











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A team of researchers at Massachusetts General Hospital and Harvard Medical School has found that it is possible to remove carbon monoxide (CO) from blood by shining a red light on it as it moves through an artificial lung. In their paper published in the journal Science Translational Medicine, they describe their device and how well it worked during testing on rats.
Carbon monoxide poisoning is one of the most common types of accidental poisonings. The gas is produced during fires and explosions.
When inhaled, it can damage organs and quite often kill the victim.
The odorless gas is so dangerous because it displaces oxygen from hemoglobin, resulting in oxygen starvation throughout the body.
The current treatment for CO poisoning is administration of 100 percent oxygen, sometimes in a hyperbaric chamber.
Such treatments, unfortunately, are not fast enough to prevent damage. Because of that, scientists have been looking for ways to remove CO from the blood faster. In this new effort, the researchers used red light.
Scientists discovered over 100 years ago that shining a red light on blood can break the bonds between CO and hemoglobin, allowing oxygen to take its place. But a means of using light to help carbon monoxide patients has not been thoroughly examined until now.
Warren Zapol discussing extracorporeal phototherapy to treat carbon monoxide poisoning. Credit: Warren Zapol, Massachusetts General Hospital
In their work, the researchers found that cutting open a rat and shining a red light on its lungs did help removed CO, but the technique would not work in humans because our lungs are less transparent.
That led them to the idea of combining a red light with an artificial lung.
Video describing the development of a membrane oxygenator for the extracorporeal removal of carbon monoxide using phototherapy. Credit: Warren Zapol, Massachusetts General Hospital
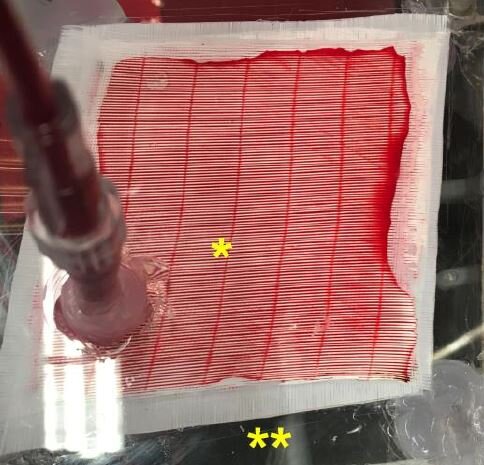
An artificial lung has a port for accepting a steady flow of blood—membranes are used to remove carbon dioxide and then to replace it with oxygen, just as real lungs do. The rejuvenated blood is then pumped back into the patient. The researchers modified the artificial lung by adding a section in which red light shined on it. This released CO in the blood, making room for the oxygen.
The researchers found that the device removed 79 percent of CO in poisoned rats compared to rats undergoing the same procedure with artificial lungs without red lights. They further report that when the rats had lung damage, the device tripled the speed of CO elimination over control groups. More testing is required to determine if humans will respond in the same manner.
More information: Luca Zazzeron et al. Phototherapy and extracorporeal membrane oxygenation facilitate removal of carbon monoxide in rats, Science Translational Medicine (2019). DOI: 10.1126/scitranslmed.aau4217
Journal information: Science Translational Medicine
Carbon monoxide (CO) gas exposure is the most common human poisoning. Upward of 50,000 patients a year are poisoned with CO in the United States (1).
The initial clinical presentation varies in patients suffering from CO poisoning: it can take the form of a headache, altered mentation, or coma, and carries a 1–3% mortality rate (2). Up to a third of moderate to severely CO poisoned patients will show signs of cardiac dysfunction, which is associated with long-term mortality (3).
Even with current therapy, 15–40% of patients will experience long-term neurocognitive sequelae (4, 5).
These neurologic and cardiac deficits do not necessarily correlate with blood CO levels, but more likely result from the pleiotropic effects of CO poisoning on oxygen delivery and cellular function.
CO competes with oxygen by binding directly to hemoglobin, thus reducing oxygen carrying capacity.
CO also exerts an R-state stabilizing effect that cooperatively increases ligand affinity, reducing hemoglobin P50 and oxygen delivery (Figures 1A and 1B) (2).
Finally, CO directly inhibits mitochondrial respiration via binding to a heme a3 of cytochrome c oxidase (Figures 1C and 1D) (6).

