










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



About 1.6 million people in the US alone currently have lifelong and incurable Inflammatory Bowel Disease (IBD) including Crohn’s disease and ulcerative colitis, and 70,000 new cases are diagnosed in the USA each year.
IBD patients suffer from pain, extreme discomfort, and many other symptoms caused by continuously relapsing and remitting inflammatory lesions in the layer of cells that lines the intestinal lumen (mucosa).
The exact causes for IBD still are poorly understood, but it is clear that a misdirected immune system is at work, and that certain components of the microbial community in our gut, known as the intestinal microbiome, and environmental factors contribute to its destructive forces.
While anti-inflammatory drugs can dampen acute inflammation and antibiotics can fight local infections when IBD episodes flare up, their use also comes at a cost.
Anti-inflammatory drugs can have severe side effects and antibiotics can disrupt the beneficial parts of the microbiome on which we depend for many of our body’s functions.
Importantly, there are no wound treatments available that could be applied to inflamed lesions directly from inside the gut lumen in order to speed up the healing process and minimize the use of those drugs.
Now, a research team at Harvard’s Wyss Institute for Biologically Inspired Engineering led by Neel Joshi, Ph.D., has developed a living material approach that uses a strain of genetically engineered E. coli Nissle gut bacteria as a locally acting probiotic.
The engineered bacteria produce a network of nanofibers that directly binds to mucus to fill inflamed areas like a patch, shielding them from gut microbes and environmental factors.
This probiotic-based therapeutic strategy protected mice against the effects of colitis induced by a chemical agent and promoted mucosal healing. Their findings are reported in Nature Communications.
“With this ‘living therapeutics’ approach, we created multivalent biomaterials that are secreted by resident engineered bacteria on-site and attach to many mucus proteins at a time—firmly adhering to the viscous and otherwise moving mucus layer, which is a challenging thing to do,” said Joshi.
“The ‘Probiotic Associated Therapeutic Curli Hybrids’ (PATCH) approach, as we named it, creates a biocompatible, mucoadhesive coating that functions as a stable, self-regenerating Band-Aid and provides biological cues for mucosal healing.” Joshi presently is a Core Faculty member of the Wyss Institute and Associate Professor at Harvard’s Paulson School of Engineering and Applied Sciences (SEAS), and will shortly be appointed as a Professor at Northeastern University in Boston.
In previous work, Joshi’s group has demonstrated that self-regenerating bacterial hydrogels firmly attached to mucosal surfaces ex vivo, and, when orally given to mice, withstood the harsh pH and digestive conditions of the stomach and small intestine without affecting the health of the animals.
To fabricate them, his team programmed a laboratory E. coli strain to synthesize and secrete a modified CsgA protein, which as part of E. coli’s “curli” system assembles into long nanofibers at the outer surface of the bacteria.
“To enable mucus adhesion, we fused CsgA to the mucus-binding domain of different human trefoil factors (TFFs), proteins that occur naturally in the intestinal mucosa and bind to mucins, the major mucus proteins present there.
The secreted fusion proteins form a water-storing mesh with tunable hydrogel properties,” said co-author Anna Duraj-Thatte, Ph.D., a postdoctoral fellow working with Joshi.
“This turned out to be a simple and robust strategy to produce self-renewing, mucoadhesive materials with long residence times in the mouse intestinal tract.”
In their new study, the team further built on these findings by introducing the machinery for producing one of the mucoadhesive hydrogels based on TFF3 into an E. coli Nissle strain that is a normal gut bacterium which can thrive in the colon and cecum sections of the intestinal tract affected by IBD, and is currently sold in many commercial probiotic formulations.
“We found that the newly engineered Nissle bacteria, when given orally, also populated and resided in the intestinal tract, and that their curli fibers integrated with the intestinal mucus layer,” said first-author Pichet Praveschotinunt, who is a graduate student mentored by Joshi.
