










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Heart disease remains the largest killer in Australia and around the world.
A new study has shown that a protein therapy- recombinant human platelet-derived growth factor-AB (rhPDGF-AB) – could improve outcomes following heart attack.
After a heart attack, scar tissue forms and this negatively affects heart function. Now, researchers from The Westmead Institute for Medical Research (WIMR) and the University of Sydney found that, infusing rhPDGF into subjects that have had heart attacks improves the quality of the scar, leads to the formation of new blood vessels in the heart, and reduced rates of dangerous heart arrhythmia (irregularities of heart rhythm that can cause sudden death).
This study was in a pre-clinical large animal model.
The discovery publishes today in the leading journal Science Translational Medicine.
Corresponding author who led the research team, Associate Professor James Chong, said: “This is an entirely new approach with no current treatments able to change scar in this way.
“By improving cardiac function and scar formation following heart attack, treatment with rhPDGF-AB led to an overall increase in survival rate in our study.
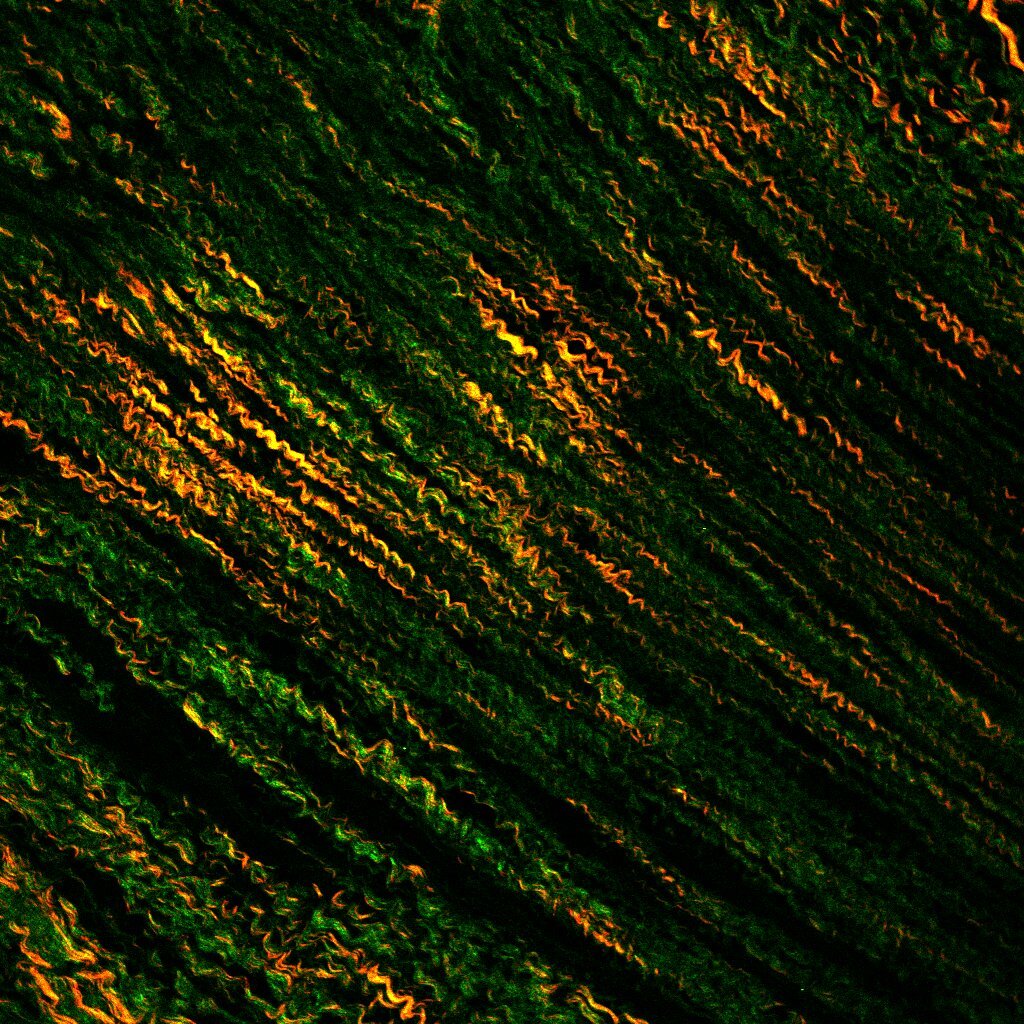
“While the treatment did not affect overall scar size, importantly we found that rhPDGF-AB led to increased scar collagen fibre alignment and strength. This improved heart function after the heart attack.
