









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Artificial intelligence can help cancer patients start their radiation therapy sooner – and thereby decrease the odds of the cancer spreading – by instantly translating complex clinical data into an optimal plan of attack.
Patients typically must wait several days to a week to begin therapy while doctors manually develop treatment plans.
But new research from UT Southwestern shows how enhanced deep-learning models streamlined this process down to a fraction of a second.
“Some of these patients need radiation therapy immediately, but doctors often have to tell them to go home and wait,” says Steve Jiang, Ph.D., who directs UT Southwestern’s Medical Artificial Intelligence and Automation (MAIA) Lab.
“Achieving optimal treatment plans in near real time is important and part of our broader mission to use AI to improve all aspects of cancer care.”
Radiation therapy is a common form of cancer treatment that utilizes high radiation beams to destroy cancer cells and shrink tumors. Previous research shows that delaying this therapy by even a week can increase the chance of some cancers either recurring or spreading by 12-14 percent.
Such statistics motivated Jiang’s team to explore methods of using AI to improve multiple facets of radiation therapy – from the initial dosage plans required before the treatment can begin to the dose recalculations that occur as the plan progresses.
Jiang says developing a sophisticated treatment plan can be a time-consuming and tedious process that involves careful review of the patient’s imaging data and several phases of feedback within the medical team.
A new study from the MAIA Lab on dose prediction, published in Medical Physics, demonstrated AI’s ability to produce optimal treatment plans within five-hundredths of a second after receiving clinical data for patients.
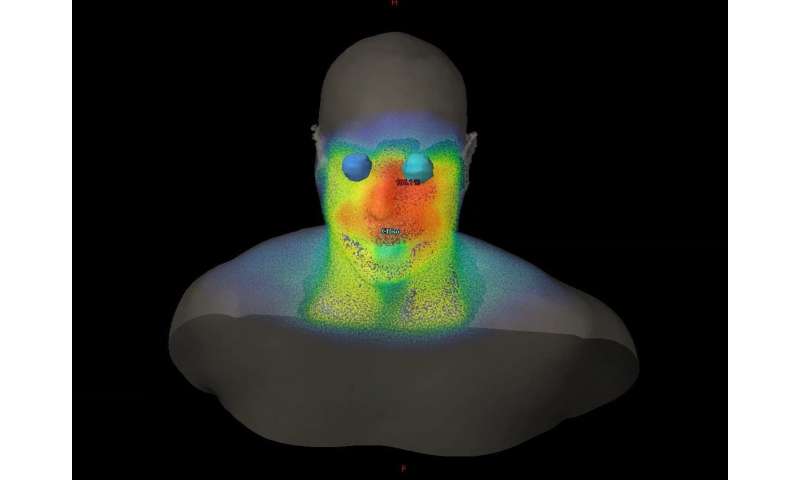
Researchers achieved this by feeding the data for 70 prostate cancer patients into four deep-learning models. Through repetition, the AI learned to develop 3-D renderings of how best to distribute the radiation in each patient.
Each model accurately predicted the treatment plans developed by the medical team.
The study builds upon other MAIA research published in 2019 that focused on developing treatment plans for lung and head and neck cancer.
“Our AI can cut out much of the back and forth that happens between the doctor and the dosage planner,” Jiang says. “This improves the efficiency dramatically.”
A second new study by Jiang, also published in Medical Physics, shows how AI can quickly and accurately recalculate dosages before each radiation session, taking into account how the patient’s anatomy may have changed since the last therapy.
A conventional, accurate recalculation sometimes requires patients to wait 10 minutes or more, in addition to the time needed to conduct anatomy imaging before each session.
Jiang’s researchers developed an AI algorithm that combined two conventional models that had been used for dose calculation: a simple, fast model that lacked accuracy and a complex one that was accurate but required a much longer time, often about a half-hour.
The newly developed AI assessed the differences between the models—based on data from 70 prostate cancer patients—and learned how to utilize both speed and accuracy to generate calculations within one second.
UT Southwestern plans to use the new AI capabilities in clinical care after implementing a patient interface.
Meanwhile, the MAIA Lab is developing deep-learning tools for several other purposes, including enhanced medical imaging and image processing, automated medical procedures, and improved disease diagnosis and treatment outcome prediction.
Artificial intelligence (AI) has recently become one of the most popular words in both industry and academia. Properly known as a modern technology term, AI was perceived as a powerful entity that could “think and act humanly without losing rationality.”1
In computer science fields, AI is defined as the study of algorithms and devices that perceive information from the environment and take action to maximize the chance of achieving specific goals.2
Due to the rapid increases in computational power as well as in data collection and sharing capabilities, a large number of AI techniques, particularly deep learning theories and algorithms, have been published in recent several years.
