










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



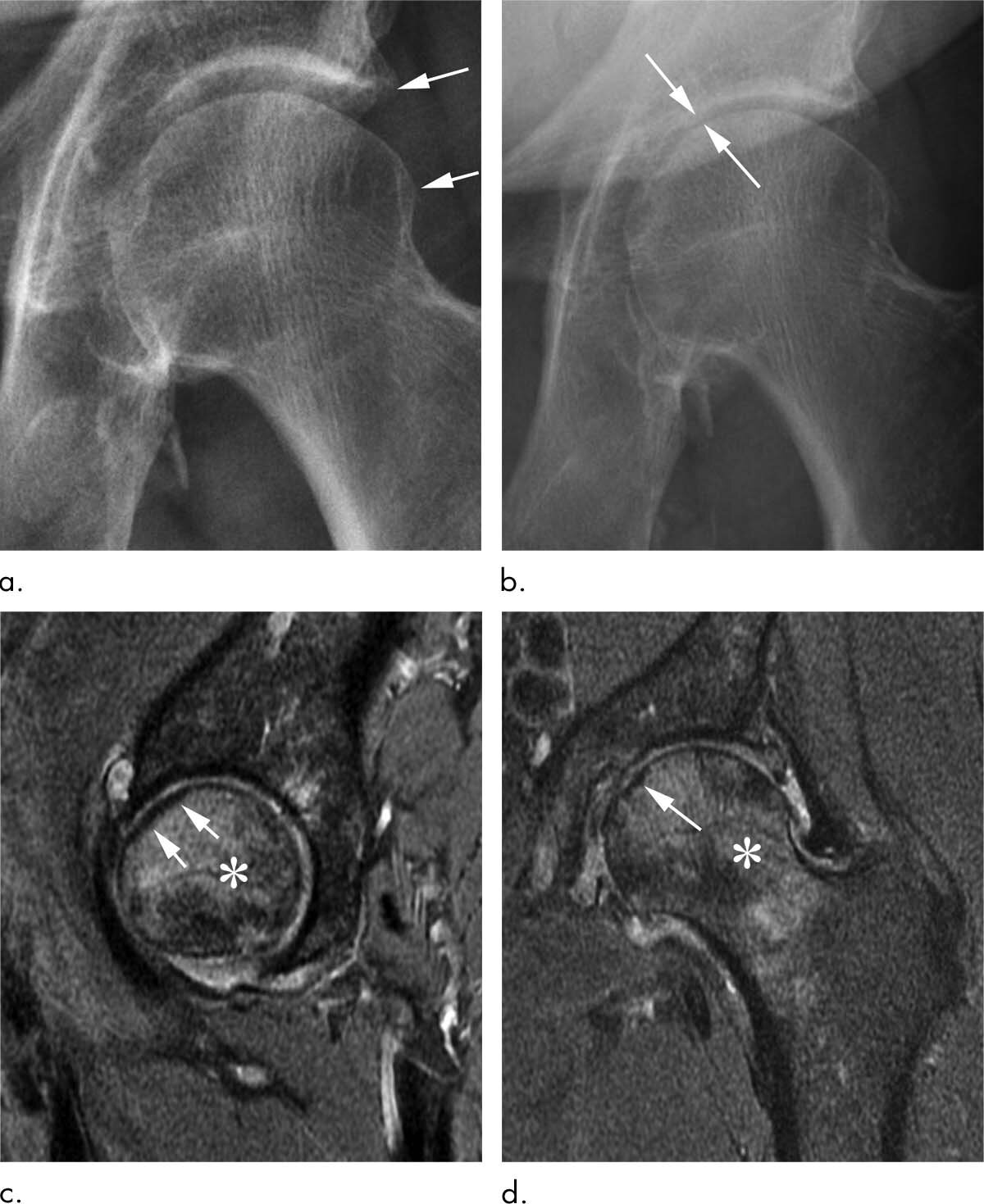
Corticosteroid injections used to treat osteoarthritis pain in the hip and knee may be more dangerous than previously thought, according to a special report published in the journal Radiology.
Researchers suggested that injection-associated risks like rapid progressive osteoarthritis, which eventually may lead to joint collapse, should be integrated into consent forms so that patients are aware of the potential risks associated with these treatments.
Osteoarthritis of the hip and knee are common and debilitating joint disorders.
Physicians often inject anti-inflammatory corticosteroids into the joint to treat the pain and swelling associated with osteoarthritis.
The procedure is widely viewed as safe, and patient consent forms mainly mention the risks of hemorrhage and infection among more rare side effects associated with most needle-based procedures.
However, a recent study led by Ali Guermazi, M.D., Ph.D., professor of radiology and medicine at Boston University School of Medicine, found that corticosteroid injections may be associated with complications that potentially accelerate the destruction of the joint and may hasten the need for total hip and knee replacements.
“We’ve been telling patients that even if these injections don’t relieve your pain, they’re not going to hurt you,” Dr. Guermazi said.
“But now we suspect that this is not necessarily the case.”
In a review of existing literature on complications after treatment with corticosteroid injections, Dr. Guermazi and colleagues identified four main adverse findings: accelerated osteoarthritis progression with loss of the joint space, subchondral insufficiency fractures (stress fractures that occur beneath the cartilage), complications from osteonecrosis (death of bone tissue), and rapid joint destruction including bone loss.

