










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



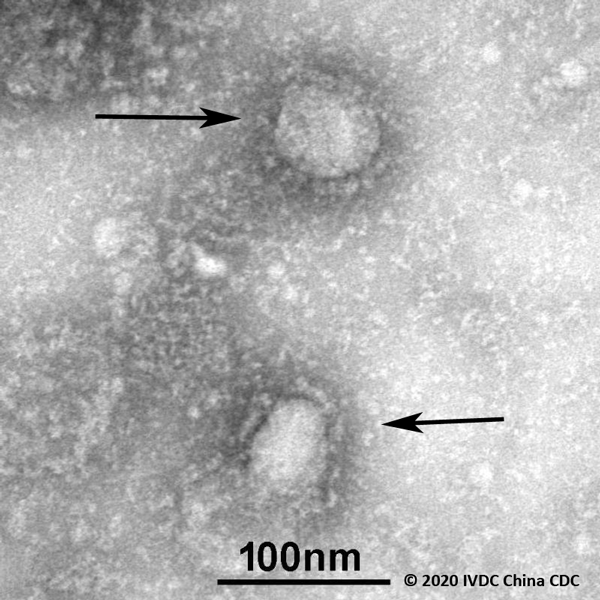
Scientists at the University of Sheffield, in partnership with Sheffield Teaching Hospitals Virology team, have sequenced their first two genomes of the novel coronavirus (COVID-19), with samples collected from patients treated in the UK.
The genomes have been published to the international viral sequence database GISAID to help track the virus and investigate how it is spreading throughout the UK population.
Increasing the amount of sequence data available will provide crucial information to scientists around the world about the origins of coronavirus cases in the UK, revealing how the virus may change over time.
Following the success of the first two samples, the team will now sequence more samples in the coming days.
The University of Sheffield’s Department of Infection, Immunity and Cardiovascular Disease, Florey Institute for Host Pathogen Interactions, and its Sheffield Institute for Translational Neuroscience (SITraN) are working collaboratively to respond to the rapidly evolving outbreak of the virus.
Dr Thushan de Silva, Wellcome Trust Clinical Fellow and Consultant in Infectious Diseases, is leading the work taking place at the University of Sheffield.
He said: “As a virus travels we know it can mutate as it reacts to the genetics of localised populations, creating different strains which may behave in different ways to treatments, vaccines and our body’s immune response.
Generation of sequence data is vital to track this process.
“This data, used alongside published samples from our international partners will be crucial for us to see the trends in these mutations.”
The University is working with Consultant Virologist Dr Caraid Evans, from Sheffield Teaching Hospitals NHS Foundation Trust’s Department of Virology, who is leading the regional NHS virology laboratory’s rapid response to the urgent requirement to support Public Health England in creating national capacity for diagnostic services.
Sequenced in less than 24 hours, the team used the Oxford Nanopore Technologies GridION capabilities under the guidance of Matthew Wyles, a research technician, based at SITraN, by using an Artic Network protocol for real-time sequencing and analysis of viral genomes.
“This data, used alongside published samples from our international partners will be crucial for us to see the trends in these mutations.”
Matthew Parker, a Clinical Bioinformatics Scientist at the National Institute for Health Research (NIHR) Sheffield Biomedical Research Centre and the analyst for the study at SITraN, said: “The facilities and expertise we have here at SITraN mean that we are able to quickly sequence and analyse these samples.
Co-localisation of sequencing equipment and scientists who have expertise in data analysis in the region are key to a successful project like this.
“The capabilities we have developed here at SITraN are crucial for Sheffield to expand our sequencing of the virus and to continue to contribute timely, accessible data that will help in the global management of the current outbreak.”
Currently, 32 countries have contributed to the global effort to tackle the outbreak by uploading samples to a public database GISAID.
Dr de Silva said: “Collecting and sharing standardised global clinical data and samples on patients infected with coronavirus is a critical process in how the health research community can contribute to our understanding outbreaks of new infectious diseases.”
Pathophysiology
CoVs are enveloped, positive-stranded RNA viruses with nucleocapsid. For addressing pathogenetic mechanisms of SARS-CoV-2, its viral structure, and genome must be considerations.
In CoVs, the genomic structure is organized in a +ssRNA of approximately 30 kb in length — the largest known RNA viruses — and with a 5′-cap structure and 3′-poly-A tail. Starting from the viral RNA, the synthesis of polyprotein 1a/1ab (pp1a/pp1ab) in the host is realized.
The transcription works through the replication-transcription complex (RCT) organized in double-membrane vesicles and via the synthesis of subgenomic RNAs (sgRNAs) sequences. Of note, transcription termination occurs at transcription regulatory sequences, located between the so-called open reading frames (ORFs) that work as templates for the production of subgenomic mRNAs.
