")










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The global community has massively underestimated the risks that pandemics present to human life and livelihoods, at least in terms of policy outcomes.
The resources devoted to preventing and responding to such threats seem wholly inadequate to the scale of the risk.
While it is impossible to produce precise estimates for the probability and potential impact of pandemics, it is not difficult to demonstrate a compelling case for greater investment.
There are very few risks facing humankind that threaten loss of life on the scale of pandemics.
People living in eras when microbes were not considered to be the cause of epidemic diseases responded to these threats differently from people living in eras when the role of microbes was understood.
Well into the nineteenth century, for example, experts and lay people alike believed that many epidemics and contagious diseases were spread through polluted air – or miasma, from the Greek word for defilement of the air or pollution.
The miasmatic theory of disease held that toxic emanations emerged from the soil or from rotting organic material or waste products and caused specific epidemic diseases such as cholera, typhus, and malaria.
Given the foul odor that pervaded every urban center of this era, the belief that it was an unhealthy force makes a good deal of sense, but when this theory was in vogue it led to public-health approaches that were very different from those taken today.
Aside from calls for quarantine, most attempts to manage an epidemic centered on cleaning up and disinfecting streets, sewers, privies, and other dirty parts of the urban environment.
This trend changed markedly in the mid-to-late nineteenth century with the advent of the germ theory of disease, and it continues to be revised, refined, and fine-tuned today as we learn more and more about microbial ecology, evolution and genomics.
Still, old ideas about contagion are often slow to die and, like fevers of unknown origin, have the power to recrudesce; as a result, many people today have ideas about the cause and spread of particular infectious diseases that are markedly different than the principles we teach in the medical school classroom (Duffy, 1992).
A pandemic could kill as many people as a devastating war, yet the resources committed to pandemic prevention and response are a fraction of the resources we commit to security.
There are also very few risks that have greater potential for catastrophic economic impact – potentially on the scale of a global financial crisis – but the measures we are taking to avoid another financial crisis are of an entirely different magnitude.1
The costs of significantly upgrading the world’s defenses against pandemics, while substantial, are not out of reach.
The economic devastation typically associated with epidemics can have a strong influence on the public’s response to a contagious disease crisis.
An order of quarantine, which closes a port or a city to foreign travelers or goods, costs communities a great deal of money and creates great hardships for individuals.
It is not surprising, then, that during the international sanitary conferences of the mid-nineteenth century, merchants were often vocal opponents of any efforts to prevent or contain disease that might have had the effect of impeding commercial enterprises and the flow of capital.
Such concerns are particularly salient in today’s world, given the existence of a globalized marketplace in which a rapidly growing percentage of the world’s population does business, especially since the emergence of India, China, and the former Communist bloc nations.
There are two sides to this equation however. While increased global commerce can certainly contribute to the spread of a pandemic, it also sets up conditions that encourage more effective responses to a pandemic.
Epidemics cost the business community a lot of money, and, in particular, the cost of a human-to-human avian influenza pandemic would be, according to all reliable projections, simply staggering.
The threat of such losses could therefore encourage developing nations faced with a brewing epidemic to communicate more openly with Western nations in the hope that their greater financial resources could help them rapidly contain or mitigate the outbreak (Stern and Markel, 2004).
The movements of people and goods and the speed of travel are major factors in the spread of pandemic disease.
Prominent outbreaks, epidemics, and pandemics of the last century.