Following this burst of techniques, AI has permeated nearly every aspect of our lives and is rapidly revolutionizing how we live. In the field of radiation oncology, the AI revolution has also been grounded in the automated support of various parts of the radiotherapy clinical workflow: target and tissue segmentation, treatment planning, radiotherapy delivery, and treatment response assessment.
This article reviews automatic treatment planning (ATP) tools in radiotherapy treatment planning, which have evolved from simple automation execution to the development of AI as a future replacement of current day manual treatment planning process.
Artificial intelligence in radiotherapy treatment planning, particularly deep learning–based investigations, would be the focus of this article. Artificial intelligence applications in other aspects of radiotherapy such as autosegmentation, image processing, or QA can be found in other reviews.3,4
Radiotherapy treatment planning, especially inverse treatment planning, is a laborious process taking hours or even days to complete. Figure 1A shows a brief workflow of manual treatment planning process in the current clinic practice.
A workflow starts with a list of dosimetric requirements, including target coverage and organ-at-risk (OAR) constraints. Based on the specific requirements of each case, a human planner makes decisions about basic planning parameters, including beam energy, number, angles, and so on. While generating a minimally acceptable plan may be quick, improving a plan is much less straightforward and often requires many iterations between planners treatment planning system (TPS).
In addition, physicians may need to interact with human planners back and forth for plan improvement based on intermediate plan results. The iterative nature of these interactions leads to tremendous human efforts and time commitment.

Because of the automatic nature, ATP has successfully reduced plan generation time, especially human interactions (mostly repetitive operations) with TPSs.5,6
Thus, human planners are able to devote more time to explore the optimal dosimetry for individually optimized treatment planning. Furthermore, the improved efficiency could also enable clinical paradigm changes, including novel treatment planning strategies,7 treatment course monitoring methods,8 and treatment delivery workflows.9,10
Besides efficiency, ATP has also improved plan quality consistency and error rate. Because conventional treatment planning is a trial-and-error process exploring dosimetric and clinical trade-offs, the final plan quality is dependent on both planner experience and time available for planning. Many ATP studies across various disease sites have reported a more consistent treatment plan quality compared to manual plans.11–16
As such, ATP can reduce health-care disparities by making advanced treatment planning expertise broadly available.17
Unlike efficiency and consistency, plan quality has not been improved by current ATP techniques.
While studies have reported that machine-generated plans are clinically acceptable, others have indicated that ATP requires essential human tuning or manipulation to ensure acceptable quality and safety.18,19
While humans should remain the center of treatment planning for plan safety and quality, an important goal of AI-based treatment planning algorithms is to augment treatment plan quality. Many new approaches are currently being explored in this area. In the following sections, we will review the past efforts of ATP applications in current research directions, as well as future research topics and challenges.
Novel AI Applications in ATP
Future treatment planning process using a powerful AI agent can be effective and efficient with minimum human intervention. Figure 1E demonstrates the role of AI in future treatment planning workflow. We envision that AI can implement all human operations and reasoning logics based on the comprehensive analysis of patient anatomy.
Parameter such as treatment prescription and delivery technique can be specified as human inputs from physicians, but these parameters can be incorporated into AI decision-making. The future workflow involves minimum human efforts from human planners and physicians; the saved human efforts can be used for other human-centered clinic care tasks.
Currently, a few emerging research topics have been reported focusing on the ATP. While there is also active research ongoing along the directions discussed in the abovementioned section, this section focuses on the novel AI algorithms in ATP, primarily deep learning–based approaches with deep architecture and compositionality.58 In this section, we discuss recent pioneering efforts of novel AI applications in ATP and introduce a few emerging research directions.
Recent Progresses of AI in ATP
A knowledge-based modeling approach was one of the earliest breakthroughs in ATP. Boutilier et al evaluated the clinical applicability of the simultaneous prediction of optimization objective weights for prostate IMRT. Using optimal weights of objectives in previous cases, multinomial logistic regression and weighted K-nearest neighbor algorithms were deployed in the training of weight prediction.59
Results showed that both methodologies could produce good predictions for clinical plans, although no significant performance improvements were found in comparison with the model using logistic regression. Ma et alproposed knowledge-based modeling using support vector regression (SVR).60
In their work, a PTV-only optimization in the absence of OAR considerations was used as the model input in addition to anatomical/geometrical features, and DVH prediction was implemented by SVR as a robust supervised learning technique. In a comparison study, this model was more accurate than the RapidPlan model in bladder and rectum DVH prediction.60
Another major research area in ATP is the prediction of spatial dose distribution. While DVH-based prediction is prevalent, its lack of spatial information may not reveal certain dosimetric end points, such as dose conformity and gradient measurements.
