










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Researchers may have found a way to press pause on spinal disc injuries, giving doctors more time to treat them before worse issues develop.
The Penn Medicine-led team discovered that cells in the outer region of spinal discs become stressed and kick off a subpar healing process after injuries, which researchers then found can temporarily be blocked with drugs that calm the cells down.
This study, conducted using specially engineered biomaterials and small animal models, was published today in Nature Biomedical Engineering.
“This work sheds light on some of the challenges we are going to face in slowing disc degeneration and preventing back pain,” said Edward Bonnevie, Ph.D., a post-doctoral fellow in Penn Medicine’s McKay Orthopaedic Research Laboratory.
“Most spine research focuses on the inner part of the disc, but our work highlights the fact that we need to treat the whole disc, and we believe doing so may lead to the identification of new targets for therapy.”
Discs in the spine are pressurized and structured similarly to water balloons, with water-attracting proteins in the inner portion restrained by an outer layer of fibrous tissue containing cells that are under a constant stretch.
The discs are designed to cushion the vertebrae from directly and painfully contacting each other.
Bonnevie, senior author Robert L. Mauck, Ph.D., a professor of Orthopaedic Surgery and director of the McKay Lab, and their fellow researchers decided to focus their research on the often overlooked outer region of the discs.
“We know that cells in the inner region undergo changes as a result of disc injury and degeneration, and researchers have tried to restore function to those cells,” Bonnevie said.
“But you can think of that like trying to fill up a water balloon that already has holes – it isn’t a viable treatment option by itself.”
In biomaterials the researchers created to mimic tissue of the outer region of discs, they saw that when an injury like a slipped disc occurs and pressure is lost, the suddenly released tissue becomes disorganized.
When this happens, they found in small animal models that it results in the generation of repair tissue that did not resemble the normal tissue, but instead had characteristics of scar tissue.
Additionally, they found that programmed cell death – known as apoptosis – occurs quickly, within 24 hours of the injury.
This poses a challenge because, unlike other areas in the body, cells in the discs lack a blood supply and cannot easily repopulate with the new cells needed for regeneration.
With the discoveries of why disc cells respond the way they do upon pressure loss, the team found that using a biological inhibitor of cell contraction, such as fasudil, could effectively “relax” the cells from the shock of suddenly losing their typical stretched state.
Once relaxed, the cells would delay their default healing response, which has the potential to buy doctors what is called a “therapeutic window” to intervene.
“These data show us that treating disc injuries very soon after injury is essential, before this transition in phenotype occurs and the scar tissue forms.
This could be done using inhibitors like fasudil applied systemically, or potentially in combination with surgical implantation of biomaterials that are designed to restore the native tissue structure and function,” Mauck explained.
