










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Human stem cells have been regarded as a promising cell source for cardiac regeneration therapy. But their clinical use is hampered due to poor performance after transplantation into failing hearts.
Recently, a stem cell biologist from City University of Hong Kong (CityU), together with his collaborators, has developed a novel strategy called in vivo priming to “train” the stem cells to remain strong after implantation to the damaged heart via a 3-D-printed bandage-like patch.
The positive results of the study show that an in vivo priming strategy can be an effective means to enhance cardiac repair.
Dr. Ban Kiwon, Assistant Professor of CityU’s Department of Biomedical Sciences, collaborated with cardiologist and experts in 3-D printing from South Korea in achieving this breakthrough.
The study was published in the latest issue of Science Advances, titled “In vivo priming of human mesenchymal stem cells with hepatocyte growth factor-engineered mesenchymal stem cells promotes therapeutic potential for cardiac repair.”
Harsh environment in failing hearts hinders stem cell survival
Regeneration is a promising strategy to treat myocardial infarction by injecting human stem cells directly into the failing hearts.
In particular, human mesenchymal stem cells (hMSCs) have been considered as a competitive agent for clinical uses for their proven safety and significant paracrine effects supporting new blood vessel formation and inhibiting cell death.
However, “the clinical trial results are disappointing as the micro-environment of a failing heart is very harsh for the injected hMSCs to stay alive,” said Dr. Ban.
Therefore, researchers have been exploring ways to increase the survival rate of hMSCs in failing hearts. “Priming, or so-called preconditioning, is a common strategy to empower the cells.
The cells are educated through particular stimulations, and when they are relocated to tough environments, they are much stronger against bad conditions and know how to react because of their previous experiences,” explained Dr. Ban.
Conventionally, priming is performed in vitro (outside a living organism) before the cells are transplanted into the heart. “But the effects of priming done in this way usually last for two or three days only.
To extend the duration of the priming effect, I have come up with an idea of in vivo priming, which means the hMSCs are primed directly on the failing hearts,” said Dr. Ban.
Novel strategy: in vivo priming of hMSCs
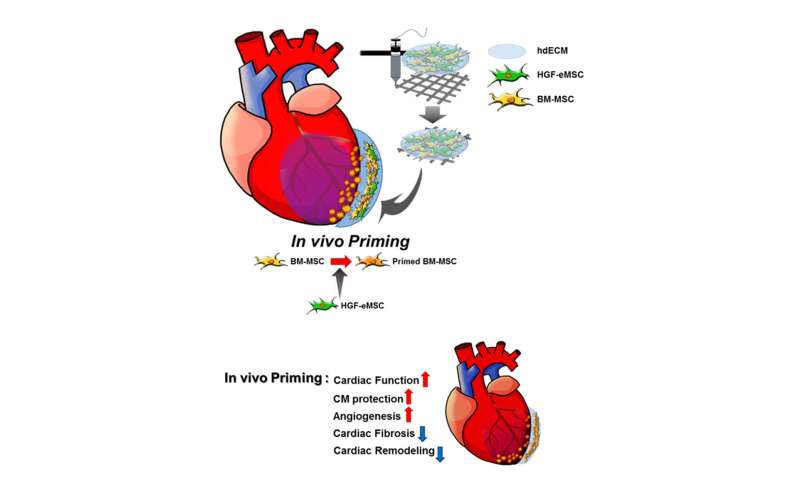
To prove the concept, the research team made a 3-D-printed patch loaded with human bone marrow-derived MSCs, and genetically engineered MSCs with human hepatocyte growth factor protein.
Hepatocyte growth factor (HGF) is involved in multiple biological activities, such as cell survival, blood vessel formation and anti-fibrotic activities, and are important in adult organ regeneration and wound healing.
The patch was then implanted like a bandage on the top of the infarct area of the myocardial-infarction-induced hearts of rats. “The genetically engineered MSCs can continuously secret human HGF protein to prime the hMSCs within the patch and make them stronger,” said Dr. Ban.