| Year(s) | Pathogen | Geographic location | Cases/mortality | Other notes | References |
|---|---|---|---|---|---|
| 1918–1920 | Influenza (Spanish flu) | Worldwide | 500 million cases and 30 to 100 million deaths | The Spanish flu claimed the lives of 2–5% of world’s population, far exceeding the death toll of WWI. | (1, 2, 6) |
| 1957–1958 | Influenza (Asian flu) | Worldwide | 1 to 2 million deaths | Accelerated development of a vaccine limited the spread of the responsible influenza strain. | (7) |
| 1968–1969 | Influenza (Hong Kong flu) | Worldwide | 500,000 to 2 million deaths | The Hong Kong flu was the first virus to spread extensively due to air travel. | (7) |
| 1960-present | HIV/AIDS | Worldwide, primarily Africa | 70 million cases and 35 million deaths | HIV was first identified in 1983. The earliest known case came from a blood sample collected in 1959. | (8–10) |
| 1961-present | Cholera | Worldwide | 1.4 to 4 million annual cases and 21,000 to 143,000 annual deaths | The seventh cholera pandemic began in South Asia in 1961. Recent notable outbreaks include those in Zimbabwe from 2008 to 2009, Haiti from 2010-present, and Yemen from 2016-present. | (11, 12) |
| 1974 | Smallpox | India | 130,000 cases and 26,000 deaths | One of the worst smallpox epidemics of the twentieth century occurred just 3 years before the disease was eradicated. | (13) |
| 1994 | Plague | India | 693 suspected cases and 56 deaths | The outbreak originated in Surat, India. Within days, hundreds of thousands of the city’s 1.6 million residents fled, spreading the disease across five states. | (14, 15) |
| 2002–2003 | SARS | Originated in China, spread to 37 countries | 8,098 cases and 774 deaths | International business travel allowed the SARS virus to spread quickly across continents. | (16, 17) |
| 2009 | Influenza (Swine flu) | Worldwide | 284,000 deaths | Many public and private facilities in Mexico closed in an attempt to prevent the spread of “swine flu” during the early days of the epidemic. The pork industry also suffered losses, even though eating pork products posed no risk. | (18–20) |
| 2014–2016 | Ebola | West Africa, primarily Guinea, Liberia, and Sierra Leone | 28,600 cases and 11,325 deaths reported (likely underestimates) | 300,000 doses of an experimental Ebola vaccine were subsequently stockpiled. | (21, 22) |
| 2015-present | Zika | The Americas, primarily Brazil | Unknown number of cases and 0 deaths reported | The Zika epidemic has resulted in few, if any, deaths. However, birth defects resulting from infection in pregnant women occurred frequently, which prompted some governments to encourage delaying pregnancy for as long as 2 years. | (23) |
| 2016 | Dengue | Worldwide | 100 million cases and 38,000 deaths | Dengue outbreaks occur periodically in affected regions. 2016 was notable for the unusual scale of outbreaks across the globe. | (24) |
| 2017 | Plague | Madagascar | 2,417 cases and 209 deaths | Plague is endemic in Madagascar, but an increase in pneumonic plague, which can be transmitted from human to human, was associated with the recent spike in cases. | (25) |
It is no coincidence that the rise of bubonic plague pandemics during the Middle Ages (as well as the invention of the formal concept of quarantine) coincided with the advent of ocean travel and imperial conquest.
As humans traveled in wider and wider circles, so too did the germs that inhabited them. During the nineteenth century, four devastating cholera pandemics were aided and abetted by the transoceanic steamship travel of millions of people.
By the close of the 19th century, journeys from Europe or Asia to North America required a travel time of 7 to 21 days, which gave most infectious diseases ample incubation periods and facilitated their recognition by health officers at the point of debarkation.
It is quite different today, when the main mode of international travel, commercial jet planes, allow people to travel anywhere in the world in less than a day. Indeed, a recent study in PLoS Medicine details how seasonal influenza can mirror peaks and valleys in air travel (Brownstein et al., 2006).
Yet while the natural response to a pandemic might be to limit air travel, either by an international edict or by the natural response of people to avoid travel by commercial airliner during such a crisis, such a response would pose a new set of troubling and potentially damaging consequences.
Our fascination with the suddenly appearing microbe that kills relatively few in spectacular fashion too often trumps our approach to infectious scourges that patiently kill millions every year.
In 2003, for example, society’s response to SARS – which affected approximately 8,000 people and killed 800 – was much more dramatic than its response to tuberculosis, which infected 8,000,000 and killed 3,000,000 that same year.
In 2001 there was a similar disproportion in the response to anthrax, which threatened only a few, and to the ongoing global pandemic of HIV/AIDS, which kills 2,000,000 people a year. A
n even more egregious example is the lack of widespread attention to the common scourges of lower respiratory tract infections and diarrheal diseases, which kill millions on an annual basis (Markel and Doyle, 2003; Achenbach, 2005).
Unfortunately, it will be impossible to know until long after the money and resources have been committed – and perhaps only after a flu pandemic has actually occurred – whether influenza was the right microbe to focus upon instead of one of the host of other emerging and re-emerging infectious threats that we face.
Perhaps the more salient question for our discussion today is how we can apply the lessons of SARS, influenza, AIDS, bioterrorism, and other microbial threats to develop a comprehensive and global plan against contagion.
Issues Between Governments: Infectious Disease and Commerce
Humans have long transmitted diseases over great distances. As shown in Figure 1-1, historians have traced the paths of three ancient diseases that, over the course of decades, spread across several continents. Some of these diseases are thought to have originated in Africa, others in Asia.

Today, infections emerge, reemerge, and spread around the world with such frequency that it is difficult to keep a list of them up to date.
In 2000, for example, athletes participating in an international triathlon held in Malaysia contracted leptospirosis and returned to their home countries during the incubation period.
While this disease is not transmitted from person to person, its presence in the athletes did create a diagnostic challenge for health-care workers around the world. More to the point, the case illustrates the potential for transmission in a world where international travel is both rapid and common.
