











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Chemotherapy has helped make the most common childhood cancer one of the most curable, but researchers have evidence that the treatment may also prime some patients for relapse.
Results published in the journal Blood reported that treatment-induced mutations cause drug resistance in some patients whose acute lymphoblastic leukemia (ALL) returns.
“Our study reveals the evolution dynamics of pediatric ALL, which suggest for the first time that chemotherapy treatment, particularly thiopurines, can cause mutations that lead to drug resistance in patients,” said study co-corresponding author Jinghui Zhang, Ph.D., chair of the St. Jude Children’s Research Hospital Department of Computational Biology. Thiopurines are a class of drugs used in most phases of ALL treatment.
The study involved 103 young ALL patients who relapsed. Most relapsed nine or more months after diagnosis.
The analysis revealed that about 20% of these patients had treatment-related mutations at relapse, some associated with drug resistance.
“The mutational signatures are specific and therapy-related, as they are only present in the genomes of relapsed ALL patients but not in other pediatric or adult cancer genomes,” Zhang said.
The findings underscore the need for less toxic therapies and precision-medicine approaches, said co-corresponding author Ching-Hon Pui, M.D., chair of the St. Jude Department of Oncology. Candidates in development include immunotherapies such as CAR-T cells and bispecific antibodies.
“This study points to the potential need to individualize therapy when drug resistant mutations emerge in ALL”, said co-corresponding author Jun J. Yang, Ph.D., of the St. Jude Departments of Oncology and Pharmaceutical Sciences. The other co-corresponding author is Bin-Bing Zhou, Ph.D., of Shanghai Children’s Medical Center and National Children’s Medical Center and the Shanghai Jiao Tong University School of Medicine.
Relapse remains leading cause of death
ALL is the most common childhood cancer. With current treatment, more than 90% of pediatric patients become long-term survivors. The prognosis is dismal for patients whose leukemia returns. Relapse accounts for 70 to 80% of ALL patient deaths.
Cause uncertain
While previous studies had identified relapse-specific drug resistance mutations, the origin of those mutations was unclear.
Some researchers proposed that ALL relapse was driven by drug-resistant leukemic cells present at diagnosis.
Whole genome sequencing analysis
The children in this study were treated in China. They underwent whole genome sequencing of leukemic cells collected at the diagnosis and relapse as well as normal DNA. The analysis also included targeted deep sequencing of leukemic cells collected regularly during treatment of 16 patients.
Researchers identified relapse-specific acquired mutations in 12 genes involved in drug response, including FPGS, a novel, relapse-related gene.
The analysis also revealed two novel mutational patterns or signatures. Researchers showed thiopurines caused one of the new mutational signatures. Additional research showed the mutations lead to multi-drug resistance.
Drug resistance and relapse timeline
The timeline of relapse of patients in this study and the presence of relapse-specific mutations in the 12 genes involved in drug response provided insight into the cause.
Most patients, 55%, relapsed nine to 36 months after diagnosis but before treatment ended. This group had the most relapse-specific mutations in the 12 drug-resistance genes, particularly compared to patients who relapsed earlier.
Mathematical modeling, mutational analysis and other evidence indicated that earlier relapse was likely caused by drug-resistant tumor cells present at diagnosis.
Investigators proposed a two-step process to explain later relapse. The model suggested that relapse occurred when partially drug-resistant tumor cells that were present at diagnosis acquired treatment-related mutations. The now drug-resistant cells divide and eventually cause relapse.
“This suggests drug resistance is not a foregone conclusion,” Yang said. “It may be preventable through changes in the dosage or timing of treatment.” Based on the findings, Pui said screening relapsed patients for drug-resistance mutations may be indicated.
his PDQ cancer information summary has current information about the treatment of childhood acute lymphoblastic leukemia. It is meant to inform and help patients, families, and caregivers.
It does not give formal guidelines or recommendations for making decisions about health care.
Editorial Boards write the PDQ cancer information summaries and keep them up to date.
These Boards are made up of experts in cancer treatment and other specialties related to cancer.
The summaries are reviewed regularly and changes are made when there is new information.
The date on each summary (“Date Last Modified”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Pediatric Treatment Editorial Board.
Childhood acute lymphoblastic leukemia (ALL) is a type of cancer in which the bone marrow makes too many immature lymphocytes (a type of white blood cell).
Childhood acute lymphoblastic leukemia (also called ALL or acute lymphocytic leukemia) is a cancer of the blood and bone marrow. This type of cancer usually gets worse quickly if it is not treated.
ALL is the most common type of cancer in children.
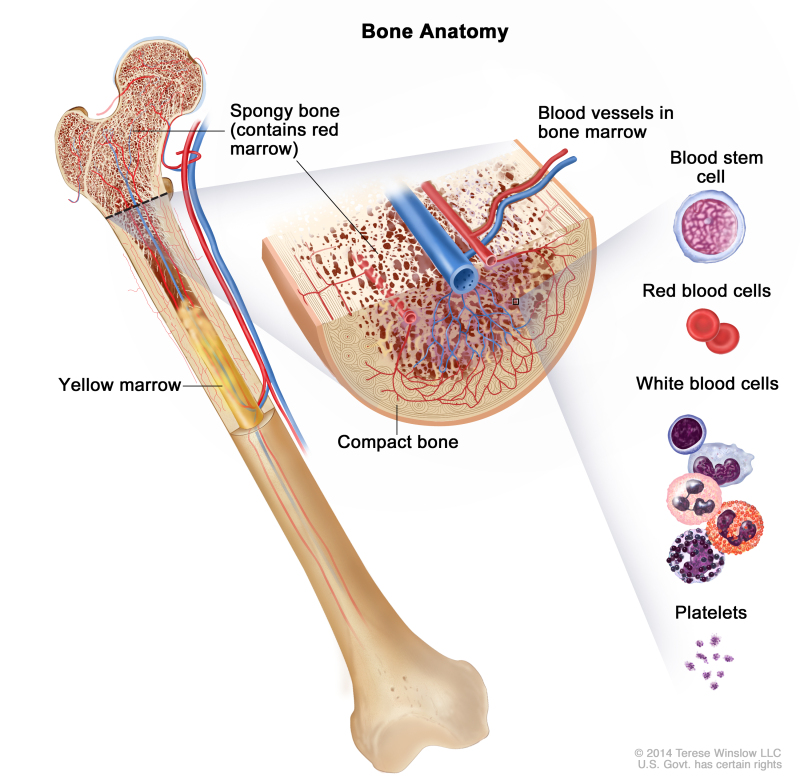
Leukemia may affect red blood cells, white blood cells, and platelets.
In a healthy child, the bone marrow makes blood stem cells (immature cells) that become mature blood cells over time. A blood stem cell may become a myeloid stem cell or a lymphoid stem cell.
A myeloid stem cell becomes one of three types of mature blood cells:
- Red blood cells that carry oxygen and other substances to all tissues of the body.
- Platelets that form blood clots to stop bleeding.
- White blood cells that fight infection and disease.
A lymphoid stem cell becomes a lymphoblast cell and then one of three types of lymphocytes (white blood cells):
- B lymphocytes that make antibodies to help fight infection.
- T lymphocytes that help B lymphocytes make the antibodies that help fight infection.
- Natural killer cells that attack cancer cells and viruses.