Accurate spatial dose distribution prediction can provide guidance for humans in decision-making during the manual treatment planning process for potentially improved quality and efficiency. In addition, the predicted dose distribution can be used for a fully automated ATP workflow without the need for DVH-based inverse optimization.
Campbell and Miften developed an artificial neural network dose models for spatial dose distribution prediction of pancreatic stereotactic body radiation therapy (SBRT).61 The network was trained by clinical plans with plan parameters voxel-based geometric parameters. Results showed promising accuracy of 3D dose distribution.
Nguyen et al used a modification on the U-net architecture for coplanar prostate IMRT dose distribution prediction.62 Based upon fully convolutional networks, U-net was proposed for image segmentation with transposed convolution operations to maintain original image dimension.63
U-net allows direct image input which avoids the feature extractions (handcrafted feature selections). This could reduce the requirement of data interpretation during the classic modeling process (eg, knowledge-based modeling process). In 2D-based prediction, the average values of absolute dose difference were found to be around 2% in PTV and under 5% of the prescription dose in OARs.62
Similarly, Kearney et al proposed a fully convolutional volumetric dose prediction neural network (DoseNet) for 3D dose distribution prediction of prostate SBRT with possible noncoplanar treatment regimen.64 Compared to U-net, DoseNet was claimed to have reduced network redundancy as a result of the inclusion of residual blocks. Chen et al adopted a published convolutional neural network (CNN) model, ResNet,65 for the dose distribution prediction of nasopharynx cancer in simultaneous integrated boost radiotherapy.66
This prediction model was used to predict a coarse dose map of each patient with reduced intensity content, and a full dose map was recovered from the coarse dose map by a Gaussian regularized low-pass filter. Based on a combined architecture of DenseNet and U-net,67 Barragan-Montero et al incorporated beam angle variation in lung IMRT and developed a model that can predict spatial dose distribution with varying beam arrangement.68
Successful prediction of dosimetric parameters has to be converted to clinical treatment plans. A few studies have explored the feasibility of automatic plan generation that can lead to deliverable plans.
Long et al proposed a framework of threshold-driven optimization for reference-based auto-planning, which automatically generates a treatment plan from a predicted reference DVH set derived from voxel-based dose distribution.69
Mahmood et al proposed a KBP workflow for plan generation.70 For oropharyngeal IMRT plan, 3D dose distribution was predicted, and the actual plan was generated forwardly by using DVH-based optimization and a set of constraints at predetermined dose–volume coordinates.
In a recent study reported by Fan et al,71 3D dose distribution in head and neck cancer was first predicted by a ResNet-based framework. For plan generation, instead of DVH-based inverse optimization, the inverse problem was solved by an L2-norm problem between the predicted dose distribution and the actual dose distribution. An open-source software of fluence map optimization was utilized for this L2-norm problem, and clinically acceptable plans were generated.72
Emerging Research Directions of AI in ATP
The CNN-based algorithms, particularly deep CNN algorithms with large numbers of hidden layers, have been recently extensively studied in medical imaging, making image-based AI applications a dominant topic in ATP research.
Along this research direction, dose distribution prediction to further improve the dose prediction accuracy and efficiency remains the focus. This may lead to a paradigm shift in plan generation: Instead of DVH-based optimization, a plan can be generated as an image reconstruction problem when using predicted dose distribution as the reference data.
Direct prediction of plan parameters could become another potential research area. If certain plan parameters can be converted to 2D/3D space object(s) (“equivalent images”), CNN-based algorithms may be utilized for the prediction, which can lead to automatic plan generation. Potentially, 2D fluence maps of static IMRT beams, 2D aperture series of step-and-shoot delivery, and dynamic multi-leaf collimator sequences (2D + time) of VMAT may be candidates for such predictions.
While most recent AI studies in radiation oncology focused on predictions, few have simulated the reasoning process in treatment planning. In the manual treatment planning process, the decision-making strategy when solving a specific dosimetric trade-off problem varies among different planners; one with more experience may make effective actions more efficiently than another qualified planner with less experience.73 Decision-making strategy will be central to the implementation of ATP with fully automated workflow without human intervention.
In manual treatment planning, each decision regarding dose trade-offs leads to one or more actions in series; this feature is well suited for reinforcement learning, which led to the success of AlphaGo, the famous AI success in the board game Go that had been challenging for conventional computer algorithms.74
Reinforcement learning has 2 distinct features: a trial-and-error search and a delayed reward.75 With a defined reward function, the agent attempts to learn the reward function value in each state and takes actions to maximize the reward. Reinforcement learning can also be realized by a direct policy search, in which the agent attempts to learn the reward functions that directly map observations to actions.
