









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



In a world of seemingly endless opportunities for finding a mate, competition for a partner can be fierce. Not all that glitters is gold, as the old adage goes.
If you’ve long suspected that people fudge the truth when it comes to presenting themselves to a potential partner, here’s the research to back you up.
In a new study, published in the Journal of Experimental Social Psychology, two researchers from the University of Rochester’s Department of Clinical and Social Sciences in Psychology and the Israeli-based Interdisciplinary Center Herzliya conclude that when the possibility of sex looms, people are more likely to change their attitudes and engage in deceptive self-presentation.
In other words, they conform, embellish, and sometimes lie.
The duo of Gurit Birnbaum, a social psychologist and associate professor of psychology at the IDC Herzliya, and Harry Reis, a professor of clinical and social sciences in psychology and Dean’s Professor in Arts, Sciences & Engineering at the University of Rochester, hypothesized that sexual thoughts – or, in the researchers’ more precise terms, the activation of an individual’s sexual system – would increase a person’s efforts to manage first impressions, bringing with it deceptive self-presentation.
They tested that hypothesis on 634 students – 328 female and 306 male – with an average age of nearly 25, all identifying as heterosexual.
Over the course of four studies, the psychologists exposed one group to sexual stimuli and the control group to neutral stimuli.
Study participants, all students at an Israeli university, then interacted with an opposite-sex stranger.
Study 1 asked two study participants at a time to solve a dilemma faced by a fictitious third person – whether to accept a job offer abroad or to reject the offer to stay close to family and friends. Both participants were assigned one specific position – one for and one against the move abroad – to argue in a face-to-face interaction.
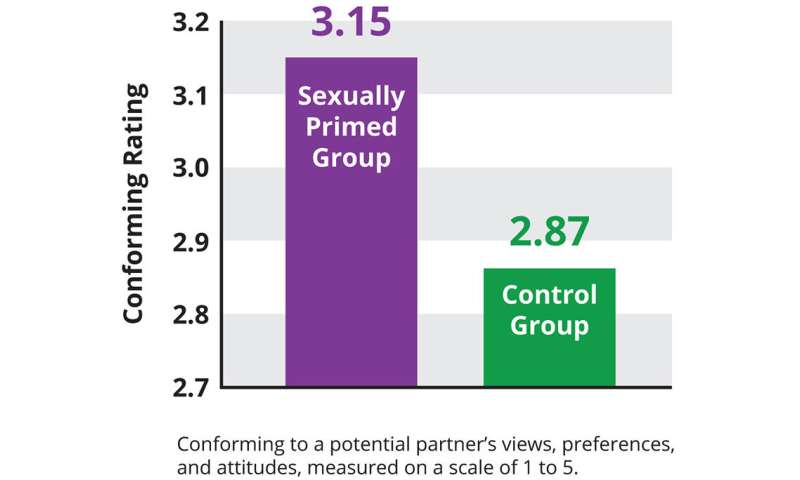
Afterwards, participants rated the extent to which they outwardly expressed agreement with the other participant’s position during the interaction. Compared to participants in the control group (without prior sexual stimuli), participants who had been sexually primed were more likely to express agreement with a contrary opinion advocated by an opposite-sex participant. The researchers interpret this behavior as a strategy to make a favorable impression with the stranger, thereby increasing the likelihood of getting closer to this person.
Study 2 examined whether study participants would actually change their declared preferences to conform to a stranger’s ideals.
Participants were asked to complete a questionnaire that assessed their preferences in various life situations (such as “to what extent does it bother you to date someone who is messy?” or “do you like to cuddle after sex?”).
Next, participants were subliminally exposed to either a sexual or a neutral picture prime.
Participants were then told they would be part of an online chat with another participant, who in reality was an insider – an opposite-sex member of the research team.
They looked at an online profile that purported to present the insider’s preferences on various subjects. After viewing the profile, participants were asked to create their own profile to be emailed to the other participant, and asked to complete their profile by rating the same items that had been presented in the insider’s profile.