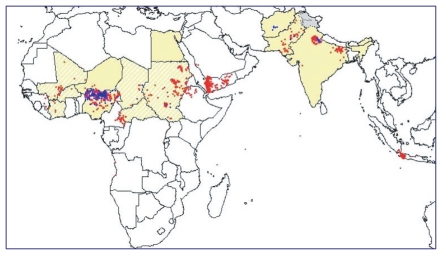
Figure 1-2 illustrates how polio spread from northern Nigeria after immunization activities were halted there in 2003. Wild type 1 poliovirus, endemic in that area, spread rapidly to neighboring countries, and thereafter – through Saudi Arabia and Yemen – as far away as Indonesia.
By the fourteenth century, governments had clearly recognized the capacity for the international spread of disease and had legislated preventive measures, such as the establishment of quarantine in Venice.
In order to keep plague out, ships arriving in that city-state were not permitted to dock for 40 days. Table 1-1 briefly traces the history of surveillance and response to global disease from this quarantine to the 1969 adoption of the International Health Regulations (IHR).[Blackford MG. A History of Small Business in America. Chapel Hill: University of North Carolina Press; 2003.]
WHO developed these regulations, along with guides for ship sanitation and for hygiene and sanitation in aviation, as a way of minimizing the international spread of disease while interfering as little as possible in world trade, transportation, and travel.
TABLE 1-1From Quarantine to International Health Regulations: A Framework for Global Health Surveillance and Response
| 1374 | Venice | Quarantine for Plague |
| 1851 | Paris | First International Sanitary Conference |
| 1947 | Geneva | WHO Epidemiological Information Service |
| 1951 | Geneva | International Sanitary Regulations |
| 1969 | Geneva | International Health Regulations |
The IHR requires that WHO be notified whenever cholera, plague, or yellow fever occur, but given today’s vast number of global microbial threats, the regulations are clearly outdated.
The IHR also provides guidance to ports, airports, and frontier posts about preventing the entry of infected travelers as well as preventing the proliferation or entry of disease vectors, such as mosquitoes and rats.
The regulations specify the maximum precautionary measures that countries may adopt in order to protect themselves from the three reportable diseases as well as the measures that they should undertake to deal with infectious diseases in general.
Reports of cholera, plague, or yellow fever received by WHO are published in the Weekly Epidemiological Record.
In 2005, a substantial revision and modernization of the IHR was adopted. The revision addresses a long-standing problem: that countries often do not report the presence of infectious diseases within their borders because they fear the economic consequences of doing so.
Trade sanctions resulting from infectious disease are often more severe than necessary, as happened, for example, following the discovery that people had contracted variant Creutzfeldt-Jakob disease by eating beef from cattle in the United Kingdom (UK).
These cattle had been infected with prions that caused bovine spongiform encephalopathy (BSE). Many countries reacted by banning imports from the UK, even after the UK had taken measures that probably rendered its products more secure from BSE than those of many of these same countries.
The result was that the UK lost billions of dollars in trade.
The lesson, then, is that the international spread of disease – or the threat of its spread – reduces commerce with affected areas.
Governments must, therefore, attempt to balance two competing goals: to prevent infectious disease from crossing their borders while simultaneously minimizing the economic impacts of disease-related restrictions on travel and trade.
The recent Ebola outbreak revealed many gaps and shortcomings in preparedness and the ability to respond effectively at both the national and global levels. These flaws in our defenses cost thousands of lives and meant that the ultimate cost of preventing Ebola from becoming a pandemic was much higher than it may otherwise have been.
Ebola also demonstrated that being better prepared has huge benefits.
For example, Nigeria contained the virus successfully, despite being a densely populated nation with many health and social challenges.
The Commission believes that commitment of an incremental $4.5 billion2 per year would make the world much safer.
This figure includes expenditures for strengthening national public health systems; funding research and development; and financing global coordination and contingency efforts, all of which are explored in greater detail in subsequent chapters.
While it may be beneficial to spend more, investing at least this much would address the most urgent weaknesses in global health security. In addition to shoring up our defenses against pandemics, this investment would also yield enormous benefits in protecting the world against other health risks, such as antimicrobial resistance (AMR) and bioterrorism.
How does $4.5 billion per year stack up against the potential risks?
The 1918 influenza pandemic killed approximately 50 million people (CDC, 2014) and arguably as high as 100 million in 1918–1920 (Johnson and Mueller, 2002).
As a driver of incremental mortality in the last century, few other events even compare:
- Total deaths from World War II are estimated to be between 35 and 60 million,3 and
- HIV/AIDS has killed nearly 40 million people since the start of the epidemic (UNAIDS, 2014).
Moreover, despite enormous advances in medicine and scientific understanding, and the containment of recent pandemic threats such as severe actue respiratory syndrome (SARS), H1N1 influenza, and, eventually, Ebola, we should not be complacent about future risks.
