










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



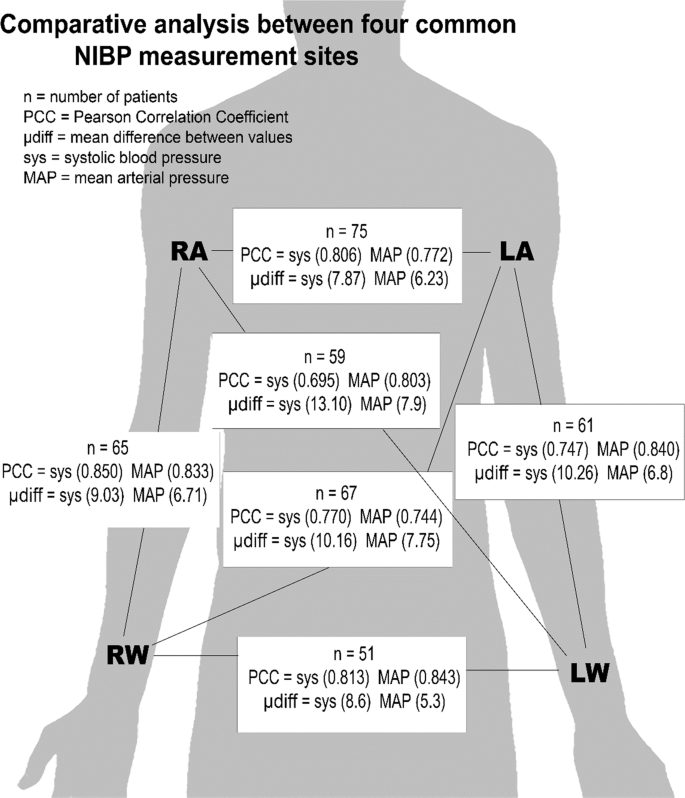
Blood pressure readings taken from neuroscience intensive care unit (NSICU) patients had marked differences between opposite sides of the body and different anatomical sites in each individual, highlighting the significant and sometimes extreme variability of this measure even in the same person depending on where it’s taken, researchers from UT Southwestern Medical Center report in a new study.
The findings, published online Feb. 25, 2020, in Scientific Reports and the 100th research paper published by nurses at UTSW, could eventually impact how blood pressure information – which informs a variety of medical decisions in the NSICU and beyond – is collected.
Having an accurate blood pressure reading is essential to delivering often lifesaving care, say UT Southwestern study leaders Kathrina B. Siaron, B.S.N., R.N., a neurocritical care nurse, and DaiWai M. Olson, Ph.D., R.N., a professor of Neurology and Neurotherapeutics and Neurological Surgery.
“For our patients in the NSICU, blood pressure often needs to be maintained in a very narrow range,” Siaron says. “Moving it one way or another could potentially harm the patient.”
It’s also a parameter that’s been measured much the same way for over a century, she explains: Patients wear a cuff around the upper arm, wrist, or thigh for noninvasive assessments, or a thin plastic catheter is inserted into their arteries for invasive measures, with arterial pressure long considered the gold standard and thought to be within 10 points of blood pressure in the upper arm.
Although it’s well known that blood pressure can vary dramatically between patients or in the same patient from moment to moment, medical care providers have long assumed that there was little variation between these measures at different sites on the same patient.
To test this idea, Siaron, Olson, and their colleagues worked with 80 patients admitted to UT Southwestern’s NSICU between April and July 2019.
These patients – split almost equally between men and women with a mean age of about 53 – were admitted to the unit for a variety of common serious neurological problems, including stroke, subarachnoid hemorrhage, and brain tumors.
The researchers had these patients sit upright in their hospital beds, wearing blood pressure cuffs on both upper arms connected to different, precisely calibrated machines.
Simultaneously, clinicians activated the machines to take readings, then recorded them. They then had the patients wear wrist cuffs and performed the same exercise.
For the 29 patients who also had arterial blood pressure sensors, values from those devices were recorded while patients were receiving noninvasive blood pressure readings.
As expected, there were often large blood pressure differences from patient to patient. However, there were also significant differences in individual patients from site to site.
There was a mean difference of about 8 points in systolic pressure (the top number in blood pressure values) between upper arms, and a mean difference of up to 13 points between upper arm and wrist systolic values.
Diastolic measures (the bottom number in blood pressure values) varied by a mean of about 6 points between arms and about 5 points between upper arms and wrists.
Arterial pressure often varied significantly from each of the values – sometimes as much as 15 points higher or lower.
Although the mean differences between sites were just a few points on average, they differed by as much as 40 points between some patients, says Olson – a dramatic difference that could radically affect what type of care that patient receives.
“If we take pressure in one arm, a patient seems fine, but in the other arm, they’re in a crisis,” he says.