The researchers found that even a non-conscious sexual stimulus (such as showing an erotic picture in a flash frame inside an otherwise neutral video) led participants to conform more to a potential partner’s preferences across various life situations.
“The desire to impress a potential partner is particularly intense when it comes to preferences that are at the heart of establishing an intimate bond,” writes the team. “Such attitude changes might be viewed as a subtle exaggeration, or as a harmless move to impress or be closer to a potential partner.”
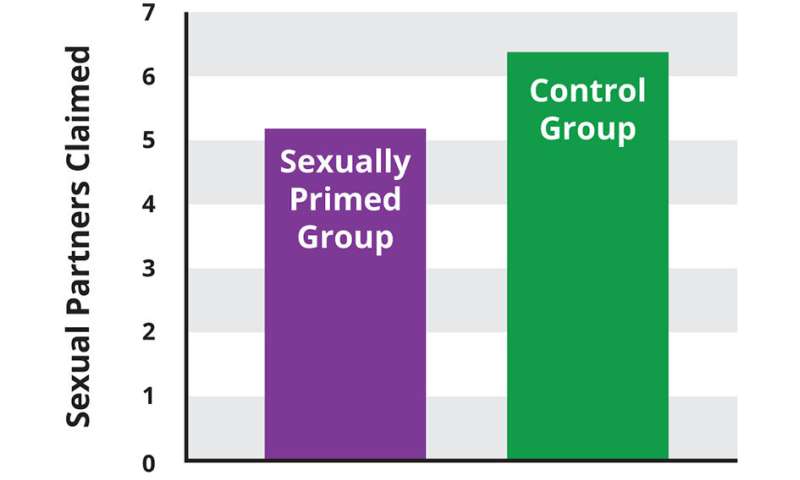
Studies 3 and 4 addressed whether participants would lie about the number of past sexual partners. The researchers hypothesized that people would reduce the actual number of partners so as to appear more selective – or less promiscuous – to a potential mate.
To test the hypothesis, researchers had participants talk about the total number of sexual partners they had had during a chat with an attractive study insider.
Then they were asked the same question in anonymous questionnaires to provide a true baseline for the researchers.
The findings were clear: study participants who had been sexually primed were more likely to lie, reporting lower numbers of previous sexual partners to a potential mate compared to the group without sexual priming.
The researchers found that both men and women (all of whom were sexually primed) tended to decrease the reported number of past sexual partners when chatting with an attractive stranger. (By the way, around seven previous partners was the magic number that most people reported in their doctored answers).
Interpreting the findings
Interestingly, Birnbaum and Reis, who have collaborated for decades (Birnbaum was a post-doctoral fellow in psychology at Rochester in 1998-99) have slightly different takes on what the findings ultimately mean.
“People will do and say just about anything in order to make a connection with an attractive stranger,” says Birnbaum. “When your sexual system is activated you are motivated to present yourself in the best light possible. That means you’ll tell a stranger things that make you look better than you really are.”
But, says Reis, “a lot of it is not necessarily what you’d call a bald-faced lie. Even though it’s clearly not the truth, it’s a way of people finding ways to emphasize different parts of how they see themselves.” And yet: “I think there’s some degree to which it is finding ways to shade one’s perception of the truth. It still counts as a lie, there’s no question about that.”
Sex on the brain
What laypersons might describe as having sexual thoughts, researchers refer to more precisely as the activation of the sexual system or sexual priming.
The phrase, Harry Reis explains, “means getting people to think about things in a sexual way. Technically it means activating a certain set of concepts in the brain. So, the parts of the brain that represent sexuality are being activated. But that doesn’t necessarily mean that people are getting genitally aroused.”
Attempts to slow the HIV epidemic worldwide have led to a clearer understanding that the battle is not simply about using condoms or adherence to medication. Rather, HIV risk and AIDS care involve complex behaviors influenced from multiple levels, from an individual’s knowledge, attitudes, emotions, and risk perception, to power dynamics between partners, accessibility of services, economic inequalities, criminalization of vulnerable groups, and policies that make HIV a priority health issue.1–3
Although there have been some calls to be more inclusive of multi-level factors beyond the individual level (e.g., at the interpersonal, network, institutional, or structural levels),4,5 evidence addressing a more holistic approach to changing HIV-related behaviors is limited.