3D microscope image showing better blood vessel formation after PDGF treatment following heart attack. Credit: Dr Robert D Hume
“Our collaborator Professor Richard Harvey,from the Victor Chang Cardiac Research Institute, had previously shown that the protein can improve heart function in mouse models following heart attack.
“This project has been developed over more than 10 years and we now have compelling data in two species for the effectiveness of this treatment.
Following heart attack, the heart muscle is damaged, causing thick scar tissue to form. This can limit the heart’s ability to function efficiently, and can increase the risk of heart failure, and sudden cardiac death.
Current treatments aim to restore blood and the oxygen supply to the heart as quickly as possible to reduce scarring. While this improves clinical outcomes, up to a quarter of patients experiencing their first heart attack will develop heart failure within one year.
Associate Professor Chong said: “While we have treatment protocols in place, it’s clear that there is an urgent, unmet need for additional treatments to improve patient outcomes particularly after large heart attacks.
Heart MRI showing better heart function after PDGF treatment. Credit: Prof Stuart M Grieve
“Heart disease is the leading cause of death in Australia. It is thought that more than 400,000 Australians have had a heart attack at some stage in their lives and that there is roughly one heart attack every 10 minutes.
Through our research, we have the opportunity to change the negative impact of these statistics.
“Some further animal studies are required to clarify safety and dosing. Then we can start looking towards clinical trials in humans very soon. rhPDGF-AB is clearly a promising therapeutic option, and could potentially be used alongside existing treatments to improve heart attack patient outcomes and survival rates.
“We now hope to further investigate the treatment, including whether it could be used in other organ systems impacted by scar tissue, such as the kidneys.”
Extensive evidence has demonstrated an association between negative emotions, social factors, and certain chronic stress conditions and adverse cardiac outcomes.1 Less well studied has been the potential association between positive and negative mindsets and cardiac risk. Such research is of interest because mind-sets are potentially modifiable, thus making them a novel relevant target for clinical intervention.
One such mindset is an individual’s level of optimism, commonly defined as the tendency to think that good things will happen in the future.2 Empirical studies have long indicated that more optimistic individuals are more likely to succeed at work and in school, sports, politics, relationships, and other forms of life endeavors.3,4
A more recent study also reported positive associations between optimism and a range of favorable physical health outcomes.5 Nevertheless, the assessment of optimism and pessimism in cardiac medical practice is uncommon.
In 2001, Kubzansky and colleagues6 reported the first study, to our knowledge, to find an association between higher optimism and a lower risk for specific cardiac outcomes, including angina, myocardial infarction, and cardiac death.
They showed effects of optimism beyond those of depression or other forms of psychological distress, a critical finding because a concern about such findings is that they simply reflect the absence of depression rather than active effects of optimism.
Since then, similar findings have been described in other studies,7–20 and most studies considered depression or distress as a potential confounder. To consider these findings more systematically, we conducted a meta-analysis of studies that have assessed the association between optimism and pessimism and adverse cardiac outcomes.
Our goals were to evaluate the magnitude of this association, the consistency of results among reported studies, the influence of potential confounders, and the quality of the reported literature.
ResultsStudy Characteristics
A flow diagram of the literature search and related screening process is shown in Figure 1. A total of 15 studies6–20 published between November 2001 and January 2017 met our inclusion criteria. Of these, 14 were prospective studies and 1 was a retrospective cohort study.8 Overall characteristics of the included studies, which comprised 229 391 individuals, are summarized in Table 1.
