









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



People with persistent back pain or persistent headaches are twice as likely to suffer from both disorders, a new study from the University of Warwick has revealed.
The results, published in the Journal of Headache and Pain, suggest an association between the two types of pain that could point to a shared treatment for both.
The researchers from Warwick Medical School who are funded by the National Institute for Health Research (NIHR) led a systematic review of fourteen studies with a total of 460,195 participants that attempt to quantify the association between persistent headaches and persistent low back pain.
They found an association between having persistent low back pain and having persistent (chronic) headaches, with patients experiencing one typically being twice as likely to experience the other compared to people without either headaches or back pain. The association is also stronger for people affected by migraine.
The researchers focused on people with chronic headache disorders, those who will have had headaches on most days for at least three months, and people with persistent low back pain that experience that pain day after day.
These are two very common disorders that are leading causes of disability worldwide.
Around one in five people have persistent low back pain and one in 30 have chronic headaches.
The researchers estimate that just over one in 100 people (or well over half a million people) in the UK have both.
Professor Martin Underwood, from Warwick Medical School, said: “In most of the studies we found that the odds were about double — either way, you’re about twice as likely to have headaches or chronic low back pain in the presence of the other.
Which is very interesting because typically these have been looked as separate disorders and then managed by different people.
But this makes you think that there might be, at least for some people, some commonality in what is causing the problem.
Around one in five people have persistent low back pain and one in 30 have chronic headaches.
The researchers estimate that just over one in 100 people (or well over half a million people) in the UK have both.
“There may be something in the relationship between how people react to the pain, making some people more sensitive to both the physical causes of the headache, particularly migraine, and the physical causes in the back, and how the body reacts to that and how you become disabled by it.
There may also be more fundamental ways in how the brain interprets pain signals, so the same amount of input into the brain may be felt differently by different people.”
“It suggests the possibility of an underpinning biological relationship, at least in some people with headache and back pain, that could also be a target for treatment.”
Currently, there are specific drug treatments for patients with persistent migraine.
For back pain, treatment focuses on exercise and manual therapy, but can also include cognitive behavioural approaches and psychological support approaches for people who are very disabled with back pain.
The researchers suggest that those types of behavioural support systems may also help people living with chronic headaches.
Professor Underwood added: “A joint approach would be appropriate because there are specific treatments for headaches and people with migraine.
Many of the ways we approach chronic musculoskeletal pain, particularly back pain, are with supportive management by helping people to live better with their pain.
“We could look at developing support and advice programmes that are appropriate for this population.
And being aware of this relationship has the potential to change how we think about managing these people in the NHS on an everyday basis.
There is a need for doctors and other healthcare professionals to think that when treating one issue to ask about the other and tailor the treatment accordingly.
For future research, there’s probably work that needs to be done to understand what the underlying mechanisms behind this relationship are.”
Low back pain and headache are leading causes of disability worldwide [1, 2]. Each headache disorder has specific diagnostic criteria [3].
The commonest types of headache are migraine, tension-type (both primary headaches) and medication overuse headache (a secondary headache) [4].
Migraine and tension-type headache featured in two of the eight causes of chronic disease and injury, each affecting more than 10% of the world’s population [1].
Chronic headache is a severely disabling condition affecting around 3–4% of adults worldwide [5].
It is defined as a headache occurring on ≥15 days per month for more than 3 months [3].
Low back pain has a high healthcare burden, and in the most recent global burden of disease study, both low back pain and migraine were featured in the five leading causes of years lived with disability [1].
Around 4% of the UK population take time off work because of low back pain, resulting in around 90 million working days lost and between 8 and 12 million General Practitioner (GP) consultations per year [6].
Chronic low back pain is defined as pain felt in the area between the bottom of the rib cage and the buttock creases for more than 3 months [7].
There is a considerable focus in headache management in achieving a precise diagnosis in line with the International Classification of Headache Disorders [3].
Once a diagnosis is identified, management is focused accordingly [3, 8]. In contrast once serious causes of low back pain are excluded (malignancy, vertebral fractures, inflammatory disorders or infection) non-specific low back pain is diagnosed.2, 3,
People with persistent low back pain and people with chronic headache disorders are typically managed by clinicians from specific clinical specialities rather than experts in the management of chronic pain syndromes [9].
Whilst this approach may be appropriate for those living with one of these chronic conditions, it may be different if people have both.
