is no single measure that is viewed as the gold standard21 and many are not well adapted for the busy primary care setting.22 The tools in Table 2 are recommended for community-based primary care.23
Table 2: Recommended frailty scoring tools for community-based primary care
| Tool | Frailty suggested by: | These tests, including scoring information, are available in the Associated Documents section below. | |
| General | PRISMA-7 Questionnaire | Score ≥ 37 | |
| Mobility | Gait Speed Test | Time > 5 seconds over 4m7 | |
| Timed Up and Go Test (TUG) | Time > 10 seconds7 | ||
| Cognitive Impairment | Standardized Mini Mental State Exam (SMMSE) | See Guidelines.ca: Cognitive Impairment – Recognition, Diagnosis and Management in Primary Care | |
| Montreal Cognitive Assessment (MoCA) | |||
| Other tests, as appropriate |
Any one of the above tools may suggest frailty. Cognition and mobility tests are best done in the outpatient setting when patients are at their clinical baseline.
Comprehensive Assessment of Patients with Frailty
Patients with identified frailty require additional assessment to support the development or refinement of a care plan. The gold standard for assessing and managing frailty in older adults is comprehensive geriatric assessment:7 an interdisciplinary process that evaluates medical, psychological, social and functional domains of older adults with frailty to develop a detailed care plan for treatment, support and follow-up.24 However, comprehensive geriatric assessment by medical specialists in geriatric care is resource intensive – see Indications for Referral below.
Many patients with frailty can be assessed and managed in the primary care setting through a network of support, which may include family, caregivers, and community care providers. Ensure patients and caregivers are referred to or connected with local health care and social services, such as those available to eligible patients through Home and Community Care within local health authorities.
Areas of Assessment
There are number of common problems associated with frailty such as falls, weight loss, poor nutrition, physical inactivity, cognitive impairment and polypharmacy—many of which may be reversible or preventable—that should be addressed to improve outcomes.
Conduct a review of the medical, functional, psychological and social/environmental needs of the patient.7 The areas of geriatric assessment outlined in Table 3 in the Management section below and the Appendix B: Sample Care Plan Template may help guide assessment.
For patients with frailty who have multiple health concerns, consider using “rolling” assessments over multiple visits, targeting at least one area of concern at each visit.25
Family physicians may be eligible for Complex Care incentive fees, which offer additional compensation to family physicians for the management of patients with complex conditions, including moderate or severe frailty, or for Chronic Disease Management incentive fees. See the Resources section below and www.gpscbc.ca: Billing Guides.

Grading Severity of Frailty
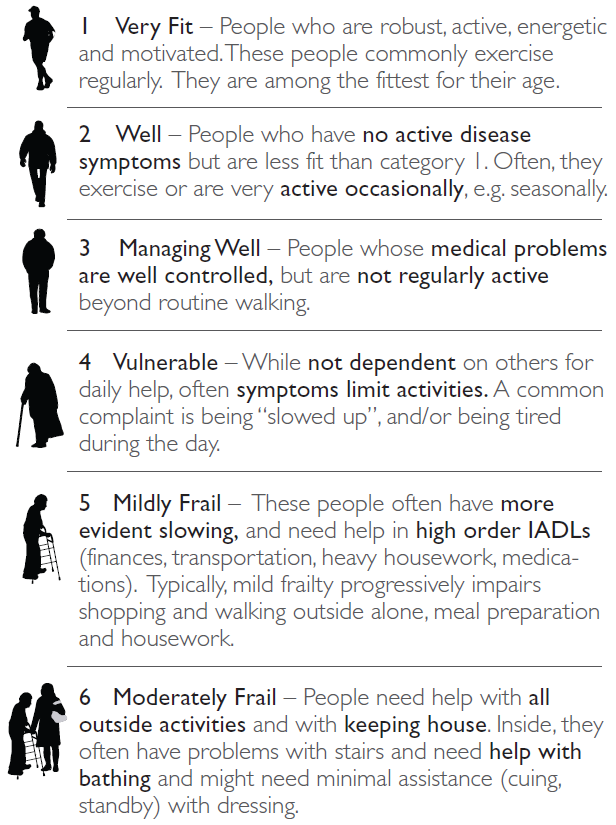
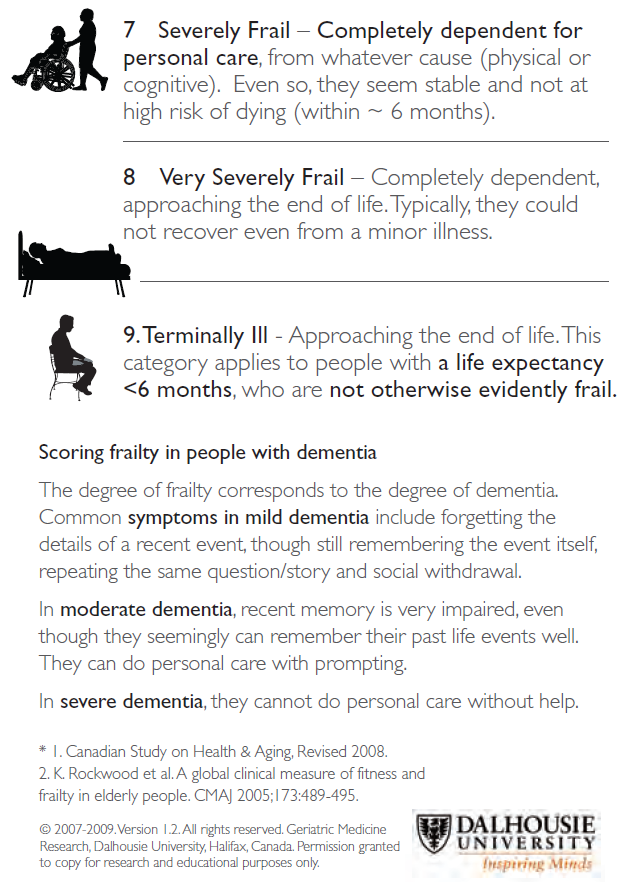
Once a patient is identified as frail or vulnerable to frailty, it is recommended that the Clinical Frailty Scale be used to categorize the needs of the patient. The Clinical Frailty Scale is a validated tool that uses clinical information to stratify patients with frailty based on their level of vulnerability. The Clinical Frailty Scale is a strong predictor of institutionalization and mortality2 and is useful for consistently communicating frailty status between care providers.
Figure 3: Clinical Frailty Scale2
More information: Marjan Abbasi et al. Identification of Frailty in Primary Care: Feasibility and Acceptability of Recommended Case Finding Tools Within a Primary Care Integrated Seniors’ Program, Gerontology and Geriatric Medicine (2019). DOI: 10.1177/2333721419848153
Provided by University of Alberta



{kind=link}