In the atypical CoV genome, at least six ORFs can be present. Among these, a frameshift between ORF1a and ORF1b guides the production of both pp1a and pp1ab polypeptides that are processed by virally encoded chymotrypsin-like protease (3CLpro) or main protease (Mpro), as well as one or two papain-like proteases for producing 16 non-structural proteins (nsps).
Apart from ORF1a and ORF1b, other ORFs encode for structural proteins, including spike, membrane, envelope, and nucleocapsid proteins.[1] and accessory proteic chains. Different CoVs present special structural and accessory proteins translated by dedicated sgRNAs.
Pathophysiology and virulence mechanisms of CoVs, and therefore also of SARS-CoV-2 have links to the function of the nsps and structural proteins. For instance, research underlined that nsp is able to block the host innate immune response.
[7] Among functions of structural proteins, the envelope has a crucial role in virus pathogenicity as it promotes viral assembly and release. However, many of these features (e.g., those of nsp 2, and 11) have not yet been described.
Among the structural elements of CoVs, there are the spike glycoproteins composed of two subunits (S1 and S2).
Homotrimers of S proteins compose the spikes on the viral surface, guiding the link to host receptors.[8] Of note, in SARS-CoV-2, the S2 subunit — containing a fusion peptide, a transmembrane domain, and cytoplasmic domain — is highly conserved. Thus, it could be a target for antiviral (anti-S2) compounds.
On the contrary, the spike receptor-binding domain presents only a 40% amino acid identity with other SARS-CoVs. Other structural elements on which research must necessarily focus are the ORF3b that has no homology with that of SARS-CoVs and a secreted protein (encoded by ORF8), which is structurally different from those of SARS-CoV.
In international gene banks such as GenBank, researchers have published several Sars-CoV-2 gene sequences. This gene mapping is of fundamental importance allowing researchers to trace the phylogenetic tree of the virus and, above all, the recognition of strains that differ according to the mutations.
According to recent research, a spike mutation, which probably occurred in late November 2019, triggered jumping to humans. In particular, Angeletti et al. compared the Sars-Cov-2 gene sequence with that of Sars-CoV. They analyzed the transmembrane helical segments in the ORF1ab encoded 2 (nsp2) and nsp3 and found that position 723 presents a serine instead of a glycine residue, while the position 1010 is occupied by proline instead of isoleucine.[9] The matter of viral mutations is key for explaining potential disease relapses.
Research will be needed to determine the structural characteristics of SARS-COV-2 that underlie the pathogenetic mechanisms. Compared to SARS, for example, initial clinical data show less extra respiratory involvement, although due to the lack of extensive data, it is not possible to draw definitive clinical information.
History and Physical
The clinical spectrum of COVID-19 varies from asymptomatic or paucisymptomatic forms to clinical conditions characterized by respiratory failure that necessitates mechanical ventilation and support in an intensive care unit (ICU), to multiorgan and systemic manifestations in terms of sepsis, septic shock, and multiple organ dysfunction syndromes (MODS).
In one of the first reports on the disease, Huang et al. illustrated that patients (n. 41) suffered from fever, malaise, dry cough, and dyspnea.
Chest computerized tomography (CT) scans showed pneumonia with abnormal findings in all cases. About a third of those (13, 32%) required ICU care, and there were 6 (15%) fatal cases.[11]
The case studies of Li et al. published in the New England Journal of Medicine (NEJM) on January 29, 2020, encapsulates the first 425 cases recorded in Wuhan.[5] Data indicate that the patients’ median age was 59 years, with a range of 15 to 89 years.
Thus, they reported no clinical cases in children below 15 years of age. There were no significant gender differences (56% male). Clinical and epidemiological data from the Chinese CDC and regarding 72,314 case records (confirmed, suspected, diagnosed, and asymptomatic cases) were shared in the Journal of the American Medical Association (JAMA) (February 24, 2020), providing an important illustration of the epidemiologic curve of the Chinese outbreak.[12]
There were 62% confirmed cases, including 1% of cases that were asymptomatic, but were laboratory-positive (viral nucleic acid test). Furthermore, the overall case-fatality rate (on confirmed cases) was 2.3%.
Of note, the fatal cases were primarily elderly patients, in particular those aged ≥ 80 years (about 15%), and 70 to 79 years (8.0%). Approximately half (49.0%) of the critical patients and affected by preexisting comorbidities such as cardiovascular disease, diabetes, chronic respiratory disease, and oncological diseases, died. While 1% of patients were aged 9 years or younger, no fatal cases occurred in this group.
The authors of the Chinese CDC report divided the clinical manifestations of the disease by there severity:
- Mild disease: non-pneumonia and mild pneumonia; this occurred in 81% of cases.