Like the board game Go, radiotherapy treatment planning consists of sequential actions and long-term consequences. However, unlike board game applications in which problems are deterministic, fully observable, single objective with easy reward definition, radiotherapy treatment planning process is (semi-) stochastic, partially observable, and multiobjective with a challenging definition of reward.
These characteristics have to be acknowledged for using reinforcement learning in ATP. For example, an ATP agent can allow only 1 or 2 actions for reinforcement learning (such as DVH constraint weight adjustment or auxiliary planning structure generation via Boolean operations), and the reward has to be defined in a simple way with a numerical scale (eg, target coverage percentage).
In summary, to simulate the human reasoning process, reinforcement learning has to be implemented from a simple problem on a small scale before its extension to the full ATP workflow.
Another possible approach of implementing decision-making process in ATP is using generative adversarial networks (GANs), a class of algorithms that generate representative samples from a set of training data by implementing 2 competing networks in a zero-sum task.76
These 2 competing networks, the generator and the discriminator, are trained simultaneously: While the generator is trained in generating samples, the discriminator is trained to assess whether the samples are “good.”
The GANs have been investigated in natural language processing and computer vision.
Recently, GANs have been utilized in medical image segmentation and disease diagnosis.77,78 The GANs have also been reported for dose distribution for radiotherapy.70 To simulate decision-making for treatment planning, GANs can be used in the model-based reinforcement learning to learn about the environment so that the reinforcement learning agent can take advantage of the previously learned environment (model) instead of simply relying on interaction with the environment (trial-and-error experience).
The 2 trained networks must have a competitive relationship in GANs; such a relationship can be simulated by a plan producer that utilizes the predicted plan distribution and a dose distribution predictor that requires produced treatment plans for its training.
Challenges of AI in ATP
Complexity in Treatment Planning: What Should AI Learn?
Like a self-driving vehicle, the treatment planning process can involve a large number of consequential actions. However, unlike those in a self-driving vehicle or a board game, actions in treatment planning may not have direct consequences (ie, any operation during the plan generation has to be evaluated many steps later after the final dose calculation). Thus, simulation of ATP workflow is more computationally expensive compared to board game applications.
To reduce the simulation cost, the complexity of the decision-making logic has to be settled on a manageable level. Fortunately, researchers can reduce such complexity by enforcing basic rules during ATP.
The current common practice of manual treatment planning follows rules from different aspects, including machine hardware limitation (eg, forbidden zones for noncoplanar beam angle selection due to collision), radiological-based clinical preferences (eg, prioritized duodenum sparing in liver/pancreas SBRT), and institutional practice guidelines (eg, a beam setup template for standardized bilateral neck IMRT).
Integration of these rules by fixing involved variables or enforcing simple “if-else” logic can reduce the ATP workflow complexity. In addition, observations following physical science rules (eg, photon dose requires build-up region with possible coverage reduction of a target near the skin surface) can be integrated into an ATP workflow to further reduce the learning complexity. As a result, building a reasonable ATP workflow for AI training requires a team effort, including radiation physicists, radiation oncologists, radiation dosimetrists, radiation therapists, and other personnel involved in radiotherapy plan generation and verification.
Working With Limited Size Data Sets
Recent progress in deep learning algorithms for imaging applications has been propelled by large-scale data sets. Compared to natural image data sets, medical image data sets have smaller sample sizes for a number of reasons: smaller sample space, patient recruitment, data acquisition variation, lack of infrastructure, and labor-intensive image processing by human experts.4,79
This limitation is compounded for ATP applications, due to the need for specific types of radiotherapy plans, a significant constraint, given the continued advancement and often short histories of modern treatment planning approaches.
So far, most reported ATP studies have included 100 or fewer patients, which is usually acknowledged as a small size data set in the discussion of these studies. Furthermore, the useful data size may get even smaller if confounding variables such as human variations have to be reduced. Relevant studies have reported that dose prediction accuracy could be improved when cases from 2 different radiation oncologists were trained separately.61
In addition, the limited size of data sets is exacerbated by the need for separated training and test data. Ideally, each data set should be separated into 3 subsets: training data, validation data, and test data. Training and validation data are used to train the model, whereas the validation data are used to tune the model during training. Model training can be carried out in a cross-validated fashion.