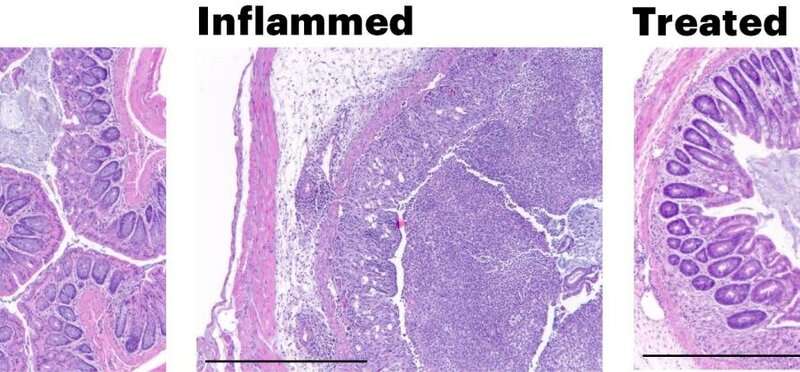
“When we induced colitis in the colons of mice by orally administering the chemical dextran sodium sulfate, animals that had received the PATCH-generating E. coli Nissle strain by daily rectal administration starting three days prior to chemical treatment, had significantly faster healing and lower inflammatory responses, which caused them to lose much less weight and recover faster compared to control animals,” said Praveschotinunt.
“Their colon epithelial mucosa displayed a more normal morphology and lower numbers of infiltrating immune cells”.
Joshi and his team think that their approach could be developed as a companion therapy to existing anti-inflammatory, immuno-suppressant, and antibiotic therapies to help minimize patients’ exposure to the drugs and potentially provide protection against IBD relapses.
“This powerful and simple approach could potentially impact the lives of thousands of patients with IBD for whom there is no disease-specific cure available.
It also is a testament to the creativity and vision of the Wyss Institute’s “Living Cellular Devices” initiative that engineers living cells to perform key therapeutic and diagnostic tasks in our bodies,” said Wyss Institute Founding Director Donald Ingber, M.D., Ph.D., who is also the Judah Folkman Professor of Vascular Biology at HMS, the Vascular Biology Program at Boston Children’s Hospital, and Professor of Bioengineering at SEAS.
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), is a type of chronic bowel inflammation diseases that relapse episodes with unknown aetiology.[1,2] It has been widely accepted that IBD is the consequence of overly activated response of mucosal immune system to the environmental, dietary, or infectious antigen in a genetically susceptible host.[3] Studies on the animal models have indicated that aggressive cell-mediated immune caused by commensal enteric bacteria plays a vital role in the development and maintenance of IBD.[4,5]
Evidence from patients also showed innate immune system would be activated and aberrant immune response would be initiated through secreting inflammatory mediators caused by endogenous bacterial flora, which would result in IBD.[6]
Therapy of IBD often involves induction of remission and prevention of relapses.[7,8] Corticosteroids are initially used to induce remission, but the maintenance is often less successful, and patients treated with long time corticosteroids may suffer several complications including growth failure or osteopenia.[9] Guidelines[10] have recommend aminosalicylates as a maintenance treatment. Clinical treatment with aminosalicylates for patients with IBD is well established to maintain remission.[11]
But also the effect is contentious and some potential complications are observed, such as infection, hepatitis, leucopenia, and pancreatitis.[12,13] Modification of the bacterial microenvironment in bowel is another therapy to induce or maintain remission in IBD.[14,15]
Using antibiotics to remove the bacteria with potential inflammatory is a seemingly feasible solution, but the use of antibiotics is limited.[16,17] Another option is to use probiotics which could solve inflammation though improving its intestinal microbial balance.[18]
Probiotics are live microorganisms that intend to provide positive efficacy on the treatment of traveler’s diarrhea, diarrhea caused by the human immunodeficiency virus, and difficile colitis relapses.[19,20] After ingested, probiotics could inhibit the overgrowth of potentially pathogenic bacteria to modify the composition in bowel, which have beneficial effects on human health.[21]
Several animal models have proved the effectiveness of probiotic therapy for patients with IBD.[22] For patients, some studies have also conducted with Escherichia coli Nissle 1917 (EcN 1917), Saccharomyces boulardii and VSL#3, and these yeasts have been reported to have some beneficial effects in IBD.[23–25]
Despite the fact that several studies have studied the effect of different probiotics, inconsistent results about the therapeutic efficacy of probiotics have been reported. This study is aimed to evaluate the effect of probiotics to maintain remission and cause complication in IBD patients.