More information: Aberrant mechanosensing in injured intervertebral discs as a result of boundary-constraint disruption and residual-strain loss, Nature Biomedical Engineering (2019). DOI: 10.1038/s41551-019-0458-4 , https://nature.com/articles/s41551-019-0458-4
Journal information: Nature Biomedical Engineering
Provided by Perelman School of Medicine at the University of Pennsylvania
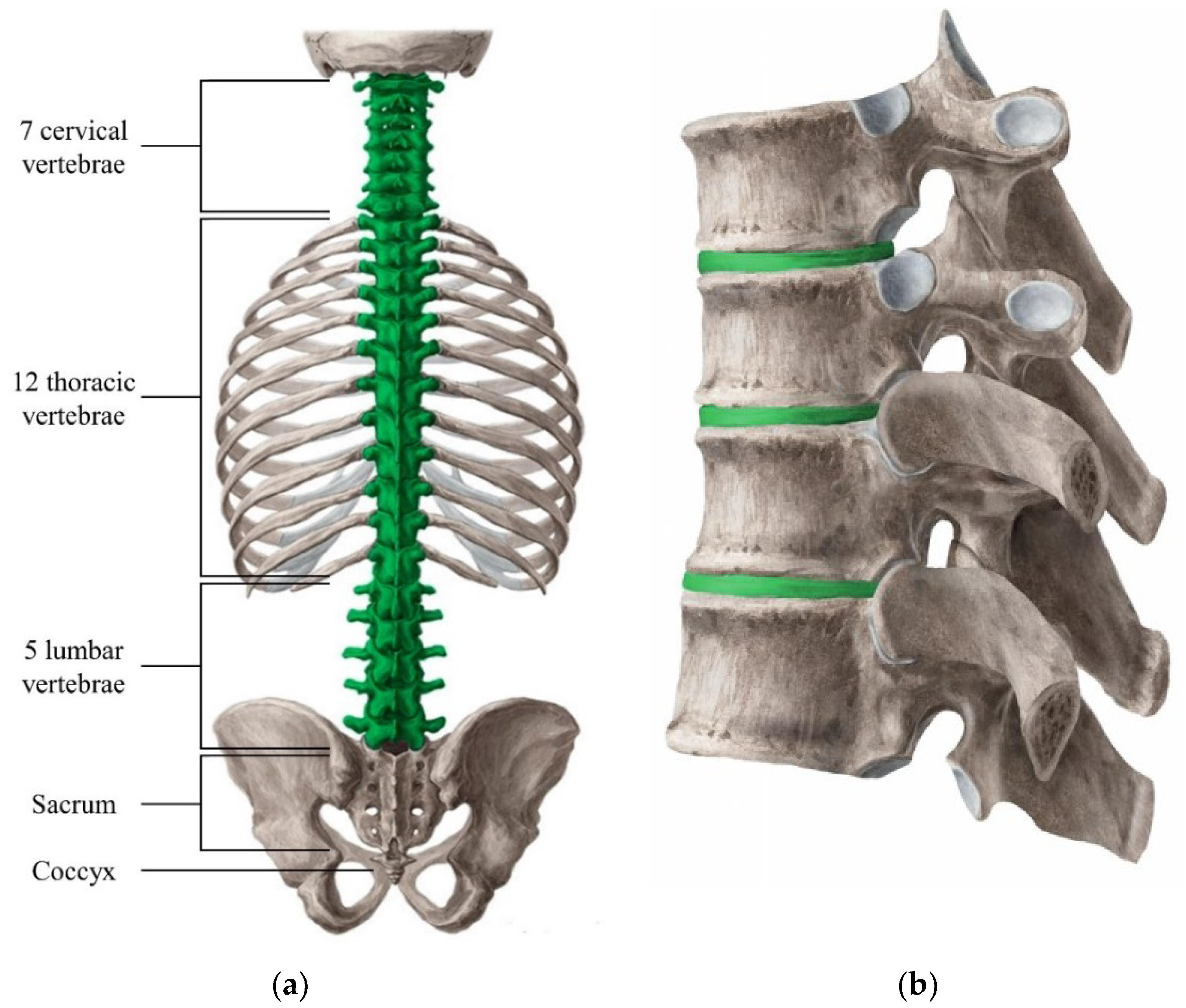
The spinal cord is a nervous tissue bundle from the medulla oblongata in the brainstem to the lumbar region, and the vertebral column protects it.
The vertebral column consists of seven cervical, 12 thoracic, five lumbar, five sacral, and three to five coccygeal vertebrae. The cervical vertebrae are numbered C1 to C7 from the base of the skull to the thoracic vertebrae.
The structure of C1, C2, and C7 have distinctive properties compared to C3 to C6. The anatomy of C3 to C6 consists of a central body, the pedicles anteriorly, lamina posteriorly completing a ring around the spinal cord.
Motion is mainly posteriorly at the superior and inferior articular processes with the vertebral artery, vein, and sympathetic plexus running through anterior foramen transversarium of the transverse process.
C1 (atlas) connects the skull and spine mainly by ligamentous attachments. It has no body due to fusion with axis (C2) vertebrae which acts as a pivot for the atlas to rotate. The most distinctive feature of C2 vertebrae is the strong odontoid process (dens) that rises perpendicularly from the upper surface of the body.
The body is deeper in front than behind, and prolonged downward anteriorly, so there is an overlap of the upper and front part of the third vertebra. C7 has a distinctive long and prominent spinous process, which is palpable from the skin surface. The transverse processes are larger in size.
The upper surface of each has a shallow sulcus for the eighth cervical nerve.
A cervical disc separates each cervical vertebrae. The composition is of inner nucleus pulposus of mucoprotein gel and outer annulus fibrosus. This composition allows for flexibility and mobility of the cervical spine. There is increased the risk of injury in cervical spine compared to the more fixed thoracic spine.
Etiology
Degenerative disc disease or acute disc herniation most commonly cervical disc injury. Degeneration of the disc occurs from a loss of water content leads to a decreased range of motion with susceptibility to facet joint disease. [1][2][3] Traumatic injuries caused by contact sports and automobile accidents which increase the risk of disc herniation.
Epidemiology
Neck pain affects up to 15% of the population in the United States with cervical disc disease. In other words, 84 out of 100,000 people have neck pain. Cervical disc injuries due to disc herniation affect people in their thirties to forties due to disc herniation, and degenerative disc disease affects people older than 50 years of age.[4]
History and Physical
The chief complaint of patients with cervical disc injury is neck pain with or without radiation to arm and fingers. Practitioners should obtain a thorough pain history that includes the severity, onset, duration, and characteristic of the pain. Other important information includes relieving, aggravating, and associated factors. Other symptomology includes muscle spasm, a decrease in mobility, and associated numbness or radicular pain.
A detailed physical examination of sensory and motor neurological examination should be performed. The doctor should assess the range of motion (ROM). The severity of pain, spasms, or degeneration affects flexion, extension, right and left rotation, and lateral flexion.