Of the 15 studies, 8 were conducted in the United States,6–8,11,15–17,19 5 in Europe,10,12–14,18 1 in Israel,20 and 1 in Australia.9 Ten studies reported data on cardiovascular events,6,10,11,13–19 and 9 studies reported data on all-cause mortality.7–9,11–13,17,19,20 The mean follow-up period was 13.8 years (range, 2-40 years). With the exceptions of a study that assessed ambulatory patients8 and another that assessed patients who had previous myocardial infarction,20 all studies were performed in community cohorts of different ages. Mean age at baseline assessment ranged from 19 to 93 years. Details regarding how exposures and outcomes were assessed in the included studies are shown in eTable 1 in the Supplement. A variety of scales were used to assess optimism and pessimism. The most frequently used (in 8 of 15 studies) scale was the Life Orientation Test–Revised.28 All studies had a low risk for bias per the Newcastle-Ottawa scale (eTable 2 in the Supplement).Optimism and Incident Cardiovascular Events
The 10 studies reporting on cardiovascular events included 209 436 participants. On pooled analysis, optimism was significantly associated with reduced risk of cardiovascular events (RR, 0.65; 95% CI, 0.51-0.78; P < .001) (Figure 2). A high heterogeneity was observed in the analysis (I2 = 87.4%). Exclusion of the study by Tindle et al,19 the largest study, did not result in any change in the pooled result (RR, 0.63; 95% CI, 0.48-0.78; P = .001). Visual inspection of the funnel plot showed evidence of publication bias (smaller studies showing no beneficial effects were missing). According to the trim-and-fill method, the association between optimism and cardiovascular events remained significant after imputing 4 possible missing studies (adjusted RR, 0.77; 95% CI, 0.61-0.92; P < .001) (eFigure in the Supplement).Optimism and All-Cause Mortality
The 9 studies (10 comparisons) reporting on all-cause mortality included 188 599 participants. On pooled analysis, optimism was significantly associated with reduced risk of all-cause mortality (RR, 0.86; 95% CI, 0.80-0.92; P < .001) (Figure 3). Moderate heterogeneity was observed in the analysis (I2 = 73.2%). Exclusion of the study by Tindle et al19 did not result in any change in the pooled result (RR, 0.86; 95% CI, 0.79-0.93; P < .001).
Visual inspection of a funnel plot showed evidence of publication bias. According to the trim-and-fill method, the association between optimism and all-cause mortality remained significant after imputing 4 possible missing studies (adjusted RR, 0.90; 95% CI, 0.83-0.97; P < .001) (eFigure in the Supplement).Subgroup Analysis
Subgroup analysis by method of assessment for optimism, follow-up duration, sex, study location, depression, educational level, socioeconomic status, and exercise or physical activity yielded largely similar results for the associations between optimism and pessimism and the risk for either cardiovascular events or all-cause mortality (Table 2).Assessment of Linear Trend
Among the 15 studies, optimism and pessimism were assessed solely as a continuous variable in 2 studies.7,9,11 In the other 13 studies, participants were divided into either tertiles or quartiles and a statistical assessment was performed regarding the presence or absence of a significant linear trend between levels of optimism and reduced risk for cardiac events and/or all-cause mortality (eTable 1 in the Supplement). In 12 of 15 studies, a significant linear trend was observed.Discussion
A review of the literature has noted associations between a number of psychosocial risk factors, including negative emotions such as depression and anxiety, social factors (eg, loneliness), and certain chronic stress conditions, with cardiovascular disease. Specific mindsets, habitual patterns of thinking which influence individuals’ views and interactions, have also been associated with cardiovascular disease risk.
Using the strongest epidemiologic methods available, a growing body of research has investigated whether the mindset of optimism vs pessimism might be associated with cardiovascular disease and has also explored potential mechanisms underlying these associations. Herein, we report the results of a comprehensive systematic review and meta-analysis to assess the association between optimism and pessimism and adverse cardiovascular outcomes.
This meta-analysis consisted of 15 studies6–20 involving 229 391 participants. Ten of the studies assessed the association between optimism and pessimism and adverse cardiovascular outcomes. In 9 of 10 studies,6,10,11,13–19 there was a significantly lower risk of cardiovascular events among individuals with high optimism scores after adjustment for a variety of clinical measures in each study.
