










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



For the first time, Northwestern Medicine scientists have pinpointed the location of dysfunctional brain networks that lead to impaired sentence production and word finding in primary progressive aphasia (PPA), a form of dementia in which patients often lose their language rather than their memory or thought process.
With this discovery, the scientists have drawn a map that illustrates three regions in the brain that fail to talk to each another, inhibiting a person’s speech production, word finding and word comprehension.
For example, some people can’t connect words to form sentences, others can’t name objects or understand single words like “cow” or “table.”
The map can be used to target those brain regions with therapies, such as transcranial magnetic stimulation (TMS), to potentially improve an affected person’s speech.
“Now we know where to target people’s brains to attempt to improve their speech,” said lead author Dr. Borna Bonakdarpour, assistant professor of neurology at Northwestern University Feinberg School of Medicine’s Cognitive Neurology and Alzheimer Disease Center and a Northwestern Medicine neurologist.
PPA occurs in patients with neurodegenerative disorders, including Alzheimer’s disease and frontotemporal degeneration.
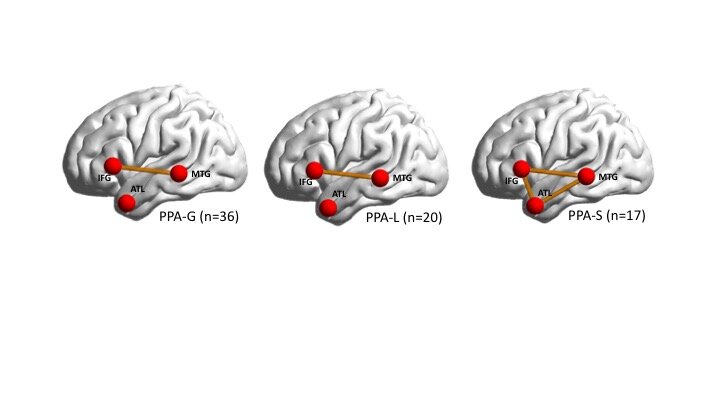
Interactions among three main regions in the brain is responsible for how people process words and sentences.
PPA occurs when there is a lack of connectivity among these areas.
Different patterns of connectivity failure among these regions can cause different subtypes of PPA.
The findings will be published Sept. 1 in the journal Cortex.
The large study (73 patients) recruited from the extensive pool of patients with PPA at Northwestern’s Cognitive Neurology and Alzheimer Disease Center, one of the largest centers in the world.
The study used functional MRI, which monitors brain activity by detecting blood flow, to locate the regions of the brain that are talking to each other or not.
That cannot be shown with structural MRI.
Previous research used structural MRI to locate only regions of the brain that had atrophied, and scientists did not clearly know how physiological impairment in these regions correlated with symptoms a patient was experiencing.
This study is novel because it examined brain regions that were still functional (had not atrophied) and focused on the networks among the functional regions to see if they were connecting or not.
This allowed the scientists to correlate the functional areas in the brain with symptoms of patients with PPA.
“Previous studies of structural changes in the brain were like archeology, in which scientists were locating areas of the brain that had already died,” Bonakdarpour said.
“But we are looking at the parts of the brain that are still alive, which makes them much easier to target with treatment.”
Bonakdarpour and his colleagues have begun testing TMS on the three targeted brain regions in healthy individuals with the goal of applying it to patients with PPA in a future clinical trial.
Journal information: Cortex
Provided by Northwestern University
Primary progressive aphasia (PPA) is a clinical syndrome characterized by speech and language impairment caused by neurodegeneration of language networks. In 1892, Pick [1] reported the case of a 71-year-old man who presented with nonsensical speech, anomia, dyslexia, dysgraphia, personality changes, and memory impairment. Apart from a few reports of Gogi aphasia in Japan in the 1940s [2], discussion of neurodegenerative aphasia remained dormant until the 1970s when British investigators published several cases with progressive semantic loss, semantic dementia [3,4], and Mesulam and colleagues first introduced the term PPA [5]. In 1996, Grossman et al. [6] also introduced the term progressive nonfluent aphasia to describe patients with progressive loss of speech fluency. PPA was initially described as a unitary syndrome with anomia as main symptom but this view did not explain the spectrum of presentations described. Furthermore, many patients did not show the typical features of semantic or nonfluent presentations; it was later clarified that most of these patients have a third PPA subtype, named the logopenic variant of PPA [7]. In 2011, an international group of experts introduced a common framework in which PPA was classified into three different variants, based on specific cognitive and neuroimaging features: semantic (svPPA), nonfluent/agrammatic (nfvPPA), and logopenic variants (lvPPA) [8]. Recent clinicopathological studies demonstrated that each variant is associated with different probabilities of neuropathological changes and, rarely, genetic mutations. Table 1 presents the 2011 PPA classification, including the diagnostic algorithm allowing for three diagnostic levels: clinical, imaging-supported, and definite diagnosis.
Table 1.
Primary progressive aphasia 2011 diagnostic consensus criteria algorithm
| PPA clinical diagnostic criteria | |||
| Inclusion criteria | |||
| (1) Most prominent clinical feature is difficulty with language | |||
| (2) Aphasia should be the most prominent deficit at symptom onset and for the initial phases of the disease | |||
| (3) These deficits are the principal cause of impaired daily living activities | |||
| Exclusion criteria | |||
| (1) Pattern of deficits is better accounted for by other nondegenerative nervous system or medical disorders | |||
| (2) Cognitive disturbance is better accounted for by a psychiatric diagnosis | |||
| (3) Prominent initial episodic memory, visual memory, and visuoperceptual impairments | |||
| (4) Prominent initial behavioural disturbance | |||
| Nonfluent/Agrammatic variant PPA | Semantic variant PPA | Logopenic variant PPA | |
| Clinical diagnosis | Core features: (at least 1) (1) Agrammatism in language production (2) Effortful, halting speech with inconsistent speech sound errors and distortions (apraxia of speech) Supporting features: (at least 2) (1) Impaired comprehension of syntactically complex sentences (2) Spared single-word comprehension (3) Spared object knowledge | Core features: (both) (1) Impaired confrontation naming (2) Impaired single-word comprehension Supporting features: (at least 3) (1) Impaired object knowledge, particularly for low frequency or low familiarity items (2) Surface dyslexia or dysgraphia (3) Spared repetition (4) Spared speech production (grammar and motor speech) | Core features: (both) (1) Impaired single-word retrieval in spontaneous speech and naming (2) Impaired repetition of sentences and phrases Supporting features: (at least 3) (1) Speech (phonologic) errors in spontaneous speech and naming (2) Spared single-word comprehension and object knowledge (3) Spared motor speech (4) Absence of frank agrammatism |
