









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Researchers at the Complutense University of Madrid (UCM) have identified changes in retinal layer thickness, inflammation or thinning in patients with mild Alzheimer’s disease, confirming that the retina is one of the most important biomarkers for early diagnosis of the disease.
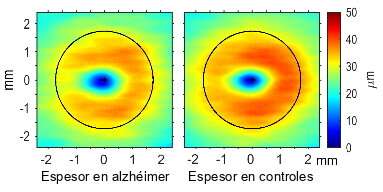
For the first time, researchers have determined the shape and size of the areas that present significant thinning in each retinal layer, which tend to occur in the same locations.
They also observed that in some patients already diagnosed with Alzheimer’s disease, the retinal layers presented neurodegeneration, whereas in others they presented neuroinflammation, the stage prior to neurodegeneration, a finding which can be used to diagnose the disease before other tests.
“The novelty of our results is that in the early stage of the disease represented by our patient sample, neural layer thinning systematically predominated over thickening, as regards both percentage of thinned surface and neural volume lost,” announced Luis Jáñez, a researcher at the Knowledge Technology Institute at the Complutense University of Madrid and first author of the study.
The results of this investigation, which have recently been published in Scientific Reports, confirm that due to the retina’s features in common with the brain and accessibility using non-invasive techniques, it constitutes one of the most important and promising biomarkers for further study of this complex neurodegenerative disease.
“In recent years, ground-breaking studies have used the eyes as a window onto the brain to detect the changes that occur during the early stages and progression of Alzheimer’s disease,” explained Elena Salobrar-García, a scientist at the Ramon Castroviejo Ophthalmology Research Institute at the Complutense University of Madrid and co-author of the study.
The macular zone is the first to present changes
Researchers at the Knowledge Technology Institute and the Ramon Castroviejo Ophthalmology Research Institute – both at the Complutense University – have developed new techniques and analytical tools that have enabled them to confirm that “the first changes appear in the macular zone, which is the most sensitive area and controls central vision and colour perception,” noted José Manuel Ramírez, director of the Ramon Castroviejo Institute.
The study was conducted with a group of 19 patients selected from 2124 clinical histories at the San Carlos Hospital Clinic Geriatric Service in Madrid.
These patients had very early stage Alzheimer’s disease and did not present any other disease that affected the retina. The study also included a control group comprising 24 volunteers similar in age and other characteristics but without any relevant disease.
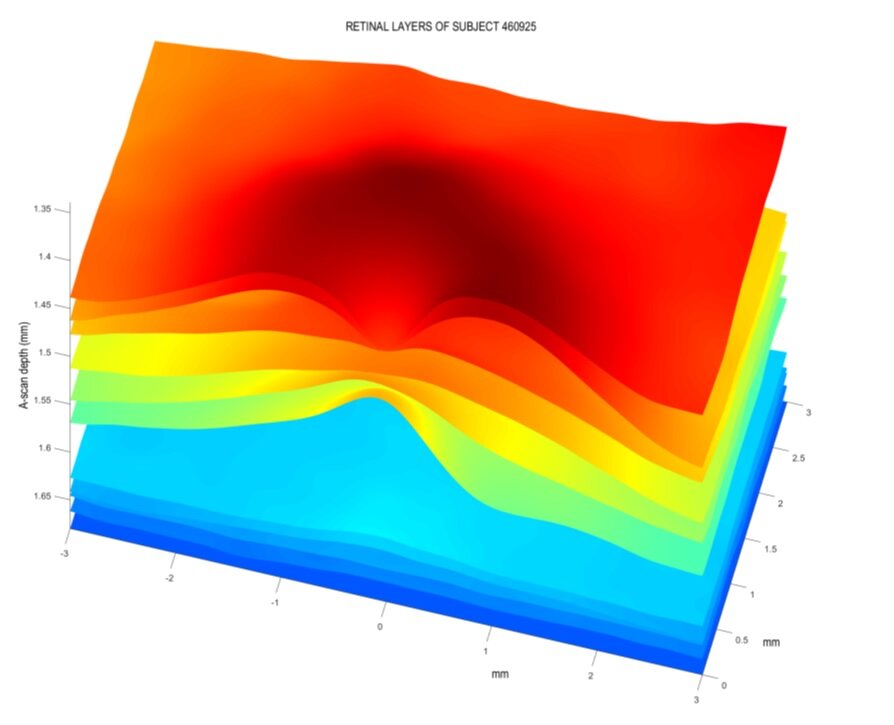
A three-dimensional image of a square region measuring 6×6 mm was obtained for each participant’s retina, using optical coherence tomography (OCT).
“With OCT, a light beam can sweep this area of the retina in 2.5 seconds. This frequently used technique is non-invasive, very fast and low-cost,” Salobrar indicated.
Afterwards, using software designed specifically for this study, the thickness of each retinal layer was measured at 262,144 points distributed over a grid of 512 columns and as many rows.
“Using statistical techniques based on Gaussian random field theory, we determined for the first time the exact shape, size and location of the areas affected by the disease in each retinal layer,” added Jáñez.