The overall pooled risk ratio for cardiovascular events among individuals with high optimism levels was 0.65. Among 9 studies,7–9,11–13,17,19,20 optimism was also associated with a reduction in all-cause mortality, but the decrease in risk was more modest, with an overall pooled risk ratio of 0.86. As with cardiovascular events, the results among studies were consistent, with 8 of 9 studies showing lower risk of all-cause mortality among the most optimistic individuals.Methodologic Differences Among Studies
There was considerable variation in questionnaires used to assess optimism and pessimism. Most studies queried dispositional optimism, with the Life Orientation Test–Revised28 most commonly used (in 8 of 15 studies). Three studies6–8 used an explanatory style measure of optimism derived using items from the Minnesota Multiphasic Personality Inventory,whereas 2 studies10,12 used a single-item measure. Despite this heterogeneity in how optimism was assessed, the lower RR that was associated with optimism was comparable among studies. Studies also varied by length of follow-up.
Among the 15 studies, participants were followed for at least 10 years in 8 studies.6–9,12,14,15,20 A significantly lower risk of cardiovascular events and all-cause mortality was observed across studies regardless of follow-up duration.Assessment of Potentially Confounding Variables
In general, the risk ratios used for this meta-analysis were adjusted for a variety of potentially confounding clinical variables. Most studies adjusted for some if not all major cardiac disease risk factors. Many studies also adjusted for psychological distress to rule out concerns that associations were primarily attributable to the absence of depression, and approximately half of the studies presented estimates also adjusted for educational level and physical activity.
Protective effects of optimism were maintained among studies adjusting for these variables. In addition, optimism was associated with comparably reduced risk among studies with a predominance of men vs women and among studies conducted in the United States vs other countries.Assessment of Outcomes According to the Magnitude of Optimism and Pessimism
Optimism was generally assessed according to continuous scales that used multi-item measures, with associations generally estimated according to tertiles or quartiles of optimism. In the 2 studies assessing optimism and pessimism by a single question, participants were divided into 3 categories based on their responses, with comparisons made between the highest vs lowest categories. Evidence of a dose-response association between level of optimism and decreased clinical risk was present in 12 of 15 studies.
In 2 of the 3 studies without evidence of a dose-response association,10,15 the optimism assessment was limited with measures including only 1 or 2 items. The evidence of dose-response associations paralleled similar findings reported for the clinical hazard of cardiovascular outcomes associated with depression, poor social support, and other psychosocial risk factors.1Comparison With Studies of Optimism and Other Medical Conditions
Our study was the first meta-analysis, to our knowledge, to assess the association between optimism and clinical outcomes. Findings were consistent with studies17,29–31 that have evaluated the association between optimism and other related medical conditions.
This includes studies that have shown an association between optimism and the risk of heart failure,29 development of cognitive dysfunction among elderly persons,30 rate of atherosclerotic progression,31 and respiratory disease, infection, and various cancers.17
In addition, a previous meta-analysis found consistent associations between optimism and a reduced likelihood of various other adverse physical health outcomes.5 Combined, these data support the findings of our meta-analysis.Mechanisms
Psychosocial risk factors tend to exert their adverse effects by both indirect behavioral mechanisms and direct physiologic mechanisms.32
Accumulating data suggest that similar mechanisms may be associated with the presence of optimism and pessimism. With respect to behavioral mechanisms, Boehm and colleagues33 conducted a random-effects meta-analysis to examine the association between optimism and 3 cardiac-relevant health behaviors: physical activity, diet, and cigarette smoking.
The study33 found a positive association between optimism and better health behaviors, although most evidence was cross-sectional and effect sizes were modest. More recently, however, larger studies34–37 with prospective designs have found significant associations between measurement of initial optimism and pessimism levels and subsequent health behaviors. For instance, among participants in the Women’s Health Initiative, greater optimism was associated with both better diet quality34 and a greater likelihood of sustaining physical exercise over time.35
Studies have also reported associations between optimism and pessimism and a variety of pathophysiologic mediators of chronic disease, including increased inflammation and impairments in hemostasis and endothelial function38,39; metabolic function40; telomerase activity and telomere length41–43; ambulatory blood pressure44; and hypothalamic-pituitary-adrenocortical function.45–47
Together, these findings suggest a direct association of optimism vs pessimism with physiologic functioning, although study of individual mediators remains sparse compared with the study of more established psychosocial mediators, such as depression. Prospective study is needed to evaluate whether pessimism is a stronger contributor to pathophysiologic dysfunction (as suggested by some studies38,40,43) than optimism is for providing positive physiologic buffering.Clinical Significance
Optimism has long been promulgated as a positive attribute for living. The findings of the current meta-analysis suggest that optimism is associated with cardiovascular benefits and that pessimism is associated with cardiovascular risk, with a pooled association that was similar to that for well-established cardiac risk factors.