A previous systematic review of twin studies has identified a possible independent association between headache and low back pain [10]. People with both headache disorders and low back pain might constitute a neglected group that could have both conditions managed in combination rather than as separate entities.
Here, we describe a systematic review of observational studies reporting the association between headaches (primary headaches, and chronic headaches) and persistent low back pain.
Searches
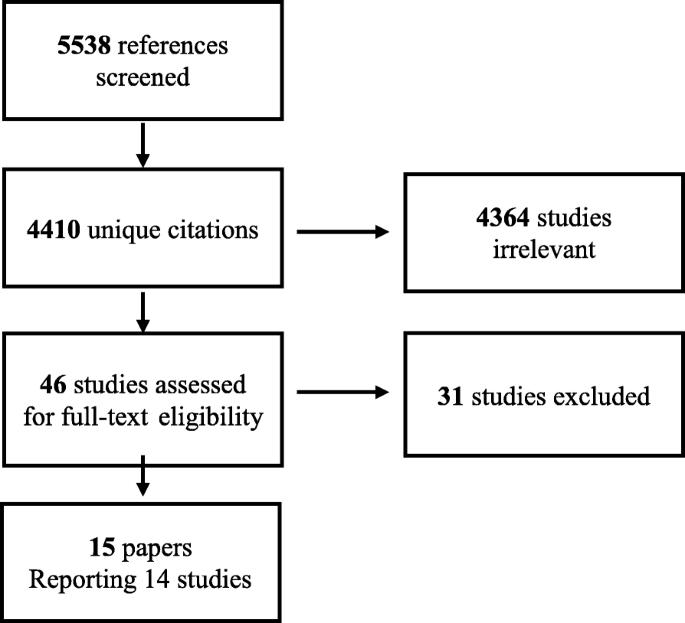
We identified 5538 potentially relevant citations, which included 4410 unique citations, 4364 of which did not meet inclusion criteria. Overall, we identified 46 studies that warranted scrutiny of the full text, 15 of these were included in the review. Thirty-one studies were excluded because they did not include a headache and back pain free group, or did not report on any association between low back pain and headaches. We included 15 papers reporting on 14 studies (Fig. 1). Citation tracking did not yield any additional result.
Definitions of headache and back pain
Definitions of low back pain varied. Due to the nature of observational studies low back pain was self-reported but the detail asked of participants, and described by studies was variable (Table 1). Swain et al. [20], used a five point scale to report low back pain frequently in the past 6 months. Hartvigsen et al. [15, 16], asked several specific questions regarding low back pain (‘have you during the past month suffered from back pain, acute low back pain or lumbago?’)
Few studies measured self-reported back pain with established questionnaires. Hestbaek et al. 2006 [26], measured low back pain with a Nordic questionnaire as did Sjolie et al. [19],. Bener et al. [24], used a variety of outcome measures including the Roland-Morris Disability Questionnaire [29], a widely used health status measure for low back pain. Jones et al. [17], provided an illustration of a shaded area of the lower back participants where participants may have expected to experience low back pain in the past month. Angst et al. [21], distinguished between lumbar back pain versus cervical pain [21].
Persistency of low back pain was described infrequently. Chronic low back pain was defined by pain in the low part of the back and thigh pain radiating to above the knee lasting over 3 months by Bejia et al. [23]
Hestbaek et al. 2006 [26], defined persistent low back pain being longer than 30 days in the past year, Yoon et al. asked for self-reported low back pain more than 15 days per month [10]. Ashina measured low back pain by self-reported frequency in the last year [22].
Like low back pain, there were varying definitions of headache, and chronic headache. Only the two studies by Ashina et al. [22], and Yoon et al. [10] used the ICHD (2nd edition) [30], now superseded by a third edition [3]. Yoon et al. also used a validated headache-screening questionnaire [10, 31].
Six studies specified that migraine or headache was self-reported [15, 16, 18,19,20, 23, 25]. Bener et al. [24], and Jones et al. [17], provided no definition, and Angst et al. [21] reported on participants reporting migraine or headache.
Hestbaek et al. [26], analysed participants according to any positive answers to headache regardless of aetiology (migraine, headache with nausea, headache with photophobia/phonophobia, severe ocular pain).
Schur et al. [28] asked if participants had a doctor’s diagnosis of headache, the authors here also explained why they used a self-reported method rather than diagnostic criteria, as validated measures were too lengthy and diagnostic criteria were not agreed upon. Hartvigsen et al. [15, 16] asked participants in a survey whether a physician had ever told them they suffered from various diseases (outcome reported as migraine headache in results), answers were taken as valid if participants confirmed that a diagnosis was made by a physician. Therefore, whether participants are truly reporting migraine or another type of headache is unclear [15, 16].