The consensus among leading epidemiologists and public health experts is the threat from infectious diseases is growing. Emerging infectious disease events are increasing significantly over time (Jones, 2008), and, with an ever-increasing global population, greater consumption of meat, and continuing increases in mobility and connectivity, the conditions for infectious disease emergence and contagion are more dangerous than ever. $4.5 billion annually equates to just 65 cents per person; with such a modest investment, we could better protect everyone in the world from such risks.
From an economic perspective, the argument is equally compelling.
The World Bank has estimated the economic impact of a severe pandemic (that is, one on the scale of the influenza pandemic of 1918–1919) at nearly 5 percent of global gross domestic product (GDP), or roughly $3 trillion (Jonas, 2014).
Some might see this as an exaggeration, but it could also be an underestimate. Aggregate cumulative GDP losses for Guinea, Liberia, and Sierra Leone in 2014 and 2015 are estimated to amount to more than 10 percent (UNDG, 2015; World Bank, 2014).
This huge cost is the result of an epidemic that, for all its horror, infected only about 0.25 percent of the population of Liberia, roughly 0.25 percent of the population of Sierra Leone, and less than 0.05 percent of the population of Guinea (WHO, 2016), with approximately 11,300 total deaths (CDC, 2016).
The Commission’s own scenario modeling, based on the World Bank parameters, suggests that during the 21st century global pandemics could cost in excess of $6 trillion, with an expected loss of more than $60 billion per year (see Appendix C).4
Indeed, the economic impact of infectious diseases appears to be increasing as greater human and economic connectedness – whether through transnational supply chains, increased travel, or ubiquitous access to communication technologies and media – fuel contagion, both of the virus itself and of fear.
Most of the economic impact of pandemics stems not from mortality but from behavioral change, as people seek to avoid infection (Burns et al., 2008). This behavioral change is driven by fear, which in turn is driven by a potent mix of awareness and ignorance.
As Poincaré noted with respect to the plague, “the plague was nothing; fear of the plague was much more formidable” (Poincaré, 1905).
The experience of SARS is instructive: viewed from the perspective of overall mortality, SARS infected “only” 8,000 people and killed less than 800 (WHO, 2003).
Yet the economic cost of SARS has been estimated at more than $40 billion (Lee and McKibbin, 2004).
At the peak of SARS, Hong Kong saw an 80 percent reduction in air traffic (Lee and McKibbin, 2004) and a 50 percent reduction in retail sales (Siu and Wong, 2004).
One reason that pandemics are so hard to predict, and their costs so hard to estimate, is that they are not discrete events, but represent the extreme end of a spectrum of infectious disease risks (see Figure 2-1).
New infectious diseases emerge annually. Outbreaks, both of new infectious diseases and of known pathogens, occur many times every year.
A small proportion of such outbreaks evolves into epidemics; others are contained, eradicated, or become endemic. An even smaller proportion of epidemics turns into pandemics.
Therefore, pandemic risk should not be seen in isolation, but rather as part of a spectrum of escalating disease events, with both costs and potential for mitigation across the entire spectrum.

Spectrum of disease risk. SOURCE: Figure created for the GHRF Commission by El Turabi and Saynisch, Harvard University.
Viewed from this perspective, the task for policy makers is not just to reduce the likelihood and cost of pandemics as extreme right-tail events, but to reduce the economic and human costs across the whole spectrum of infectious disease threats.
We should not become fixated on the probability of a “once-in-a-100-years” pandemic of the 1918–1919 influenza pandemic of severity.
Much less virulent pandemics can still cause significant loss of life and economic impact. The influenza pandemics of 1958 and 1968, while far less deadly than the one in 1918–1919, are estimated to have cost 3.1 percent and 0.7 percent of global GDP, respectively (McKibbin and Sidorenko, 2006).
Potential pandemics, that is outbreaks or epidemics that could become pandemics if not effectively contained, can also have enormous impact.
Ebola, an epidemic that looked as if might have the potential to become a pandemic, has killed more than 11,000 people (CDC, 2016) and cost more than $2 billion (World Bank, 2014).
While there is a high degree of uncertainty, the Commission’s own modeling suggests that we are more likely than not to see at least one pandemic over the next 100 years, and there is at least a 20 percent chance of seeing four or more (see Appendix C).
Framed in this way, the investment case for pandemic preparedness and response rests not just on the probability and costs attached to a severe pandemic, but also on the likely costs to human lives and livelihoods across the spectrum of infectious disease threats.
The apparent acceleration in the emergence of new infectious diseases underscores the need for a “One Health” approach, which recognizes the connection of human health to animal and plant health.
Further outbreaks of new, dormant, or even well-known diseases are a certainty. More epidemics with the potential to become pandemics should be anticipated.
Among the known threats are multiple strains of influenza, coronaviruses, and vector-borne diseases – headlined by malaria but also including other endemic conditions that are still spreading because of climate change among other reasons.