- Severe disease: dyspnea, respiratory frequency ≥ 30/min, blood oxygen saturation (SpO2) ≤ 93%, PaO2/FiO2 ratio [the ratio between the blood pressure of the oxygen (partial pressure of oxygen, PaO2) and the percentage of oxygen supplied (fraction of inspired oxygen, FiO2)] < 300, and/or lung infiltrates > 50% within 24 to 48 hours; this occurred in 14% of cases.
- Critical disease: respiratory failure, septic shock, and/or multiple organ dysfunction (MOD) or failure (MOF); this occurred in 5% of cases.[12]
Data obtainable from reports and directives provided by health policy agencies, allow dividing the clinical manifestations of the disease according to the severity of the clinical pictures. The COVID-19 may present with mild, moderate, or severe illness.
Among the severe clinical manifestations, there are severe pneumonia, ARDS, sepsis, and septic shock. The clinical course of the disease seems to predict a favorable trend in the majority of patients.
In a percentage still to be defined of cases, after about a week there is a sudden worsening of clinical conditions with rapidly worsening respiratory failure and MOD/MOF. As a reference, the criteria of the severity of respiratory insufficiency and the diagnostic criteria of sepsis and septic shock can be used.[13]
Uncomplicated (mild) Illness
These patients usually present with symptoms of an upper respiratory tract viral infection, including mild fever, cough (dry), sore throat, nasal congestion, malaise, headache, muscle pain, or malaise. Signs and symptoms of a more serious disease, such as dyspnea, are not present. Compared to previous HCoV infections, non-respiratory symptoms such as diarrhea are challenging to find.
Moderate Pneumonia
Respiratory symptoms such as cough and shortness of breath (or tachypnea in children) are present without signs of severe pneumonia.
Severe Pneumonia
Fever is associated with severe dyspnea, respiratory distress, tachypnea (> 30 breaths/min), and hypoxia (SpO2 < 90% on room air). However, the fever symptom must be interpreted carefully as even in severe forms of the disease, it can be moderate or even absent. Cyanosis can occur in children. In this definition, the diagnosis is clinical, and radiologic imaging is used for excluding complications.
Acute Respiratory Distress Syndrome (ARDS)
The diagnosis requires clinical and ventilatory criteria. This syndrome is suggestive of a serious new-onset respiratory failure or for worsening of an already identified respiratory picture. Different forms of ARDS are distinguished based on the degree of hypoxia. The reference parameter is the PaO2/FiO2:
- Mild ARDS: 200 mmHg < PaO2/FiO2 ≤ 300 mmHg. In not-ventilated patients or in those managed through non-invasive ventilation (NIV) by using positive end-expiratorypressure (PEEP) or a continuous positive airway pressure (CPAP) ≥ 5 cmH2O.
- Moderate ARDS: 100 mmHg < PaO2/FiO2 ≤ 200 mmHg.
- Severe ARDS: PaO2/FiO2 ≤ 100 mmHg.
When PaO2 is not available, a ratio SpO2/FiO2 ≤ 315 is suggestive of ARDS.
Chest imaging utilized includes chest radiograph, CT scan, or lung ultrasound demonstrating bilateral opacities (lung infiltrates > 50%), not fully explained by effusions, lobar, or lung collapse.
Although in some cases, the clinical scenario and ventilator data could be suggestive for pulmonary edema, the primary respiratory origin of the edema is proven after the exclusion of cardiac failure or other causes such as fluid overload. Echocardiography can be helpful for this purpose.
Sepsis
According to the International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3), sepsis represents a life-threatening organ dysfunction caused by a dysregulated host response to suspected or proven infection, with organ dysfunction.[14]
The clinical pictures of patients with COVID-19 and with sepsis are particularly serious, characterized by a wide range of signs and symptoms of multiorgan involvement. These signs and symptoms include respiratory manifestations such as severe dyspnea and hypoxemia, renal impairment with reduced urine output, tachycardia, altered mental status, and functional alterations of organs expressed as laboratory data of hyperbilirubinemia, acidosis, high lactate, coagulopathy, and thrombocytopenia.
The reference for the evaluation of multiorgan damage and the related prognostic significance is the Sequential Organ Failure Assessment (SOFA) score, which predicts ICU mortality based on lab results and clinical data.[15] A pediatric version of the score has also received validation.[16]
Septic Shock
In this scenario, which is associated with increased mortality, circulatory, and cellular/metabolic abnormalities such as serum lactate level greater than 2 mmol/L (18 mg/dL) are present. Because patients usually suffer from persisting hypotension despite volume resuscitation, the administration of vasopressors is required to maintain a mean arterial pressure (MAP) ≥ 65 mmHg.
Source:
University of Sheffield



{kind=link}