Among such models, ecological models are a family of approaches seeking to describe the multiple levels of influence on individual behavior in the interest of creating environments conducive to health promotion.6
Although there seems to be little disagreement that ecological approaches are more comprehensive and potentially more explanatory and effective than frameworks or models only taking one level into account,7 such frameworks have received relatively little research attention, for at least three reasons.
First, assessing impact at multiple levels is often viewed as too difficult or expensive. For instance, an intervention in a low-income setting with the objective of increasing HIV counseling and testing may need to address
(1) the stigma of being tested and/or of testing positive;
(2) the quality of patient–counselor interactions;
(3) facility capacity, supplies, and environment; and
(4) access to those facilities by infrastructure, such as good roads and public transportation.
Addressing all of those factors and measuring improvements of each is extremely ambitious for any one research project. Even in an individual-focused intervention, addressing multi-level factors has its challenges.
Second, multi-level interventions are diverse and often context specific,8 and thus, it is not easy, or even appropriate, to replicate them. Nor do they easily support generalizations across contexts.9
For instance, a “structural” intervention for people who inject drugs in Ukraine (eg, needle exchange programs) would seem to have little in common with a structural intervention for poor women in Ethiopia whose financial dependence on men often results in transactional or cross-generational sex (eg, cash transfer).
Finally, with randomized controlled trials (RCTs) still viewed as the “gold standard” in health research, interventions addressing factors at multiple levels are often not attempted because an RCT is not feasible or even appropriate.10
Furthermore, combining individual-level and structural-level factors in one study is not straightforward.
For instance, Kippax10 argued that structural influences, such as political will to implement harm reduction strategies or funding for mass media to lead public discussions about sensitive HIV-related topics, have a determining impact on HIV transmission and the likelihood that individual- or interpersonal-level interventions will succeed. But political will and vibrant mass media are rarely amenable to evaluation through an RCT, as the meta-analysis by Lacroix et al.11 in this special issue documents.
Multi-level approaches, thus, are in many ways at odds with contemporary HIV-related policy, which often favors brief, replicable, and easily disseminated interventions. Individual-level or interpersonal-level interventions are most amenable to such constraints. However, this article is guided by the current literature and theory, rather than by policy constraints.
Indeed, it is in line with simultaneous policy shifts (contradictory to the emphasis on brevity and replicability) in favor of structural interventions. Although the field of behavior change research in HIV seems to accept that change means going beyond the individual level,4 there is still only a small literature on models taking multi-level approaches. This article aims to contribute to the shift to a more holistic approach by synthesizing and making sense of a complex literature, leading us to outline the next steps required as clearly as possible. Specifically, we
(1) list potentially relevant variables/factors related to behavior change at all levels of the individual–structural spectrum,
(2) identify characteristics of important recent multi-level models and compare them,
(3) identify challenges in using such models, and
(4) identify next steps and make actionable recommendations.
A Menu of Behavior Change Factors
Figure Figure11 provides a menu of the various influences on behavior change at each level of the socio-ecological framework based on our review of existing literature on behavior change interventions related to HIV prevention, treatment, and care. The individual level includes factors comprising the micro-level, such as individual perceptions, beliefs, or emotions. The interpersonal/network level includes dyadic or family influences, such as relationship satisfaction or social support.
The community level includes influences at a larger group level, such as social capital or community norms. The institutional level focuses on factors within the health system, such as quality of service providers, confidentiality, or sufficient resources.
Finally, the structural level includes the most macro-level factors affecting behavior, such as the economy, political climate, enforcement of policies and laws, or funding environment. Some structural factors may be more removed from individual control than others.