There is also always the possibility of re-emerging or completely new zoonotic viruses, or of different kinds of infectious threats, such as fungal infections, particularly in the context of growing AMR.
Such potential pandemics are perhaps more frequent than is recognized; in the past 15 years, we have faced at least five: SARS, H5N1, H1N1, Ebola, and Middle East respiratory syndrome (MERS).
So, even if we downplay the likelihood of a catastrophic pandemic – and this would certainly be a mistake – there is a powerful case for investing more to minimize the frequency and mitigate the impact of potential pandemics.
We appear to have been successful in preventing Ebola from becoming a pandemic, but at far greater cost in terms of lives and dollars than would have been necessary had we been better prepared.
Given the degree of uncertainty in this arena, it also makes sense to think about the relative costs of error – of investing too much or investing too little.
If we overinvest, we will have upgraded primary health care and public health systems more than merited by the pandemic threat alone and spent more on vaccine and diagnostic research than strictly necessary.
Yet it is hard to see this as wasted money. The core capabilities of primary care and public health systems are crucial to achieving many other health objectives.
For example, reinforcing disease surveillance and response capabilities will have benefits for the management and treatment of endemic diseases, such as tuberculosis and malaria, which themselves cause significant loss of life and economic harm.
- Tuberculosis affects 8.5 million globally each year, reducing labor productivity by about 30 percent and reducing global GDP by about $12 billion per year (Fonkwo, 2008).
- Malaria affects approximately 150 million people each year (Global Burden of Disease Study 2013 Collaborators, 2015), and is estimated to reduce GDP for sub-Saharan African countries by some 10 percent (Sachs and Malaney, 2002).
Such investments in the foundations of national health systems would also play a role in mitigating the threats to health security from noncommunicable diseases (Heymann et al., 2015).
On the other hand, if we invest too little, we open the door to potential disaster.
The investment case for reinforcing global capabilities, rather than simply each country’s own preparedness, does not depend on altruism, although such a moral argument clearly exists.
To make themselves safer, rich countries must help the poorer parts of the world, because global health security is truly a public good.
Zoonotic transfers and outbreaks in even the poorest parts of the world can have global impact, as both HIV/AIDS and Ebola demonstrate.
It is instructive to take pandemics out of the medical context and think about the threat as a national security issue. For any one country, a pandemic is a threat that could kill hundreds and thousands every few years – and might potentially kill millions.
Yet in most countries it attracts a small fraction of the resources devoted to national defense.
Global military spending amounts to more than $2 trillion (CIA, 2015); many countries participate in highly structured and well-resourced international alliances, such as the North Atlantic Treaty Organization (NATO); and most countries regularly conduct exercises to test preparedness and response.
As Bill Gates has pointed out, the contrast with the small amount of resources devoted to protecting humankind from potential pandemics is striking (Gates, 2015).
It is equally illuminating to consider pandemics as an economic risk.
Despite the compelling evidence of the disruption caused by potential pandemics, their threat to economic stability typically receives very little attention from economic policy makers at either the national or international levels, and even fewer resources.
Since the global financial crisis of 2008, policy makers have forced banks to dramatically increase their capital levels as a protection against future crisis, the cost of which is ultimately borne by society as a whole, through lower returns on equity or higher costs of credit.
Consider the new total loss absorbing capacity (TLAC) rule, which applies only to the 27 largest banks in the world.
The direct costs of this rule are estimated at $17 billion, and the resulting higher credit spreads are expected to cost approximately $20 billion in reduced GDP growth.
This single component of the investment in preventing a future financial crisis dwarfs our Commission’s proposed spending on pandemic risk (BIS, 2015).
Our point is not to argue that we spend too much or too little on other threats to security or economic stability, but rather to highlight out how relatively little we invest to protect the world from the threat of infectious diseases.
One truth that holds across many different types of potentially catastrophic risks, including pandemics, is that prevention is far more cost-effective than response, and that the most effective response is a well-prepared response.
In other words, spending money now will save money and lives later.
Suggestions/Recommendations. Based on our assessment of the challenges for R&D identified in this paper, we propose the following potential solutions for the GPMB and others to consider:
- Rationalise the system for coordinating R&D activities to create more focused global leadership with respect to epidemics R&D, reduce fragmentation, recognise overlaps and accelerating innovation. As part of this, WHO’s role needs to be further strengthened and resourced to provide leadership across preparedness and response.
- Develop norms, ethics, and standards of behaviour for all actors including national governments, humanitarian organisations, international organisations, militaries, researchers, and communities.
- Develop multi-year plans for R&D that move beyond disease specific approaches, to avoid cycles of panic and neglect.
- These plans should reflect a sustained commitment to R&D beyond immediate emergencies and complement national research agendas and centres of research excellence, National Action Plans for Health Security and regional activities.