The test data should be used to test the model performance after model validation; these data should be segregated from the model training. When using the limited size data for ATP, however, the test data set is sometimes not used and the validation results are reported as the study end point. However, it is important to note that for increasingly complex AI methods such as those discussed in section 3, a sufficiently large, well-curated, and controlled database and a rigorous model training and testing process following the 3-part data splitting described earlier are especially critical.
Without them, overfitting, a modeling error where the model performance is overestimated, tends to happen when an overly complex model is developed based on a limited data set. Using data sets of practically limited small sizes for dose prediction in knowledge-based treatment planning, the more complex algorithms were indeed shown to perform inferiorly to the simpler approaches, likely due to overfitting.80
This overfitting limits model generalization when dealing with new data. One potential approach to counteract size limitations is transfer learning, which generates a model by using a small size data set to tune a model which is trained by a larger data set from another domain.81 A commonly used data set for pertaining of deep learning models for medical image studies (particularly CNN) is ImageNet, which is composed of natural scene images.81,82
Data augmentation is another approach for dealing with limited data. In general, data augmentation increases the usable number of data by adding altered versions of the original data.83 A simple example is to add affine image transformations (translations, rotations, and scaling) to the original image sets during the data training for autosegmentation.
A third approach is to incorporate high-level handcrafted features in model learning, which should be treated as representative statistics from small data sets based on previous endeavors. Additional operations can be added into the network topology to avoid overfitting.84
However, this approach requires good knowledge of AI algorithms at a low hierarchy level, which can be challenging for those without a comprehensive computer science background. For ongoing deep learning–based ATP research, it will be interesting to see how the above methods can be adapted and new methods developed to overcome the critical data size limitation.
Toward Clinical Application: Regulation and Collaboration
Although the future of AI in ATP remains in motion, radiotherapy treatment planning will likely not become “driver-less” in the next coming years. The AI-based ATPs must be validated before being introduced into routine clinical use.85 Quality and efficiency improvements should be the focus when evaluating an AI-based ATP method at the current stage. Humans should remain as the center of the treatment planning process in overseeing the clinical treatment planning workflow with ultimate responsibility for plan safety and quality.
Successful validation of AI-based ATP methods requires a large patient cohort size. In addition, for each patient, multiple data types, including multimodality simulation images, treatment plan, radiogenomic tests, and clinical data, may be necessary for methodology development and validation and generalizability.
Such an endeavor may require new paradigms of data regulation and supervision in addition to the standard institutional review board functions. Multicenter collaborations could augment patient cohort size for methodology development and validation. However, retrospective data with significant variations among different institutions’ practice may become a problem when investigating AI-based ATP, particularly in the simulation of reasoning logics.
Prospective multi-institution studies with detailed guidelines of treatment plan generation are fundamental for future studies. Over the past decade, similar efforts on conforming structure naming to the nomenclature standardization by professional society committees, vendors, and the clinical community have made great strides that substantially facilitated radiotherapy big data research.
Therefore, larger numbers of plans from recent clinical trials with rigorous planning guidelines and from the subsequent protocol adoption are expected to yield better quality data for AI-based ATP research. Meanwhile, clinical utilization of the current ATP tools may also help generate plans of more consistent quality among planners and institutions, which could in turn facilitate future AI-based treatment planning research.
Finally, each step in the treatment planning workflow requires great engineering efforts to ensure accuracy and safety. For proof-of-concept studies, open software packages can be adopted when demonstrating the feasibility of new AI applications in ATP.72,86 However, when considering clinical validation, a more robust platform based on the vendor-specific automation function should be used. This may require a new model of academic/industrial cooperation to deal with potential issues in data security and intellectual proprietary conflicts and to ensure the active quality assurance that is critical during the clinical deployment of the new tool.
Conclusion
In this work, the current ATP solutions have been reviewed based on their technical characteristics and clinic workflow impacts. In reported clinical investigations, the discussed solutions have demonstrated the improved planning efficiency and plan quality consistency. Artificial intelligence in ATP is an emerging field and is rapidly developing.
Recent research works of AI in ATP, particularly deep learning–based investigations, have been summarized. In addition, future research directions regarding AI in ATP have been proposed. Finally, challenges of AI research in ATP and practical issues of potential preclinical and clinical investigations have been discussed. We believe that AI technologies would eventually change the paradigm of radiotherapy treatment planning practice. While embracing the promising future, current researchers should be aware of the limitations of current practice and possible research opportunities of AI to meet health-care needs in the next or 2 decades.
More information: Dan Nguyen et al. Incorporating human and learned domain knowledge into training deep neural networks: A differentiable dose‐volume histogram and adversarial inspired framework for generating Pareto optimal dose distributions in radiation therapy, Medical Physics (2019). DOI: 10.1002/mp.13955



{kind=link}