For instance, wars, famines, or droughts are important structural factors further removed from the individual than, for instance, the availability of transport to access a clinic or income-generating opportunities in a particular community. Moreover, although we distinguish between “levels,” they are highly interactive, with processes ranging between micro and macro. Structural influences function only with the cooperation of individuals and their interpersonal relationships, and vice versa.

Many of these factors have been extensively researched and incorporated into successful interventions (eg, self-efficacy, behavioral skills, stigma reduction) while others have been discussed as important factors without much evidence to date on how they can be leveraged for behavior change (eg, emotions, sexual relationship power, community mobilization). The figure provides citations to key articles evidencing or arguing for each factor, where available.
The purpose of this figure is to provide an overview of the diverse influences relating to HIV risk or AIDS care. The figure does not represent a theory of the relationships among the variables at the different levels of analyses, nor can it be used to determine which variables might be most important to address in a particular intervention.
Nonetheless, it does highlight some variables that have only recently been investigated, such as emotions,12,13 social networks/coalitions/capital,14 and relationship investment.15 Moreover, in recent years, theoretical models have begun to conceptualize how these variables and levels are linked together.
Recent Theoretical Frameworks Addressing Multi-Level Factors
Many individual-level theories have played prominent roles in past behavioral interventions focused on HIV prevention and AIDS care, including especially Social Cognitive Theory,16,17 the Theories of Reasoned Action18 and Planned Behavior,19 the Transtheoretical Model,20,21 and the Information, Motivation, Behavioral Skills Model22 (Table (Table1).1).
Although these models primarily focus on the individual level, they have been associated with significant behavior change across a range of groups with varying risk levels (eg, men who have sex with men, adolescents, people living with HIV/AIDS, African Americans23–28).
Nonetheless, reviews of such models have concluded that, because they do not explicitly consider high-level connections, their success is constrained.29 Of note, meta-analyses of behavioral intervention trials routinely find that inconsistencies in study outcomes cannot be explained solely on the basis of moderators stemming from individual-level theories23−28; until recently, these meta-analyses have rarely considered factors outside the intervention itself in efforts to explain heterogeneity.
Several recent models have taken up the challenge of expanding from individual-level features to be inclusive of higher levels. The Multiple Domain Model (MDM)30 proposes that there are multiple domains of influence on health behavior, with situational/contextual variables being the most proximal to behavior, followed by preparatory behaviors, behavioral intentions, normative, attitudinal, and self-efficacy beliefs, personality and social environmental factors, and finally social structural variables. Essentially, the MDM starts with the
Theory of Planned Behavior, replacing perceived behavioral control with self-efficacy. It then adds structural factors in the sociological sense (race, gender, age, social class) and variables that address personality, the social environment (school connectedness or family relationships), and social situational variables (substance use, relationship status, or hormonal contraceptive use).
The MDM allows each of these to have direct (not merely indirect) relationships with behavior. Hence, factors outside of the individual are explicitly modeled as factors shaping one’s behavior.
Three recent efforts embraced ecological frameworks as an overarching theme. First, the Network-Individual-Resource Model (NIRM) recognizes and addresses the substantive reciprocal ties of individuals and important social networks across their lifespans—ties that have their basis in the tangible and mental resources individuals and networks possess.29
Second, the Dynamic Social Systems Model (DSSM)31 conceptualizes resources, science and technology, formal social control, informal social influences and control, social interconnectedness, and settings as aspects that dynamically intersect to create structural realities ranging from micro- to meso- to macro-levels.
Third, the Transmission Reduction Intervention Project (TRIP)32 rests explicitly on the fact that HIV transmission requires body fluid exchange and is spread through community sexual and injection networks. Current expositions related to TRIP emphasize the need to simultaneously intervene at higher levels than the individual (eg, care providers) and rectify power imbalances (eg, ensure they understand patients’ social and economic realities).
All 4 multi-level approaches concur that factors outside the individual relate to risk and the ability to change behavior. For example, a great deal of recent research confirms that social stigma creates health risks and worsens health care.33,34 The DSSM, TRIP, and NIRM agree in focusing on resources as critical for sustaining behavior change; they also emphasize power dynamics between individuals and surrounding social forces.