In a child with ALL, too many stem cells become lymphoblasts, B lymphocytes, or T lymphocytes. The cells do not work like normal lymphocytes and are not able to fight infection very well. These cells are cancer (leukemia) cells. Also, as the number of leukemia cells increases in the blood and bone marrow, there is less room for healthy white blood cells, red blood cells, and platelets. This may lead to infection, anemia, and easy bleeding.
This summary is about acute lymphoblastic leukemia in children, adolescents, and young adults. See the following PDQ summaries for information about other types of leukemia:
- Childhood Acute Myeloid Leukemia/Other Myeloid Malignancies Treatment
- Adult Acute Lymphoblastic Leukemia Treatment
- Chronic Lymphocytic Leukemia Treatment
- Adult Acute Myeloid Leukemia Treatment
- Chronic Myelogenous Leukemia Treatment
- Hairy Cell Leukemia Treatment
Past treatment for cancer and certain genetic conditions affect the risk of having childhood ALL.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your child’s doctor if you think your child may be at risk.
Possible risk factors for ALL include the following:
- Being exposed to x-rays before birth.
- Being exposed to radiation.
- Past treatment with chemotherapy.
- Having certain genetic conditions, such as:-Down syndrome.-Neurofibromatosis type 1.-Bloom syndrome.-Fanconi anemia.-Ataxia-telangiectasia.-Li-Fraumeni syndrome.-Constitutional mismatch repair deficiency (mutations in certain genes that stop DNA from repairing itself, which leads to the growth of cancers at an early age).
- Having certain changes in the chromosomes or genes.
Signs of childhood ALL include fever and bruising.
These and other signs and symptoms may be caused by childhood ALL or by other conditions. Check with your child’s doctor if your child has any of the following:
- Fever.
- Easy bruising or bleeding.
- Petechiae (flat, pinpoint, dark-red spots under the skin caused by bleeding).
- Bone or joint pain.
- Painless lumps in the neck, underarm, stomach, or groin.
- Pain or feeling of fullness below the ribs.
- Weakness, feeling tired, or looking pale.
- Loss of appetite.
Tests that examine the blood and bone marrow are used to detect (find) and diagnose childhood ALL.
The following tests and procedures may be used to diagnose childhood ALL and find out if leukemia cells have spread to other parts of the body such as the brain or testicles:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Complete blood count (CBC) with differential: A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells and platelets.
- The number and type of white blood cells.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the sample made up of red blood cells.

- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow and bone under a microscope to look for signs of cancer.

The following tests are done on blood or the bone marrow tissue that is removed:
- Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of blood or bone marrow are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. For example, in Philadelphia chromosome–positive ALL, part of one chromosome switches places with part of another chromosome. This is called the “Philadelphia chromosome.” Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.

- Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of leukemia. For example, the cancer cells are checked to see if they are B lymphocytes or T lymphocytes.
- Lumbar puncture: A procedure used to collect a sample of cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs that leukemia cells have spread to the brain and spinal cord. This procedure is also called an LP or spinal tap.

- This procedure is done after leukemia is diagnosed to find out if leukemia cells have spread to the brain and spinal cord. Intrathecal chemotherapy is given after the sample of fluid is removed to treat any leukemia cells that may have spread to the brain and spinal cord.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. The chest x-ray is done to see if leukemia cells have formed a mass in the middle of the chest.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) depends on:
- How quickly and how low the leukemia cell count drops after the first month of treatment.
- Age at the time of diagnosis, sex, race, and ethnic background.
- The number of white blood cells in the blood at the time of diagnosis.
- Whether the leukemia cells began from B lymphocytes or T lymphocytes.
- Whether there are certain changes in the chromosomes or genes of the lymphocytes with cancer.
- Whether the child has Down syndrome.
- Whether leukemia cells are found in the cerebrospinal fluid.
- The child’s weight at the time of diagnosis and during treatment.
Treatment options depend on:
- Whether the leukemia cells began from B lymphocytes or T lymphocytes.
- Whether the child has standard-risk, high-risk, or very high–risk ALL.
- The age of the child at the time of diagnosis.
- Whether there are certain changes in the chromosomes of lymphocytes, such as the Philadelphia chromosome.
- Whether the child was treated with steroids before the start of induction therapy.
- How quickly and how low the leukemia cell count drops during treatment.
For leukemia that relapses (comes back) after treatment, the prognosis and treatment options depend partly on the following:
- How long it is between the time of diagnosis and when the leukemia comes back.
- Whether the leukemia comes back in the bone marrow or in other parts of the body.
Targeted therapy
Targeted therapy is a treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. There are different types of targeted therapy:
- Tyrosine kinase inhibitors (TKIs) are targeted therapy drugs that block the enzyme, tyrosine kinase, which causes stem cells to become more white blood cells or blasts than the body needs. Imatinib mesylate is a TKI used in the treatment of children with Philadelphia chromosome–positive ALL. Dasatinib and ruxolitinib are TKIs that are being studied in the treatment of newly diagnosed high-risk ALL.
- Monoclonal antibody therapy is a cancer treatment that uses antibodies made in the laboratory, from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. Blinatumomab and inotuzumab are monoclonal antibodies being studied in the treatment of refractory childhood ALL.
- Proteasome inhibitor therapy is a type of targeted therapy that blocks the action of proteasomes in cancer cells. Proteasomes remove proteins no longer needed by the cell. When the proteasomes are blocked, the proteins build up in the cell and may cause the cancer cell to die. Bortezomib is a type of proteasome inhibitor therapy used to treat relapsed childhood ALL.
New kinds of targeted therapies are also being studied in the treatment of childhood ALL.
See Drugs Approved for Acute Lymphoblastic Leukemia for more information.
More information: Benshang Li et al, Therapy-induced mutations drive the genomic landscape of relapsed acute lymphoblastic leukemia, Blood (2019). DOI: 10.1182/blood.2019002220
Journal information: Blood
Provided by St. Jude Children’s Research Hospital



{kind=link}