| Imaging supported diagnosis (both present) | (1) Clinical diagnosis of nfvPPA | (1) Clinical diagnosis of svPPA | (1) Clinical diagnosis of lvPPA |
| (2) Imaging: (at least 1) | (2) Imaging: (at least 1) | (2) Imaging: (at least 1) | |
| (a) Predominant left posterior frontoinsular atrophy on MRI | (a) Predominant anterior temporal lobe atrophy on MRI | (a) Predominant left posterior perisylvian or parietal atrophy on MRI | |
| (b) Predominant left posterior frontoinsular hypoperfusion or hypometabolism on SPECT or PET | (b) Predominant anterior temporal hypoperfusion or hypometabolism on SPECT or PET | (b) Predominant left posterior perisylvian or parietal hypoperfusion or hypometabolism on SPECT or PET | |
| PPA with definite diagnosis | Clinical diagnosis fulfilled | ||
| AND | |||
| (1) Histopathologic evidence of a specific neurodegenerative disorder (e.g. FTLD-tau, FTLD-TDP, AD, other) | |||
| OR | |||
| (2) Presence of a known pathogenic mutation |
Adapted with permission from [8,9]. AD, Alzheimer’s disease; FTLD-tau, frontotemporal lobar degeneration-tau; FTLD-TDP, frontotemporal lobar degeneration–TAR DNA-binding protein; lvPPA, logopenic variant primary progressive aphasia; nfvPPA, nonfluent/agrammatic primary progressive aphasia; PPA, primary progressive aphasia; svPPA, semantic variant primary progressive aphasia.
This article focuses on describing the updated clinical and neuroimaging features of the three main PPA variants. We then summarize pathological and genetic findings and finally discuss the role of PPA in furthering the scientific understanding of neurodegenerative diseases.
SEMANTIC VARIANT PRIMARY PROGRESSIVE APHASIA
The first three cases of this syndrome were described by Warrington [3] in 1975. Patients suffered from loss of word and object knowledge, and deficits were typically most severe for low frequency and low familiarity items [8].
Symptoms included poor performance in confrontational naming, single word comprehension, and object and face identification tasks. Later work by Snowden et al. [4] and Hodges et al. [10] further demonstrated that semantic loss also leads to surface dyslexia, a disorder in which patients can read pseudowords but not exceptionally spelled words.
Typical reading errors include ‘regularization’ errors in irregular words, such as ‘yacht’ or ‘island’ are pronounced as ‘yachdt’ and ‘is-land’ [10].
SvPPA patients often produce semantic paraphasias and tend to substitute specific, subordinate (in the semantic hierarchies) words with generalized terms, such as replacing ‘screwdriver’ with ‘thing’ and ‘panther’ with ‘animal.’ For a decade, it was unclear whether semantic dementia and ‘fluent PPA’ were different entities [11].
In 2004, Gorno-Tempini et al. [7,8] included semantic dementia as one of the three PPA variants and the term semantic variant PPA (svPPA) was later adopted by the international workgroup. This new classification of svPPA includes the key classic features of semantic dementia, such as anomia and word comprehension deficits. Supporting diagnostic features include surface dyslexia or dysgraphia, impairment in object or face knowledge, and relatively spared repetition and speech production abilities [8].
Further reports described deficits in different categories of objects and stimuli modalities, such as famous faces [12], voices [12], nonverbal environmental sounds [13], smells [14], and taste stimuli [15], sometimes in relation to greater right ATL damage.
In general, the hallmark feature of this disorder is an inability to identify the meaning of stimuli despite preserved perception. As svPPA progresses, behavioural symptoms including lack of empathy, changes in personality, disinhibition, mental inflexibility, and compulsive behaviours commonly occur [16].
In addition to different clinical symptoms, the three main PPA variants show distinct neuroimaging features [8].
The different patterns of neuroanatomical changes in each subtype are determined by the selective vulnerability of certain brain networks to the neurodegenerative disorders that cause neuronal damage [8,17].
Damage to the ATL in svPPA is identified as atrophy on volumetric brain imaging (MRI) or as hypometabolism on fluorodeoxyglucose (FDG)-PET (Fig. 1). The ATL damage is most often greater in the left hemisphere, which is consistent with naming, word comprehension, and reading difficulties [10,18], but in roughly 30% of svPPA cases, atrophy is more severe in the right ATL [19,20].
Individuals with greater right ATL atrophy present initially with difficulty identifying familiar people, recognizing facial expressions, and with behavioural abnormalities, such as loss of empathy and compulsive, repetitive behaviours [19–21]. Structural connectivity analysis demonstrated severe damage to ventral white matter tracts, typically the anterior portion of the inferior longitudinal fasciculi (ILF) and uncinate fasciculi [22,23] (Fig. 2).
Task-free fMRI studies show that focal ATL damage causes decreased functional connectivity and functional changes in a widespread semantic network including modality-specific primary and association cortices [24,25]. Magnetoencephalography (MEG) study shows hyposynchrony of alpha and beta frequencies in the left temporoparietal junction, also suggesting that functional disruption areas expand beyond atrophic regions [26].
r people, recognizing facial expressions, and with behavioural abnormalities, such as loss of empathy and compulsive, repetitive behaviours [19–21].
Structural connectivity analysis demonstrated severe damage to ventral white matter tracts, typically the anterior portion of the inferior longitudinal fasciculi (ILF) and uncinate fasciculi [22,23] (Fig. 2).
Task-free fMRI studies show that focal ATL damage causes decreased functional connectivity and functional changes in a widespread semantic network including modality-specific primary and association cortices [24,25]. Magnetoencephalography (MEG) study shows hyposynchrony of alpha and beta frequencies in the left temporoparietal junction, also suggesting that functional disruption areas expand beyond atrophic regions [26].