The DSSM and NIRM also agree in focusing on the dynamic interplay between levels, although the former focuses only on the structures people face and the latter implies reciprocal interactions between individuals and realities constructed by networks. To the NIRM, networks cannot exist without individuals and vice versa. The MDM and the NIRM agree in emphasizing social environmental factors directly influencing behavior, even when the individual may wish to act differently.
The NIRM is the only 1 of these 4 models directly addressing development across the lifespan, which characterizes both individuals and networks. Thus, the NIRM holds that prevention needs, and risk itself, depend importantly on the life stage and circumstances. Individuals with great needs or little autonomous power (eg, infants and children) are vulnerable to others’ influence and can be positively (eg, sustenance from caregivers) or negatively affected (eg, harmed by poor care). In parallel, networks that might improve health gain strength when more individuals actively participate in them and promote their goals.
Finally, of these models, TRIP and the NIRM most embrace the perspective that individuals must find ways to cope with stressors. In short, one reason behavior change efforts may fail is because those addressed by an intervention live in circumstances filled with stressors such as demanding physical environments or stigmas associated with minority status, HIV-positive status, or both.
Reid et al35 recently showed that both residential segregation and prejudice levels of majority members toward minorities interfered with the success of behavioral interventions meant to decrease sexual risk behaviors.
Logically, the stress created by unfriendly social environments—in this case addressed at the U.S. county level—interfered with individuals’ ability to improve habits. Understanding how to promote positive coping with environmental stressors and how to make communities more supportive would thus offer considerable hope for larger behavior change effects.
Table Table11 compares recent behavior change models and how they attempt to address factors beyond the individual. Because individual and structural elements clearly are relevant to HIV risk and transmission prevention, a strength of the NIRM is that it recognizes the linkage between levels, where micro connotes processes or variables solely within individuals, and macro implies linkages between individuals and others.36
Thus, the NIRM recognizes that individuals (micro) enact risk behaviors with those to whom they are linked in networks (macro). In contrast, individual-level HIV prevention theories either have no explicit linkage to macro-levels or do so only indirectly. Finally, the individual-level models have little ability to explain structural influences, whereas the other 4 models at least permit a direct influence of such factors on risk behavior.
The NIRM and TRIP recognize that networks or organizations possess resources that bear on risk behavior; the NIRM explicitly addresses how networks create structural realities that interplay with risk. Although addressing these high-level factors creates challenges for brevity and replicability, doing so is more likely to result in sustainable behavior change.
Because these multi-level models are all relatively new, there have not been extensive empirical studies evaluating their assumptions. Another consideration in our discussion is that various versions of socio-ecological models have typically been discussed as organizing frameworks rather than as testable (ie, falsifiable) empirical models.
Indeed, at this writing, of the broader, relatively new models we discuss here, we are aware of research supporting predictions only of the MDM and the NIRM. MDM research so far has generally shown that situational and preparatory behaviors add significant predictive power for behavior beyond attitudes, norms, intentions, and self-efficacy.
The MDM research also suggests that social–structural variables (eg, gender, age, socioeconomic status) seem to have primarily indirect effects on behavior through attitudinal and situational factors.28,37,38 NIRM-related meta-analyses have supported its hypotheses: (1) individual resources are crucial to the success of interventions (eg, interventions were more successful if they also reduced depression39) and (2) the structural dimensions of economic resources and community support in the locales where individuals are targeted by health promotion relate to the success of these efforts.11,35,40,41
Only time will tell whether DSSM and TRIP function more as organizing frameworks or begin to be tested empirically. Finally, we have also noted that evaluating multi-level theories is routinely more complex than evaluating individual-level theories.
More information: Gurit E. Birnbaum et al, Making the right first impression: Sexual priming encourages attitude change and self-presentation lies during encounters with potential partners, Journal of Experimental Social Psychology (2019). DOI: 10.1016/j.jesp.2019.103904
Journal information: Journal of Experimental Social Psychology
Provided by University of Rochester



{kind=link}