Instead of directly injecting the genetically engineered cells into the heart, he added that encapsulating the cells in the patch for placement on the surface of the heart can prevent mutations or other undesirable outcomes.
And the patch is fabricated by 3-D-printing of pig heart-derived extracellular matrix hydrogel, simulating the cardiac tissue-specific micro-environment.
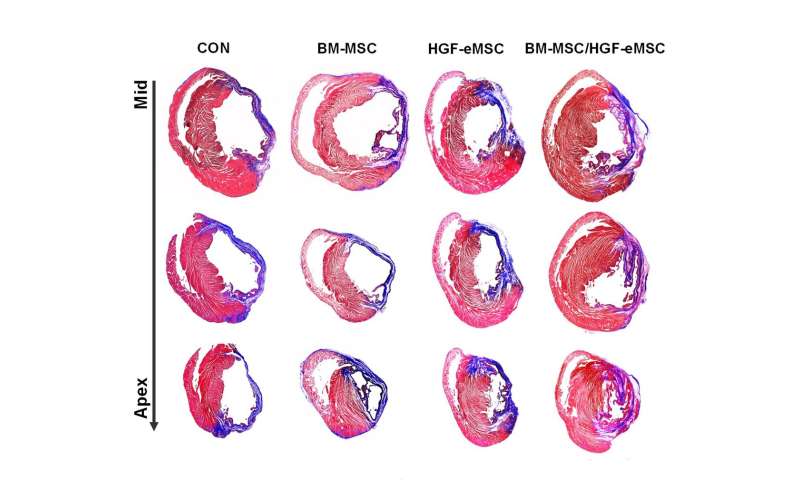
It was found that the primed hMSCs had a higher survival rate compared with unprimed ones in the patches attached to the failing hearts.
Those empowered hMSCs released greater amounts of paracrine factors beneficial for repairing damaged cardiac muscle tissues and regenerating vasculatures.
“We found that the primed cells can survive even after eight weeks in the patch after implantation to the heart.
Also, there is a significant improvement in cardiac function as well as vessel regeneration comparing to the unprimed cells,” said Dr. Ban.
“Our team is the very first to achieve priming in hearts in vivo.
But more importantly, by showing that in vivo priming of hMSCs can enhance the therapeutic potential for cardiac repair, we hope our study can bring significant implications for related stem cell therapy in future,” concluded Dr. Ban. It took the team over two years to achieve these remarkable results.
The team will explore the possibility of conducting the experiments on bigger animals and even clinical trials, as well as modifying the structure of the patch.

Human mesenchymal stem cells (hMSCs) have been considered as one of the most promising cell sources for cell-based cardiac regeneration therapy because of their proven safety and notable paracrine effects to secrete numerous antiapoptotic and angiogenic growth factors, which enabled them to be a more competitive agent for clinical applications (1–3).
However, unlike promising results obtained from preclinical models of myocardial infarction (MI), recent multiple meta-analyses have debated whether the therapeutic potential of hMSC treatment is sufficient (4, 5).
While these clinical trials successfully demonstrated the feasibility and safety of hMSC treatment, the researchers were unable to show significant functional benefit. The overall efficacy of hMSC treatments from multiple meta-analyses has been relatively modest, with an improvement in the left ventricular ejection fraction (LVEF) of approximately 3 to 4% (4, 5).
These results generated a consensus for the need for innovative ways to improve the therapeutic potential of hMSC treatment in failing hearts (3).
In response, diverse approaches have been attempted to enhance the therapeutic efficacy of hMSCs in treating MI. For instance, genetically engineered hMSCs overexpressing a number of antiapoptotic proteins (6, 7), growth factors, or prosurvival genes—such as vascular endothelial growth factor (VEGF) (8), insulin-like growth factor 1 (IGF-1) (9), and hepatocyte growth factor (HGF) (10)—showed increased survival and retention in vivo resulting in improved cardiac function and myocardial angiogenesis in MI-induced hearts.
However, these approaches require genetic modification and, therefore, are incompatible with clinical applications.