Grey matter atrophy patterns in patients with three main primary progressive aphasia variants versus controls. Presented here are statistical parametric maps that depict the grey matter atrophy patterns in semantic variant PPA (svPPA, n = 58), nonfluent/agrammatic variant PPA (nfvPPA, n = 40), and logopenic variant PPA (lvPPA, n = 24) compared with control groups that are matched for age, sex, scanner and sample size. Voxel-based morphometry results thresholded are set at a family-wise error rate of P < 0.001. FWE, familywise error rate; PPA, primary progressive aphasia. Reproduced with permission from [88].

White matter damage in the three main primary progressive aphasia variants versus controls. (a) The average mean diffusivity values for left superior longitudinal fasciculus (SLF), inferior longitudinal fasciculus (ILF), uncinate fasciculus (UNC) in all three PPA variants when compared with healthy controls on a standard MNI (Montreal Neurological Institute of McGill University Health Centre) brain template. The asterisk symbol (m) indicates statistical difference from normal controls with P value less than 0.05. The colour bar represents the average mean diffusivity values, ranging from low (violet-blue) to high values (yellow-red). Mean diffusivity is measured in 10−3mm2 s−1. (b) The average mean diffusivity values for arcuate fasciculus (AF), frontoangular SLF (SLF-II), frontosupramarginal SLF (SLF-III), and temporoparietal SLF (SLF-tp) in all three PPA variants when compared with healthy controls on a standard MNI (Montreal Neurological Institute of McGill University Health Centre) brain template. The asterisk (m) indicates statistical difference from normal controls with P value less than 0.05. The colour bar represents the average mean diffusivity values, ranging from low (violet-blue) to high values (yellow-red). Mean diffusivity is measured in 10−3 mm2 s−1. Reproduced with permission from [21].
SvPPA is most often associated with frontotemporal lobar degeneration-TAR DNA-binding protein 43 (FTLD-TDP 43) type C disorder [27].
Consistently, recent molecular PET imaging show that amyloid deposition is uncommon in svPPA especially under 60 years of age [28▪▪] and CSF abeta and tau studies are usually negative [29]. [18F]AV1451 PET designed to specifically target tau shows ATL binding in svPPA, raising concerns regarding the specificity of this ligand to tau [30▪].
As the disease progresses, anatomical damage extends to connected brain regions in the posterior temporal lobes, contralaterally to the initially less involved ATL and anteriorly to orbitofrontal regions [20].
Consistently semantic and language impairments become more generalized, although islands of fluency might remain and can be useful for differential diagnosis later in the disease course.
Typically, patients develop more prominent behavioural symptoms, whereas motor functions are usually spared until the final stages, unless svPPA is associated with motor neuron disease [31].



{kind=link}