Three studies involved face-to-face interviews within the sample. Ahangar et al. [25] used a mixture of questionnaires and in-person interviews to collect data from elderly people in the town of Amirkola, Iran. Bener et al. [24] used trained nurses to interview patients and complete questionnaires. Angst et al. [21] used a stratified subsamples of the original sample for face-to-face interviews, two-thirds of those participants scoring high risk for psychopathological syndromes according to the Symptom Checklist-90-R [32].
No studies reported on the severity of headache and severity of low back pain.
Relationship between specific headache types and persistent low back pain
Table 3 summarises the results of the included studies. Ashina et al. [22] found 649/796 (81.5% of their participants had lifetime prevalence of low back pain); 321/796 (40.3%) of their participants had primary headache (migraine and/or frequent episodic tension type headache or chronic tension type headache). Of these 475/796 (59.7%) reported infrequent episodic tension type headache or no headache categorised as no headache in the past year; 281/796 (35.3%) had episodic headache, 80/796 (10.1%) had pure migraine, 138/796 (17.3% had pure tension type headache, and 103/796 (12.9%) had coexistent migraine and tension-type headache.
No case of chronic migraine was identified in the study. Ashina et al. [22] noted a positive correlation between the number of days with tension type headache or migraine and number of days with low back pain in the past year (r = 0.25, p < 0.001, r = 0.16, p < 0.001, respectively). The lifetime relative frequency of low back pain was higher in those with primary headache migraine and or tension type headache than those without headache (87.2 versus 77.7%) (p = 0.001). The adjusted odds ratio for primary headache (migraine and or frequent tension type headache or chronic tension type headache) and low back pain was OR 1.7 (95% CI 1.2–2.5).
Yoon et al. [10], identified those affected by chronic low back pain and primary headache disorders. The outcome variable of low back pain was defined as presence of frequent low back pain (yes vs. no), defined as self-reported low back pain occurring on more than or equal to 15 days per month. We present their multivariate analysis results (adjusted for age, gender, smoking status, drinking status, education level, BMI).
The association between migraine and low back pain was OR 1.2 (95% CI 0.7–2.1) (Ashina et al.) [22], and frequent low back pain and episodic migraine (no coexisting tension-type headache) OR 4.6 (95% CI 4.0–5.4)(Yoon et al) [10].
The association between episodic headache and low back pain was OR 1.7 (95% CI 1.2–2.5) (Ashina et al.) [22] and frequent low back pain and episodic headache OR 3.8 (95% CI 3.4–4.2) (Yoon et al) [10]. Associations between tension-type headache and low back pain were as follows; pure tension-type headache and low back pain OR 1.9 (95% CI 1.2–3.1) (Ashina et al.) [22] and episodic tension-type headache OR 3.5 (95% CI 3.0–4.1) (Yoon et al) [10].
Combining migraine and tension type headache disorders and experience of low back pain
Ashina et al. [22] found an OR 2.4 (95% CI 1.3–4.4), and Yoon et al. [10] found an OR 4.8 (95% 4.2–5.5) between frequent low back pain and episodic migraine with coexisting tension-type headache.
Chronic headache and low back pain
Ashina et al. [22] found 40 individuals that reported chronic headache. In their analysis of chronic headache and low back pain the adjusted odds ratio was 1.9 (95% CI 0.8–4.5). Low back pain was used in analysis if it had been reported occurring at least 1 day in the past year.
Yoon et al. [10], found an odds ratio of chronic low back pain and chronic headache of 8 (95% CI 5.3–12.1); low back pain and chronic migraine with coexisting tension type headache OR 9.3 (95% CI 5.6–15.5); low back pain with chronic migraine (no coexisting tension type headache) OR 9.5 (95% CI 4.9–18.4); low back pain and chronic tension type headache OR 4.4 (95% CI 2.1–9.0).
Source:
University of Warwick
Media Contacts:
Peter Thorley – University of Warwick
Image Source:
The image is in the public domain.
Original Research: Open access
“The association between headache and low back pain: a systematic review”. Arani Vivekanantham, Claire Edwin, Tamar Pincus, Manjit Matharu, Helen Parsons, Martin Underwood.
Journal of Headache and Pain doi:10.1186/s10194-019-1031-y.



{kind=link}