- Efforts to strengthen in-country R&D capacity should be more epidemic sensitive than epidemic specific, addressing day-to-day issues and not focused on building capabilities that are only relevant in the event of an epidemic.
- As long-term plans are developed, international and national research funders should align their spending on R&D for epidemics to these, such as R&D Blueprint roadmaps, country-led research agendas for epidemic risk diseases and National Action Plans for Health Security (NAPHS).
- Plans for R&D should address the following gaps:
- Systematic integration of social science into response programme activities, and further training and collaboration opportunities for social scientists to work with response actors across the entire preparedness/response continuum. WHO and implementing agencies, such as UNICEF, need to build on existing efforts and further integrate social sciences into their programmes so that evidence shapes practice.
- Accelerate development of rapid diagnostics and therapeutics. Building the foundations for this R&D should include biological reference materials and clinical care standards as well as basic biological understanding of diseases and the factors that affect emergence and transmission, as well as clinical research.
- Expand R&D for “Disease X”, including investment in platform technologies for R&D on epidemic risk diseases and harnessing the potential of technological developments such as real-time genetic sequencing and geospatial mapping.
- Improve the ability to do R&D on epidemic risk diseases
- National regulatory authorities should develop and improve pathways for emergency use of products that are fit for purpose.
- Work to expand the use of adaptive clinical trial models and other innovative approaches to R&D, that generate the most actionable findings and are appropriate for studying epidemic risk diseases, especially in the places where those diseases happen.
- Significant strengthening of country capacities, especially those with few resources, including ethics, regulatory capacity, and technical and clinical skills, to ensure that innovative R&D approaches such as adaptive trials and human infection studies are ethical, rigorous and can take place when and where they are needed.
- Implementation research should be integrated in the design and review of response activities, to ensure continual learning of what works, to inform future preparedness and response activities.
R&D for Epidemic
Outbreaks of human infectious diseases have devastating consequences for lives and livelihoods around the world. Research and development (R&D), including fundamental scientific research, social sciences, ethics, epidemiology, product development and clinical research, is critical to understand and stop these infectious disease outbreaks.
However, the window to study these diseases and develop approaches to tackle their spread, can be short and infrequent, often happening in places that lack the infrastructure for R&D. Research during an emergency response is often the only or most effective opportunity for determining the safety and efficacy of interventions or products such as a diagnostic, therapeutic or vaccine.[White House United States Government (2019). Global Health Security Strategy, Available from: https://www.whitehouse.gov/wp-content/uploads/2019/05/GHSS.pdf [Accessed 15 May 2019] ]
This relies on the work done in preparation, such as the preclinical studies with preliminary safety and efficacy data for a therapeutic, or the underlying anthropological or epidemiological knowledge needed to develop an intervention for an outbreak. As a result, approaches to R&D have adapted to these different circumstances (Figure 1) and will need to continue to do so.
Research is now widely accepted as a key component of the response to epidemics following progress in recent years. Take Ebola viruses, first identified in 1976 and emerging periodically in Central African countries over the next few decades. Efforts to develop vaccines against these viruses remained stuck in the early stages of R&D for years, with no human safety studies either between or during outbreaks.
This changed in the 2014-2016 West Africa Ebola epidemic, which demonstrated the ability to do research in outbreaks, and the role of countries where research is conducted. Increased efforts to accelerate R&D for preparedness have paid off by creating the tools needed to respond to outbreaks, such as the portfolio of Ebola vaccines in late stage development.
The Ebola vaccine rVSV-ZEBOV and the cAd3 vaccine were trialled Liberia, with rVSV-ZEBOV also trialled in Sierra Leone followed by a phase II trial in Guinea in 2015. rVSV ZEBOV was then used in the DRC to control a relatively small outbreak in the west of the country in May 2018.
The vaccination strategy using rVSV ZEBOV in the much larger epidemic in the DRC’s North Kivu/Ituri region since August 2018 shows the benefits of preparedness and international collaboration (Box 1).
The availability of the protocol and swift deployment of trained personnel and equipment meant that the vaccination strategy started seven days after the declaration of the outbreak. Over 180,000 people in DRC4 have been vaccinated since [WHO, External Situation Report 51, Ebola Virus Disease, Democratic Republic of Congo. Available from: https://apps.who.int/iris/bitstream/handle/10665/326015/SITREP_EVD_DRC_20190721-eng.pdf?ua=1 [Accessed 12August 2019]], in an effort that has helped manage the spread of the disease in an extremely challenging situation amid security issues, conflict and other humanitarian needs. Preliminary analysis indicates high vaccine efficacy and that the vaccination strategy is a highly efficient delivery method [WHO (2019). Preliminary results on the efficacy of rVSV-ZEBOV-GP Ebola vaccine using the ring vaccination strategy in the control of an Ebola outbreak in the Democratic Republic of the Congo: an example of integration of research into epidemic response. Available from: https://www.who.int/csr/resources/publications/ebola/ebola-ring- vaccination-results-12-april-2019.pdf [Accessed 16 May 2019]], although there are methodological limitations with the data. Serious difficulties with contact tracing due to conflict and displacement of people are posing significant challenges in getting the epidemic under control, but we assume it would have been worse without the vaccine.