Discussion
Until now, there have no standard therapy for IBD and the most common treatment option is to establish systemic or topical immunoregulation with mesalazine or sulfasalazine, which could reduce the associated risk of cancer in bowel.[37,38]
Unfortunately, previous studies have reported several serious adverse effects about the use of mesalazine after long time follow-up[39,40]; thus an alternative therapy is required. It has been reported that almost 40% of adults and children who suffered with IBD have treated with alternative therapies such as probiotics, which may mediate the inhibition of nuclear factor kB.[41,42]
Organisms present in probiotic preparations include S boulardii, Lactobacillus GG, EcN 1917, and VSL#3. S boulardii has been showed the prevention of recurrences on Clostridium difficile infection, and animal models have reported the effects in IBD.[43,44] There were few data about the effect of S boulardii on patients with IBD, but the reduction of clinical features about inflammation and reinforcement of intestinal epithelial barrier were observed in previous studies.[45–47] Lactobacillus GG (LGG) has been used as the treatment of rotavirus, acute diarrhea, and atopic disease in at-risk infants.[48,49]
It could modify bacterial flora in human bowel. EcN 1917 is one of the most common strains used as probiotics in IBD patients, and the specific characteristics like the unique structure of lipopolysaccharide and biofilms formation in different conditions make it survive in the gut.[50,51] VSL#3 consists of 8 different bacterial species, which has been shown to be effective in infection disease, such as chronic pouchitis.[52,53]
In our study, we preformed meta-analyses of the remission, relapse, and complication rate between EcN 1917 and mesalazine. Although safe and well tolerated, there was no significant difference either in the EcN1917 group or among patients treated with mesalazine. Generally, experiment-control studies are presented to test the difference.
However, due to the fact that mesalazine has been regarded as the established gold standard therapy, the results in our study were aimed to demonstrate the equivalence. The meta-analyses suggested that EcN1917 provided similar efficacy in remission, relapse and complication rate compared with mesalazine.
We also conducted the comparison of the efficacy between IBD patients treated with probiotics and placebo. All the combined results about the efficacy in remission, relapse, and complication rate showed no significant difference between probiotics and placebo groups. As 3 types of probiotics including S boulardii, Lactobacillus GG and VSL#3 were involved in the meta-analyses, the subgroup analyses were conducted.
Though no difference was observed in remission rate of Lactobacillus GG, VSL#3 showed higher remission rate than that of placebo group (RR = 1.67, 95%CI[1.06, 2.63]). Both S boulardii and Lactobacillus GG showed similar result about the relapse rate in subgroup mate-analysis, but the relapse of patients with placebo showed higher rate than VSL#3 (RR = 0.29, 95%CI[0.10, 0.83]). The frequency of complications was similar in all subgroups. The side-effects motioned in the studies were relatively minor including diarrhea, abdominal pain, arthralgia, bdominal bloating, and some discomfort.
In summary, EcN 1917 has a similar efficacy with the mesalazine, the commonly used drug for IBD patients. While both S boulardii and Lactobacillus GG showed no advantage compared with placebo, the mixed probiotics, VSL#3, presented better results.
There were some potential limitations in this study. Some high heterogeneity was observed in the meta-analyses. As subgroup analysis has been conducted, high heterogeneity was attributable to the different types to some extent. Few articles have been involved in our studies and few patients were enrolled in the trials, which could generate the possibility of bias. Besides, some other parameters of the patients could influence the result of the treatment and increases the risk of flare-up.[54] Future studies with high quality about the different probiotics used to IBD patients should be conducted.
More information: Pichet Praveschotinunt et al, Engineered E. coli Nissle 1917 for the delivery of matrix-tethered therapeutic domains to the gut, Nature Communications (2019). DOI: 10.1038/s41467-019-13336-6
Journal information: Nature Communications
Provided by Harvard University



{kind=link}