Taken together, the cardiovascular and psychological benefits of optimism make it an attractive new arena for study within the field of behavioral cardiology. The success of this research may require addressing 3 key issues. First, there is a need to define more clearly the central processes that underlie the medical benefits associated with optimism.
This should include more study into the physiological processes and health behaviors that may ensue from optimism vs pessimism as well as the study of potential salutogenic mechanisms that may cotravel with optimism vs pessimism.
With respect to the latter, a study48 reported an association of optimism with more effective goal setting, problem solving, and coping skills, suggesting that these are potential assets related to optimism that could be incorporated into the measurement of optimism and/or form the basis of clinical intervention.
Second, the studies of our meta-analysis were associated with substantial variability in the cut points that were applied to optimism vs pessimism. This variability differs from the use of depression scales, whereby specific diagnostic cut points have been established. For instance, screening for depression, as advocated by the American Heart Association, has been made possible because of the development of widely accepted criteria for defining depression risk based on the 2- and 9-item General Health Questionnaire.
A similar consensus in diagnostic criteria could improve future epidemiologic investigations regarding optimism and pessimism and is needed for use as a clinical assessment tool in medical practice. To this end, emerging data suggest that the Life Orientation Test–Revised, as developed by Scheier and colleagues,28 may be a suitable screening tool given its brevity and successful use across many clinical outcomes.
Third, the findings of this meta-analysis appear to support establishment of interventions that might diminish pessimism and promote optimism among clinical patients. Various studies49–54 have reported that pessimism can be reduced49,50 and optimism can be enhanced through the use of cognitive behavioral therapy and positive psychological techniques,51–54 making these techniques potentially suitable for use in cardiac rehabilitation programs and other group settings.55
However, further research will need to assess whether optimism that is enhanced or induced through directed prevention or intervention strategies has similar health benefits vs optimism that is naturally occurring. More broadly, the present findings concerning the cardiac benefits of optimism might encourage studies on whether similar benefits can be derived from instilling other positive mindsets (eg, sense of purpose or gratitude) that may be elicited through guided interventions.Limitations
Our meta-analysis has several limitations. The cohorts included in this meta-analysis varied widely in age, ranging from teenagers in 1 study7 to nonagenarians in another.12 However, the consistent association of optimism to reduced cardiovascular risk among all age groups could also be considered a strength of our study. Although each study adjusted for important covariates, these covariates varied widely from study to study.
Thus, we could not systematically assess the independent effects of various individual clinical covariates, including smoking, diabetes, and hypertension. This variability in covariate adjustment may help to account for the considerable heterogeneity found among studies, which was high for the assessment of cardiovascular outcomes (I2 = 87.4%) and moderate for all-cause mortality (I2 = 73.2%).
Lack of uniformity in scales and/or variance in the cut points used within a given scale, particularly the Life Orientation Test–Revised, may have also contributed to this heterogeneity. In addition, the measurement of optimism according to both positively and negatively framed items has led to an ongoing debate as to whether these items separately represent optimism and pessimism as distinct constructs. Although recent research suggests that considering both positively and negatively worded items as indicative of a unitary measure of optimism is most appropriate,56 there was insufficient information to address this issue in our meta-analysis.Conclusions
The findings suggest that optimism is associated with a lower risk of cardiovascular events and all-cause mortality. Future studies should seek to better define the biobehavioral mechanisms underlying this association and evaluate the potential benefit of interventions designed to promote optimism or reduce pessimism.
More information: Sujitha Thavapalachandran et al. Platelet-derived growth factor-AB improves scar mechanics and vascularity after myocardial infarction, Science Translational Medicine (2020). DOI: 10.1126/scitranslmed.aay2140



{kind=link}