However, the vaccine is still unlicensed and the path to bringing other vaccine candidates forward has been slow.


Founding for R&D – lack of data on epidemic R&D
It is challenging to find good data on the levels of investment in R&D related to epidemic risk diseases. We need better monitoring and reporting of these investments in order to more accurately track progress in preparedness.
Over recent years, spending on R&D for neglected diseases as a whole has increased above inflation[GFINDER (2018). Neglected Disease Research and Development:
Reaching New Heights. Available from: https://www.policycuresresearch.org/wp-content/uploads/Y11_GFINDER_Full_report_Reaching_new_heights.pdf. [Accessed 12 June 2019] ]. Figure 2 provides a breakdown of the areas in which these investments have been made over 10 years, with the vast majority going towards vaccines, basic research and therapeutics, representing 36%, 22% and 20% respectively. Between 2008-2017, public funding from LMICs increased, reaching US$105m (up $17m) in 2017, its highest share of public funding (4.5%) since 2013.
India was responsible for over 70% of the total LMIC public funding and was largely responsible for this increase in LMIC public funding compared with 2016. South Africa also provided its highest ever level of government funding ($14m).

Significant investment from public funding for neglected diseases R&D
R&D investments for neglected diseases are up 7% from 2016 to 2017, totalling US$3,566 million10. The top ten funders and their investment in neglected diseases R&D is shown in Figure 3. As in previous years, HIV/AIDS, malaria and tuberculosis (TB) collectively received more than two thirds of funding, $2,496m[GFINDER (2018). Neglected Disease Research and Development:Reaching New Heights. Available from: https://www.policycuresresearch.org/wp-content/uploads/Y11_GFINDER_Full_report_Reaching_new_heights.pdf. [Accessed 12 June 2019]].
Note that neglected diseases included in the G- FINDER data do not include those on the WHO R&D Blueprint priority list. This data is lacking for investment in R&D for epidemic risk diseases, however data on neglected diseases shows relevant trends in major funders and investment in R&D.

Progress has been made in recognising the valuable role that social and behavioural sciences play in research response to epidemics. Even though social and behavioural sciences have been involved in outbreaks and epidemics risk R&D for years, there has recently been much greater visibility of this work.
The Ebola Response Anthropology Platform, as part of the Scientific Advisory Group for Emergencies (SAGE), helped to shape UK policy in Sierra Leone and has received attention for its efforts in the West Africa Ebola epidemic [Institute of Development Studies (2016). IDS-led team wins first prize for social science response to Ebola,
https://www.ids.ac.uk/news/ids-led-team-wins-first-prize-for-social-science-response-to-ebola/
—- Institute of Development Studies (2017). A ‘real-time’ and anthropological response to the Ebola crisis,
https://www.ids.ac.uk/opinions/a-real-time-and-anthropological-response-to-the-ebola-crisis/ ].
The Ebola Response Anthropology Platform enabled social scientists and outbreak control teams to interact and develop a coordinated, adaptive and iterative response to the Ebola outbreak.
The core activity was providing rapid response by email, conference call and online dialogue to operational questions raised by those working for NGOs, government and international agencies to contain the epidemic or care for those affected.
Social science has demonstrated its potential to save live, humanise outbreak responses, and mitigate the disruptive socio-economic and psychosocial burdens associated with outbreaks.
Despite this development in the profile and relevance of social and behavioural sciences research related to epidemics, there is a lack of data on funding at an international level.
Funding for the pipeline of R&D Products
While there are a number of long-standing programmes to fund epidemics related R&D, a few are worth noting. The European Union provides financial support for relevant projects through their Horizon 2020 programme as well as through the European and Developing Countries Clinical Trials Partnership (EDCTP), which invested €652.5 million in 442 projects between 2003 and 201814.
The European Union funded Innovative Medicines Initiative (IMI) has also funded product development for epidemic risk diseases, notably Ebola and zoonotic diseases.
The US Biomedical Advanced Research and Development Authority (BARDA) and US National Institutes for Health (NIH) have invested significantly in pandemic influenza products, including diagnostics, therapeutics and vaccines, as well as epidemics R&D more broadly.
In 2017, the African Union established the Africa Centre for Disease Control and Prevention (CDC), a significant demonstration of political support and investment for improved surveillance, emergency response and prevention of infectious diseases.
There has also been greater investment in epidemics related R&D since 2014. Established in 2017, the Coalition for Epidemic Preparedness Innovations (CEPI), is a partnership of public, private, philanthropic and civil society organisations that aims to stimulate, finance and coordinate vaccine development for emerging infectious diseases.