Another strategy to bolster the therapeutic potential of hMSCs is priming/preconditioning the hMSCs—which exposes them to physical treatments (e.g., hypoxia and heat shock), pharmacological agents, growth factors, distinct types of biomaterials, modified culture conditions, or other various molecules, including microRNAs—in vitro before transplantation into the hearts (11–15).
Previous studies of the underlying mechanisms of the priming effects reported that hMSCs receiving these priming applications had short-term memory and remembered a priming stimulus, even after relocating to new environments, and shifted their phenotype in therapeutically desirable directions (14, 16).
However, it appears that the priming application only provides a short-term benefit. Although there have been no studies directly evaluating how long the priming/preconditioning effect persists in the heart, the results of previous studies on ischemic preconditioning (IPC), which is one of the major intrinsic cardioprotective processes induced by repeated episodes of short periods of ischemia, imply that the effects of priming/preconditioning in the heart is not likely to last long (17–19).
Several studies examining the underlying mechanisms of IPC suggested that the protective effects conferred by IPC began within minutes after the IPC stimulus and was maintained for only 4 to 6 hours (17–19). Consequently, for hMSCs to be used more effectively for comprehensive cardiac repair, an innovative method that can maintain the priming effect of hMSCs more consistently and effectively must be developed.
Therefore, in the present study, we sought to develop a strategy, namely, in vivo priming, which could prime hMSCs in intact hearts in vivo.
To induce and maintain the beneficial effects of priming persistently in situ, we loaded MSCs isolated from human bone marrow (BM-MSCs) together with genetically engineered HGF-MSCs (HGF-eMSCs) that continuously secrete HGF within a three-dimensional (3D) cardiac patch, which was implanted in the epicardium of MI-induced hearts. Regarding patch generation, to recapitulate the cardiac tissue–specific microenvironment as closely as possible, we used heart-derived extracellular matrix (hdECM) hydrogel.
Our hypothesis was that BM-MSCs can be constantly primed by HGF secreted from HGF-eMSCs within the cardiac patches and those empowered BM-MSCs would demonstrate an enhanced therapeutic potential for cardiac repair. Subsequently, we demonstrated that the primed BM-MSCs had a higher survival rate compared with unprimed BM-MSCs in the patches while they were attached to the MI hearts, which led to a significant improvement in cardiac function and an enhancement of vessel formation after MI. The results of this study carry significant implications for future stem cell therapy in cardiac repair.
DISCUSSION
Despite varied outcomes from several clinical trials evaluating the therapeutic efficacy of MSCs in treating heart failure, because of several inherent advantages, MSCs are still considered one of the most promising candidates for cell-based cardiac regeneration therapies to date (3).
Thus, particularly in the field of adult stem cells, the focus has been on developing effective methods to augment the therapeutic potential of MSCs (14). In the present study, we sought to develop a strategy to enhance the therapeutic efficacy of MSCs in vivo by coencapsulating BM-MSCs with engineered HGF-eMSCs within 3D cardiac patches, which were then implanted in the epicardium of MI hearts.
Our results demonstrated that the BM-MSCs were primed within the epicardially attached cardiac patch through the sustained secretion of paracrine factors, specifically HGF, from the HGF-MSCs.
Subsequently, those empowered BM-MSCs survived for longer periods and released greater amounts of beneficial paracrine factors capable of salvaging damaged myocardium and regenerating vasculatures.
Although the concept of priming cells to bolster therapeutic capacity is not entirely novel and it has been previously tested in various other cell types, such as several types of immune cells (3, 13) and hepatocytes (20), the fact that this study was the very first to achieve priming in intact hearts in vivo after transplantation of BM-MSCs onto MI hearts should be appreciated.
To prime BM-MSCs in vivo, we encapsulated BM-MSCs together with HGF-eMSCs genetically engineered to continuously release HGF. We chose HGF as a major inducer for in vivo priming since HGF is a renowned pleiotropic factor that is involved in multiple biological activities, such as cell proliferation and survival, angiogenesis, and antifibrotic and antiapoptotic activities (21–24).