In order to compare changes in thickness in different layers, the researchers developed software capable of performing exact arithmetic operations with the huge whole numbers generated by combining the hundreds of thousands of points sampled in each layer.
“The results of our study represent a breakthrough for the diagnosis and follow-up of Alzheimer’s disease and confirm that the retina is a good biomarker,” the researchers concluded.
Optical coherence tomography (OCT) has transformed the diagnosis and treatment of ocular disease. Currently, OCT is one of the most widely used ophthalmic decision-making technologies [1].
OCT uses retroreflected light to provide micron-resolution, cross-sectional images of biological tissues.
The first experimental OCT device developed to image the human retina in vivo was introduced in 1991 [2].
OCT has become a compelling medical imaging technology, particularly in ophthalmology, as it allows achieving the cross-sectional structure of the retina and anterior eye with higher resolutions than any other non-invasive imaging modality [2].
Even commercially available OCT systems exhibit extremely high resolution, typically in the micrometer-scale resolution; and the resulting images can be analyzed both qualitatively and objectively.
The recent introduction of OCT angiography (OCTA) and wide-field imaging in clinical practice has led to significant advancements in retinal disease understanding and treatment [1].
Further developments of OCT technology may impact eye disease diagnosis and improve the management of the major clinical and public health problems associated with visual impairment.
Also, there is growing evidence to incorporate the OCT technology into clinical settings managing cerebrovascular and neural diseases [3].
Alzheimer’s disease (AD) is the most prevalent chronic neurodegenerative disorder and the cause of dementia in the elderly [4].
The global prevalence of AD is 36 million people and is estimated to double every 20 years, reaching 115 million in 2050 [5].
The pathologic findings typical for AD are beta-amyloid (Aβ) plaques, neurofibrillary tangles (NFTs), and reactive gliosis [6]. Recent studies have shown that AD initiates decades before it is clinically expressed [7,8,9,10,11,12].
Therefore, it could be possible to identify individuals who will develop AD before the early symptoms appear, and potentially to employ prevention in high-risk patients [4,5,7,8,9,10,11,12].
In clinical practice, the diagnosis of AD is based on cognitive evaluation; such an approach might be insufficient in individuals with much brain or cognitive reserve.
Also, evaluation of brain biochemistry and anatomy using molecular markers or neuroimaging modalities are not surrogates for cognitive processing, nor psychological function.
Currently used diagnostic techniques, which include neuroimaging (e.g., magnetic resonance imaging (MRI) and positron emission tomography (PET)) or cerebrospinal fluid protein levels (e.g., tau and Aβ), are costly or relatively invasive.
Also, these techniques present low specificity and are not readily accessible to the majority of clinicians and patients.
As the eye and brain share critical structural and pathogenic pathways, a non-invasive multivariate biomarker methodology using the eye may provide new insights into the onset and progression of AD.
The link between eye pathology and AD has been established.
In patients with AD, the visual function is commonly affected; symptoms include loss of best-corrected visual acuity, a reduction in contrast sensitivity, ocular motility abnormalities, and color vision defects [13].
It is known that the most likely locations for AD onset are parahippocampal regions, the entorhinal cortex, and hippocampus [14].
Interestingly, McKee et al. found dense AD pathology in the visual association cortex Brodmann area 19 in some cognitively intact individuals with preclinical AD, with the absence of significant pathology in the hippocampus or entorhinal cortex [15].
It was hypothesized that area 19 might confer enhanced vulnerability to neurodegeneration [15].
Recently, advances in neuro-electrophysiological tests and optical imaging have made it possible to detect specific manifestations of neurodegenerative diseases in the eye; in particular, retinal microvascular alterations with abnormal bioelectrical activity of retinal ganglion cells, photoreceptors, and the optic nerve have been associated with cognitive decline and brain alterations in relation to aging and brain abnormalities in early AD [16,17].
Also, evidence of ganglion cell loss and photoreceptor damage observed in AD patients has been reported using OCT [16,17]. Not only retinal but also choroidal thickness was found to be reduced in enhanced depth SD-OCT studies [18,19].
Based on the evidence mentioned above, researchers have even suggested that if an association can be made between the amyloid in the brain and particular manifestations in the eye, then it would be feasible to diagnose AD by a specific eye examination.
This review will highlight recent insights into measuring retinal structure in patients with AD and the identification of retinal biomarkers using commercially available OCT devices.
OCT may offer an opportunity to improve the understanding of the neurobiological changes in neurodegenerative diseases such as AD and may aid to develop both diagnostic and prognostic biomarkers that can predict clinical progress.
A mounting body of evidence suggests that disturbances in retinal blood flow and structure are related to cognitive function, which can severely impair vision.
The OCT technology may allow researchers and physicians to gain deeper insights into retinal morphology and clarify the impact of AD on retinal health and function. This review will also focus on the challenges and opportunities associated with the applications of OCT technology to identify AD’s biomarkers in the eye.
More information: Luis Jáñez-Escalada et al, Spatial analysis of thickness changes in ten retinal layers of Alzheimer’s disease patients based on optical coherence tomography, Scientific Reports (2019). DOI: 10.1038/s41598-019-49353-0
Journal information: Scientific Reports
Provided by Universidad Complutense de Madrid



{kind=link}