CEPI brings together often-siloed aspects of R&D for vaccines and has committed to investing a total of $370 million in 13 candidate vaccines for diseases on the R&D Blueprint priority list as well as vaccine platform technologies for Disease X (Table 1).
CEPI has received multi-year funding from Norway, Germany, Japan, Canada, Australia, the Bill & Melinda Gates Foundation, and Wellcome Trust, reaching over US$ 750 million of its $1 billion funding target. CEPI has also received single-year investments from the governments of Belgium and the United Kingdom.
There has also been significant investment into the antimicrobial drug development pipeline in the form of CARB-X, which will invest US$550 million. $300 million of this commitment is from the US Government, and although not an epidemic-specific initiative, it demonstrates that there is appetite for pooling public and private funds to address global health challenges like antimicrobial resistance.
The large public investments in CEPI demonstrate that the political will and support that exists for R&D for epidemic risk diseases has moved up the agenda in several countries.

REFERENCES
- BIS (Bank for International Settlements). Assessing the economic costs and benefits of TLAC implementation. Basel, Switzerland: BIS; 2015.
- Burns A, van der Mensbrugghe D, Timmer H. Evaluating the economic consequences of avian influenza. Washington, DC: World Bank; 2008.
- CDC (Centers for Disease Control and Prevention). Reconstruction of the 1918 Influenza Pandemic Virus. 2014. [November 15, 2015]. http://www.cdc.gov/flu/about/qa/1918flupandemic.htm.
- CDC. 2014 Ebola outbreak in West Africa—case counts. 2016. [February 1, 2016]. http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/casecounts.html.
- CIA (Central Intelligence Agency). The world factbook. 2015. [November 30, 2015]. https://www.cia.gov/library/publications/the-world-factbook/geos/xx.html.
- Fonkwo PN. Pricing infectious disease: The economic and health implications of infectious diseases. EMBO Reports. 2008;9(Suppl 1):S13–S17. [PMC free article] [PubMed]
- Gates B. The next epidemic—lessons from Ebola. New England Journal of Medicine. 2015;372(15):1381–1384. [PubMed]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. [PMC free article] [PubMed]
- Heymann DL, Chen L, Takemi K, Fidler DP, Tappero JW, Thomas MJ, Kenyon TA, Frieden TR, Yach D, Nishtar S, Kalache A, Olliaro PL, Horby P, Torreele E, Gostin LO, Ndomondo-Sigonda M, Carpenter D, Rushton S, Lillywhite L, Devkota B, Koser K, Yates R, Dhillon RS, Rannan-Eliya RP. Global health security: the wider lessons from the West African Ebola virus disease epidemic. Lancet. 2015;385(9980):1884–1901. [PMC free article] [PubMed]
- Johnson NPAS, Mueller J. Updating the accounts: Global mortality of the 1918–1920 “Spanish” influenza pandemic. Bulletin of the History of Medicine. 2002;76:105–115. [PubMed]
- Jonas O. Pandemic risk. Washington, DC: World Bank; 2014.
- Jones KE, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL, Daszak P. Global trends in emerging infectious diseases. Nature. 2008;451(7181):990–993. [PMC free article] [PubMed]
- Lee JW, McKibbin WJ. Estimating the global economic costs of SARS. Washington, DC: The National Academies Press; 2004. pp. 92–109.
- McKibbin WJ, Sidorenko AA. Global macroeconomic consequences of pandemic influenza. Sydney, Australia: Lowy Institute for International Policy, The Australian National University; 2006.
- Poincaré H. La valeur de la science. Paris: Flammarion; 1905.
- Sachs J, Malaney P. The economic and social burden of malaria. Nature. 2002;415(6872):680–685. [PubMed]
- Siu A, Wong RYC. Economic impact of SARS: The case of Hong Kong. Cambridge, MA: MIT Press; 2004. (Asian Economic Papers).
- UNAIDS (Joint United Nations Programme on HIV/AIDS). Fact sheet 2014—global statistics. 2014. [February 1, 2016]. http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/factsheet/2014/20140716_FactSheet_en.pdf.
- UNDG (United Nations Development Group)–Western and Central Africa. Socio-economic impact of Ebola virus disease in West African countries. Addis Ababa, Ethiopia: UNDG; 2015.
- World Bank. The economic impact of the 2014 Ebola epidemic: Short and medium term estimates for West Africa. Washington, DC: World Bank; 2014.
- WHO (World Health Organization). Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003. 2003. [February 1, 2016]. http://www.who.int/csr/sars/country/table2003_09_23/en.
- WHO. Ebola Situation Report—20 January 2016. 2016. [February 1, 2016]. http://apps.who.int/ebola/current-situation/ebola-situation-report-20-january-2016.



{kind=link}