Previous studies showed that overexpression of the HGF gene in the myocardium or the transplantation of HGF-overexpressing MSCs promoted cardiac function and vascular regeneration and prevented cellular apoptosis. MSCs pretreated with HGF cytokines displayed greatly enhanced therapeutic potential to repair damaged organs, such as livers (20).
In regard to the use of genetically engineered HGF-eMSCs generated by lentiviral vector encoding human telomerase reverse transcriptase (hTERT) and c-Myc reprogramming factors, to exclude the risk for tumorigenicity, particularly since c-Myc is an oncogene, we irradiated (100 Gy) the cultured HGF-eMSCs before patch generation to prevent their overgrowth.
Subsequently, we observed that the proliferation rate of HGF-eMSCs was markedly decreased in in vitro culture, and no tumor was detected from in vivo tumorigenicity testing using nude mice. Notably, microscopic observations of rat heart tissues harvested at weeks 4 and 8 after implantation revealed that most of the hMSCs were located within the patch and they did not migrate to the neighboring myocardium until 8 weeks following implantation.
Most of DiI (1.1′-dioctadecyl-3,3,3′,3′-tetramethylindocarbocyanine perchlorate)–positive hMSCs, which we prelabeled with CM-DiI (red fluorescence) before patch generation to monitor their migration, were detected within the patch, not in the myocardium.
These results further verify that our strategy of encapsulating genetically engineered cells in patches located outside the heart is a suitable strategy that can prevent undesirable outcomes from genetically modified cells in the heart.
One of the critical hurdles for the clinical application of BM-MSCs for cardiac cell therapy is their low survival and poor engraftment in the heart. Given the inherent characteristics of the heart as a contractile organ and owing to the undesirable microenvironments in the ischemic myocardium, the implanted BM-MSCs easily die or leak out of the injection sites and washout through venous shunts.
Therefore, to improve the survival of transplanted BM-MSCs and thereby ensure prolonged secretion of favorable paracrine factors toward injured myocardium, we aimed to generate hdECM-derived cardiac patches to serve as carriers of a cell reservoir, as well as to provide structural and potential vasculature support to the infarcted area.
Our results indicated that both primed and unprimed BM-MSCs appeared to survive better within the patch until 8 weeks after implantation, as evidenced by the minimal number of detectable TUNEL-positive MSCs in most of the experimental groups. We presume that the hdECM-derived cardiac patches provided a complimentary microenvironment that enabled more resistance against hostile conditions in ischemic tissues, particularly during the early stage of implantation.
Surviving MSCs continuously released beneficial paracrine factors and, consequently, restored the injured myocardium and promoted the vascular regeneration. In terms of the techniques we used to engineer the cardiac patches, in direct contrast to several previous studies that simply used natural ECMs or synthetic materials to produce cardiac patches, we took an innovative approach that used a mixture of lyophilized porcine hdECM with MSCs as bioink. By using lyophilized porcine hdECMs that allow for convenient storage and easy transport of cell-free ECMs, our study demonstrated the potential clinical benefit of BM-MSCs in translational research in the field of cardiac repair.
In summary, in the current study, we suggested a proof-of-concept platform coined as in vivo priming that maximizes the therapeutic potential of BM-MSCs to treat heart disease. When BM-MSCs were placed together with HGF-eMSCs engineered to continuously secrete HGF in a cardiac patch that was epicardially implanted in the hearts, paracrine secretion by the BM-MSCs was remarkably bolstered and the paracrine factors were stably secreted toward the diseased hearts.
Despite literature movement away from BM-MSCs, our study indicates the remarkable potential that BM-MSCs still have as a source of cell-based cardiac therapy if used effectively—a potential that, if studied under scrutiny, can open a new doorway to the future of cardiac stem cell therapy.
More information: “In vivo priming of human mesenchymal stem cells with hepatocyte growth factor–engineered mesenchymal stem cells promotes therapeutic potential for cardiac repair” Science Advances (2020). DOI: 10.1126/sciadv.aay6994 , https://advances.sciencemag.org/content/6/13/eaay6994



{kind=link}