Evaluation
X-ray
Plain radiography is an initial and inexpensive method of evaluating the cervical spine for an osseous injury. In chronic disc degeneration, decreased disc height and osteophytes can be seen. There is a higher incidence of cervical cord injury demonstrated with the use of plain radiographs in the assessment of cervical spine stenosis. The Torg ratio is the sagittal canal/vertebral body ratio measured on cervical spine lateral radiographs. The normal value is 1.0. A ratio of 0.8 and below has been considered indicative of cervical spinal stenosis.
MRI
Magnetic resonance imaging is the best modality to assess cord compression and disc herniation. T2 weighted views are preferred. Findings include decreased disc height, reduced signal intensity, and spondylotic osteophytes.
Other Studies
Patients with equivocal studies may opt for a discography when conservative measures fail. Electrophysiological studies can be performed to evaluate and elucidate the nerve roots affected by injured cervical disc.[5][6]
Treatment / Management
In the acute phase, management consists of pain relief, physical therapy, and surgery. [6][7][8]
Non-Surgical
Pain relief is used to decrease the level of inflammation, allowing for physical therapy which includes segmental mobilization. Goals of therapy are to decrease pain, improve range of motion, strengthen muscles, and improve spinal biomechanics. Initial modes of pain relief are oral anti-inflammatory agents, as well as epidural injections. Depending on the severity of pain and the extent of pathology, medial bundle branch blocks or rhizotomies may be performed.
Surgical
When conservative management fails, surgery is indicated for acute disc herniation which causes central cord syndrome. Several techniques have been described based on pathology. Anterior discectomy with fusion is the recommended procedure for anterolateral or central soft disc herniation, while a posterior laminoplasty or laminectomy may be considered when technical limitations for anterior access exist or when the patient has had prior surgery at the same level.
Surgical intervention is indicated for patients who have had six weeks to three months of conservative management of disc herniation or degenerative disc disease. Associated worsening myelopathy or neuropraxia are also indications for surgery.
Several surgical procedures can be performed. These procedures are total disc replacement, anterior cervical discectomy and fusion (ACDF), laminectomy, or laminoplasty. Indications for total disc replacement surgery include symptomatic, spontaneous/degenerative, or traumatic herniated cervical nucleus pulposus with or without radiculopathy, and cervical degenerative disc disease without posterior column instability. Indications for anterior cervical discectomy and fusion surgery included cervical spondylosis, stenosis herniated discs, degenerative disc disease with instability and facet arthritis, tropism, or facetogenic pain.
Brief Surgical Techniques
Total Disc Replacement (TDR) and Anterior Cervical Discectomy and Fusion (ACDF)
Surgical exposure of the desired vertebral level is achieved through an anterior cervical incision. Subcutaneous dissection is performed to allow for adequate mobilization to tissue incision. The discectomy is performed with pituitary rongeurs, curette, and a burr drill to remove affected disc. The posterior longitudinal ligament can be left in situ depending on the severity of herniation. The center of the disc is identified. A keel is made using the burr after which the disc is removed and disc replacement performed. A similar surgical method is used for anterior cervical discectomy and fusion, the difference is the type of implant, which can be an interbody cage with an anterior cervical plate or a standalone cage. Although complications are rare, patients experience dysphagia, hoarseness, and transient sore throat. Adjacent segment disease or pseudoarthrosis can occur depending on severity and number of levels operated. The majority of patients get symptomatic relief and can resume full activity after six months.
Laminectomy
Cervical laminectomy removes the lamina on one or both sides to increase the axial space available for the spinal cord. Clinically indicated for spinal stenosis or cervical disc disease involving more than three levels of disc degeneration with anterior spinal cord compression. Single-level cervical disc herniation is usually managed with the anterior approach. The complications of the posterior approach include instability resulting in kyphosis, recalcitrant myofascial pain, and occipital headaches.
Laminoplasty
The kyphotic deformity is a well-known complication of laminectomy. To preserve the posterior wall of the spinal canal while decompressing the spinal canal a Z-plasty technique for the lamina was developed. The variant of the procedure uses a hinged door for the lamina. Laminoplasty is commonly indicated for multilevel spondylotic myelopathy. Nerve root injury is seen in about 11% of the surgeries. This complication is unique to laminoplasty, and the suggested etiology is traction on the nerve root with the posterior migration of the spinal cord.
Enhancing Healthcare Team Outcomes
The diagnosis of cervical disc disease is difficult because there are many causes of pain in the neck area. The disorder is best managed by a multidisciplinary team that includes a pain specialist, radiologist, nurse practitioner, primary physician, orthopedic surgeon, emergency department physician and a physical therapist. Once diagnosed the treatment is initially conservative. Only patients who do not respond to conservative treatment or those who continue to have neurological symptoms should be referred for surgery. Unfortunately, the results of surgery are not optimal with many patients continuing to have chronic pain which is disabling. No matter what treatment is selected, physical therapy is highly recommended. [9][10][11]



{kind=link}