The researchers recommend careful scrutiny of patients with mild or no osteoarthritis on X-rays who are referred for injections to treat joint pain, especially when the pain is disproportionate to the imaging findings.
Prior research has shown that these patients are at risk of developing rapid progressive joint space loss or destructive osteoarthritis after injections.
Physicians may also want to reconsider a planned injection when the patient has acute change in pain not explained by X-rays as some underlying condition affecting joint health may be ongoing, the researchers said.
Most importantly, younger patients and patients earlier in the course of the disease need to be told of the potential consequences of a corticosteroid injection before they receive it.
“Physicians do not commonly tell patients about the possibility of joint collapse or subchondral insufficiency fractures that may lead to earlier total hip or knee replacement,” Dr. Guermazi said. “This information should be part of the consent when you inject patients with intra-articular corticosteroids.”

With corticosteroid injections so widely used, the potential implications of the study are enormous, according to Dr. Guermazi.
“Intra-articular joint injection of steroids is a very common treatment for osteoarthritis-related pain, but potential aggravation of pre-existing conditions or actual side effects in a subset of patients need to be explored further to better understand the risks associated with it,” Dr. Guermazi said. “What we wanted to do with our paper is to tell physicians and patients to be careful, because these injections are likely not as safe as we thought.”
Osteoarthritis (OA) is a highly prevalent and extremely disabling condition, affecting 30.8 million people in the USA alone [1]. In 1741, J.B. Morgagni first described articular cartilage loss in OA [2]. To this day, radiographic measurement of cartilage loss remains the key diagnostic tool for OA [3].
Consequentially, chondroprotection has been a major focus of disease modifying treatment in OA. Chondroprotective drugs (disease modifying OA drugs, DMOADs) have generally targeted structural changes of disease by aiming to inhibit cartilage-degrading factors or promote cartilage production, with or without effects on symptoms.
Of the $81 billion annual healthcare expenditure on OA in the USA, 15% is attributed to prescription drugs [4, 5]. However, an effective means to prevent OA-related damage has proven elusive.
Therefore, much of this expenditure centers on drugs that target pain rather than structural changes.
Given current limitations in DMOADs, OA progresses and surgical joint replacement is the only viable option.
However, joint replacement is by no means a panacea with a mortality rate of 1% and at least 10% of total hip or knee replacements reporting no improvement or worse symptoms at 1 year after surgery [6, 7].
In this review, we consider recent progress and challenges in chondroprotection and how chondroprotection should encompass both direct (within cartilage) and indirect (articular or systemic) strategies.
We also discuss how a step change in successful chondroprotection requires reframed thinking in disease stratification, target identification, and drug development, including drug delivery strategies.Go to:
Osteoarthritis – Chondroprotection Is Not Chondrocentric
Osteoarthritis (Fig. 1) occurs at synovial joints and was long regarded as a structural disease of wear and tear.
The key symptoms of OA are pain and joint instability, with radiographic joint space narrowing due to cartilage loss being a major clinical sign of disease. Alongside OA-related cartilage degradation, osteophytes form at joint margins, and bone remodeling occurs, leading to bone marrow lesions and bone sclerosis [8].
Synovitis (synovial inflammation) and meniscal damage are common and altered levels of inflammatory mediators are detected in OA synovial fluid. Furthermore, OA is now widely accepted as a whole joint disease [9], but the chronicity of tissue involvement in OA remains ambiguous, and cartilage may not be the initial site from which OA propagates.
The cross-talk between cartilage and other tissues suggests cartilage loss can occur secondary to other OA-related changes to the joint [10].
We must also remember that synovial joints are, in fact, comprised of diverse tissues that experience different loads; have distinct functional requirements; and possess differing proportions of tissue types.
The interactions of these factors likely explain the predilection of OA for certain anatomical sites (commonly knee, hip, spine, hands, and feet).

A representation of an osteoarthritic knee, including the main contributing tissues and their interactions. The exact balance of tissue involvement and interaction is dependent on both joint site and the subtype of OA. Articular cartilage loss typifies OA but the exact balance of tissue involvement and interaction is dependent on joint site, stage and subtype of disease
Chondroprotection offers a preventive strategy that might decelerate structural disease progression and loss of function and, through the manipulation of inflammatory pathways, improve pain. However, the success of such strategies demands a holistic approach that judiciously targets OA pathobiology across all joint tissues.
Disease Stratification – Breaking Down a Spectrum of Diseases into Different Subtypes
Advances in clinical, molecular, and genetic characterization of OA suggest it is better regarded as a spectrum, or continuum, of conditions leading to end-stage disease with a common entity: loss of articular cartilage [51]. This is unsurprising given the varied clinical manifestations of OA. However, most current clinical and laboratory-based studies do not consider disease subtypes in their study design.
Disease stratification is best demonstrated in oncology, where the ability to utilize molecular information to predict prognosis and optimal therapeutic strategy has been the first step towards personalized treatment [52]. To apply this to chondroprotection in OA, we must consider the key characteristics by which to stratify patients (Fig. 2).