The effects of CO on Hb and mitochondria. CO competitively binds to Hb with oxygen, reducing carrying capacity (A). CO binding to Hb, similar to oxygen, stabilizes the relaxed, R-state of Hb, increasing other sites’ affinity for oxygen binding, reducing oxygen delivery by the remaining, non-CO-bound Hb (shifting the oxygen dissociation curve to the left) (B) (solid line, normal; dashed line, CO poisoning) (2). Normally, cytochrome c (C) feeds an electron (e−) into the heme a subunit I of cytochrome c oxidase (CytA, binuclear center with Fe2+ and copper [CuA]), which pumps a proton (H+) across the mitochondrial inner membrane (to be used by ATP synthase [not pictured]). The electron participates in the reduction of O2 to H2O at the heme a3 subunit II of cytochrome c oxidase (CytB, binuclear center with Fe2+ and copper [CuB]) (C). In CO poisoning, CO competitively binds with heme a3, shutting down the reduction of oxygen and stopping the transport of protons. The electrons fed in through cytochrome c from complexes I–III are unable to complete oxidative phosphorylation and can form free radicals (D) (2, 6).
There is no current antidote for CO poisoning, and management options are limited to normobaric oxygen or hyperbaric oxygen therapy.
One hundred percent normobaric oxygen therapy reduces the elimination half-life of CO from 320 to 74 minutes, and further to 20 minutes under hyperbaric conditions (3–5 atmospheres of pressure), by increasing the partial pressure of oxygen, which competes with CO for Hb binding (2, 7–9).
The practical efficacy of hyperbaric oxygen therapy is quite limited because of the significant time delays between diagnosis in the field, transportation to a hyperbaric facility, and actual treatment (2, 10).
There is conflicting evidence that hyperbaric oxygen therapy is efficacious: a meta-analysis of seven randomized control trials in 2011 (11) showed no significant benefit.
Even in positive studies, neurological impairment, although improved, remains substantive (2, 11) There is clearly an unmet clinical need for better therapies for CO poisoning.
In this issue of the Journal, Zazzeron and colleagues (pp. 1191–1199) have developed a creative treatment technology based on photolysis of CO bound to hemoglobin, enhancing the dissociation rates of CO and clearance in exhaled breath (12).
The investigators used lung phototherapy at 630 nm in a murine model of CO poisoning, using photo-dissociation of carboxyhemoglobin (COHb) in the pulmonary circulation (13). They reported a reduction in the half-life of COHb by measuring both the exhaled CO concentration and the rate of decline of COHb levels.
The half-life of COHb was more than halved with direct pulmonary phototherapy on the lungs in a mouse open-thoracotomy exposure model.
Phototherapy, when given during ongoing poisoning, reduced apparent uptake rates and improved survival.
To demonstrate a less invasive, and perhaps more clinically practical, means of providing this therapy, the group used an esophageal optical fiber placed in mice with CT scan guidance to optimize proximity to the lungs.
This also reduced the half-life of COHb, although to a lesser extent than the direct invasive lung phototherapy approach.
Although this technology is quite innovative and opens the door to new thinking on how to enhance CO clearance rates without hyperbaric oxygen, the thoracotomy approach to phototherapy is associated with as many or more limitations as hyperbaric oxygen.
The use of a less invasive trans-esophageal illumination is clearly feasible, as esophageal suction catheters and balloon devices are frequently placed in medical practice and in emergent situations. However, this approach will be challenged by the limited tissue penetration of the 630 nm wavelength of light, which is the absorbance of ferric hemoglobin within the visible range (14).
Unfortunately, illumination at the near-infrared or infrared range for deeper tissue penetration has minimal effects on CO dissociation rates from hemoglobin (13, 15). Although the 630 nm light worked in a mouse with a thin esophagus, it would not be expected to work in a human with much thicker esophageal and mediastinal tissue separating the light source from the pulmonary circulation.
Even in the mouse, the effect size of the esophageal phototherapy was less than that observed with direct phototherapy of the exposed lung. For example, the control 100% oxygen half-life of COHb in mice was 6.8 minutes, and the esophageal illuminary therapy only lowered the COHb half-life to 5.7 minutes.
There is a large body of evidence that the toxicity of CO poisoning, and specifically neurocognitive deficits, is not from COHb levels per se, but is, rather, a result of the effects of mitochondrial poisoning, free-radical generation, and activation of the immune response (2,6). A now classic canine study illustrated the importance of cellular toxicity and the effect of CO diffusion into tissues (16). In this study, the toxicity of inhaled CO was greater than the toxicity of the same concentration of COHb, given as an infusion of ex vivo CO-treated red blood cells. It is unclear whether phototherapy could be expected to be better than hyperbaric therapy at reversing such effects, which require release of CO from cytochrome c oxidase into the circulation to bind with hemoglobin or to diffuse directly into exhaled breath. In fact, this might require direct tissue phototherapy for enhanced dissociation from cytochrome c oxidase.
Although these challenges suggest limitations to the current therapy, the technology developed in this study highlights the promise of reducing COHb half-lives in the blood, using photodissociation methods.
This concept opens the door to alternative, more efficient methods for the delivery of phototherapy. Similar to hemodialysis, extracorporeal photodynamic blood illumination has been proposed to externally remove blood, exposing blood to an illuminator and reperfusing blood back to the patient (17).
Perhaps this technology could be adapted to dialysis circuits, which are more readily available than hyperbaric oxygen therapy, which is offered at only several hundred centers in the United States (18). Total body cutaneous illumination for CO photodissociation has also been proposed, provided the photolyzed CO does not rebind completely before flow to the pulmonary arterioles and capillaries for diffusion to exhaled breath (19). Another option may be development of light-emitting nano or microparticles, such as quantum dots, which would deliver the light directly to red blood cells and tissues (20).
There are clearly several creative ways this technology could be modified to a more translatable therapy, now that these first quite important and innovative proof-of-concept studies have shined a light on a new path to cure.



{kind=link}