Overview of OA stratification categories and their interactions. Clinical signs and symptoms, risk factors, and molecular signatures interact and can define OA subtypes. The combinatorial effects of different stratification measures will define distinct subtypes and stages of OA. For example, risk factors such as trauma will drive changes in molecular and cellular signatures and altered clinical signs and symptoms. As OA progresses stratification categories will continue to feedback on each other, therefore individual stratification measures (or combinations thereof) may be specific to a particular stage of disease
Clinical Phenotypes
A first step to classify OA can be through the affected joint(s). Clinically adopted imaging, pain, and function scores can also incorporate affected joint surface(s) and stage of disease. There are several studies where these scores reveal patterns in chondroprotective response. Individuals with severe cartilage loss have a reduced likelihood of improved pain following intra-articular steroid injection [53, 54]. Meanwhile, strontium ranelate inhibition of cartilage loss was more effective in patients with meniscal extrusion and bone marrow lesions than in those with meniscal extrusion alone [55]. Osteophytes and synovitis may also predict the rate of structural progression [8, 56], which varies between individuals, influencing both prognosis and chondroprotective strategy [57]. Potential predictors of structural progression include pain [58], inertia [57], bone marrow lesions [59], joint loading [60], baseline Kellgren–Lawrence (KL) grade, obesity, and alignment [61]. However, few studies have the power and quality to reliably deconvolute clinical predictors of cartilage loss or other clinical outcomes [62].
Risk Factors
Risk factors for OA, including age, sex, and trauma, may hint at the underlying mechanism and determine the broadly applicable stratification steps. Age is associated with inflammaging and senescence and predicts improvement in pain following corticosteroid injection for knee OA [54]. Mechanisms underlying pain differ in males and females, and, consequentially, the mechanisms underlying cartilage damage may also be modulated by sex. Younger males are less likely to require joint replacement [63], and morphological differences between sexes might contribute to OA development and severity [64, 65]. Although few studies have investigated the effects of OA risk factors on pharmacologic driven chondroprotection, there is evidence that OA progression is reduced in post-menopausal women undergoing hormone replacement therapy [66, 67]. Site- and hormone-based interactions are also seen in the presentation of hand OA at the time of menopause, in contrast to other forms of OA that present post-menopause [68, 69]. Comorbidities, including obesity, diabetes, and metabolic syndrome, are additional risk factors for OA with clinically related readouts such as high serum cholesterol, which is associated with generalized OA [70]. Lifestyle, diet, and alteration of the microbiome may also affect OA onset and progression [71].
Joint loading and trauma significantly impact OA development. Lower step rate is associated with a greater risk of increased cartilage damage in knee OA patients [72]. Following traumatic ACL injury, initial cartilage damage is more common in the lateral and medial compartments of the knee than in the medial alone [73]. Sport-related knee injuries lead to a significantly greater likelihood of joint replacement [74], yet younger patients have differing underlying biology and immune status, higher physical demands, and greater need to avoid surgical joint replacement. These factors greatly impact the requirements of therapeutic chondroprotection while identifying a relatively defined group on which to test DMOADs [75].
The breadth of OA risk factors and clinical phenotypes demonstrates the wealth of potential disease subtypes. Risk factors alone, although identifiable prior to clinical presentation for OA, are not adequate to reliably predict OA occurrence or prognosis. A key advantage of stratifying OA patients based on observable clinical factors (pain, function, and imaging scores) is data accessibility: there is often no invasive testing needed and readouts are readily available in the clinic. When considering timing of DMOAD intervention and identification of disease mechanisms, patients often do not present to clinic until they have “end-stage” disease where pain or function is severely affected. Indeed, the structural features of OA do not consistently correlate with each other or with symptoms. Patients can suffer severe pain, but show limited radiographic evidence of OA, or have late-stage radiographic OA, but limited pain. However, cross-talk between cartilage damage and pain can occur, with pain-targeting strategies (e.g., corticosteroids) leading directly or indirectly to cartilage loss [76–78].
Neither the clinical phenotype nor the combination of risk factors directly reveals mechanism of disease, preventing meaningful identification, development, and evaluation of chondroprotective strategies [79]. In fact, a number of molecular mechanisms (endotypes) may contribute to each risk factor-induced effect and clinical phenotype. While a first step in stratification for chondroprotection may utilize clinical scoring and risk factors, it is unlikely that these will be meaningful in isolation. Future studies should explore the interrelationships among structure, function, and pain and integrate molecular endotyping to generate robust stratification systems.
More information: “Intra-articular Corticosteroid Injections of the Hip and Knee: Perhaps Not as Safe as We Thought?” Radiology, 2019.
Journal information: Radiology
Provided by Radiological Society of North America



{kind=link}