“The values we collected were really all over the place. There was no consistency between the same arm or wrist between different patients.”
It’s unclear why these differences exist between sites, adds Siaron – blood pressure numbers could be affected by an assortment of factors, such as a patient’s posture, anatomical differences, or medical conditions that affect blood flow.
The team plans to continue to study blood pressure among different anatomical sites in varying populations, such as patients in the general ICU or healthy volunteers.
Eventually, they say, blood pressure might be collected using a totally different protocol, such as averaging the values between two sides of the body or accepting the highest number.
Blood pressure variability (BPV) is an independent cardiovascular risk factor in hypertensive patients. The best method for quantifying BPV is still an object of debate. The existence of different BPV patterns, particularly age and arterial stiffness related, is postulated. Our aims were:
- i)to compare BPV using different blood pressure (BP) measurement methods
- ii)to compare different calculation approaches
- iii)to analyze the predictors of BPV.
Cross-sectional study in 108 elderly hypertensive hospitalized patients. Each patient underwent blood pressure measurements with 5 different modalities: 24 hour BP and pulse wave velocity (PWV) monitoring (24hBPM), measurement by nurses or physicians, self-measurement and beat-to-beat monitoring. Differences between maximum and minimum values (ΔBP), averages of the absolute differences between consecutive values (ARV) and coefficients of variation (CV) were calculated.
ΔBP showed the wider values’ dispersion (Δ systolic blood pressure (SBP): 66.4 ± 22.9 and Δ diastolic blood pressure [DBP]: 45.0 ± 13.5 mmHg).
ARV and CV were highest with nurses’ measurements (SBP-ARV 9.2 ± 6.2; DBP-ARV 6.9 ± 5.2; SBP-CV 7.6 ± 5.3; DBP-CV 9.6 ± 5.5).
The strongest correlation was found comparing physicians’ SBP measurements and 24hBPM ARVs (R2 0.23, P <.05). 24hBPM ΔSBP in a multivariate analysis was significantly associated with age (β −3.85, SE 0.83; P <.001) and PWV (β 20.29, SE 3.70; P <.001).
Calcium antagonists were associated with a lower ΔSBP (β −14.6, SE 6.1, P <.05) while diuretics and alpha-blockers with a significant increase (β 14.4 SE 5.4, P <.01; β 26.9 SE 11.7, P <.05).
Age, PWV, diuretics, alpha-blockers, but also measurements obtained by nurses, increase BP variability while calcium antagonists reduce it.
BP profiles in elderly in-hospital patients potentially provide important information; they should, however, be interpreted cautiously.
Discussion
In this study, we confirmed that blood pressure variability is a blood pressure measurement method dependent phenomenon and that the different mathematical determinants of variability used, likely assess peculiar aspects of individual blood pressure behavior.
In our population sample, poor correlation was seen comparing respectively blood pressure obtained with the different methods proposed and the estimators of variability.
BP measured by nurses showed the highest variability values compared with measurement performed by physicians and self-measurements.
Although blood pressure variability represents an intriguing research field, with notable clinical and patient outcome implications, 1 important issue still has to be clarified.
To date, neither consensus nor gold standard has been published on how and with which method variability should be estimated.
Our proof of concept study is the first one comparing several approaches to calculate blood pressure variability in a specific and distinctive population composed of over 70-year-old in-hospital hypertensive patients.
Previous findings did already analyze the topic, highlighting a poor correlation between methods used for variability estimation and investigating the variability agreement between ABPM and beat-to-beat and between ABPM and self-measurements.[21–24]
However, our study is the first one in which a full between-methods comparison of blood pressure variability was explored starting from 5 different blood pressure assessment strategies.
Furthermore, a wide and exhaustive comparison between blood pressure variability assessment methods was performed. No former study did indeed investigate these variables using 3 different determinants of short-term variability (ARV, CV, and ΔBP).
Furthermore, in previous studies, younger populations in heterogeneous environmental circumstances and potentially with several factors influencing punctual BP fluctuations were evaluated.[23,24]
Finally, our study is the first one aimed at comparing BPV, also analyzing values obtained with a continuous beat-to-beat noninvasive monitoring system (Finometer).
Our choice to calculate 3 different determinants of short-term variability arises from the attempt to highlight peculiarities of the within-individual differences; peculiarities that can only partially be investigated by BPV determinants dependent on the mean BP.[25,26]
In our population, variability calculated on the basis of BP measured by beat-to-beat showed the better systolic and diastolic correlation with values obtained from the 24hBPM. Similarities and differences between BPV determinants were highlighted by the fact that some of them only showed a significant correlation.
Recently, findings of observational studies showed an association between ABPM-BPV and arterial stiffness. This association was more evident focusing on short-term BP variability determinants such as ARV and CV.[27–28]
Furthermore, a strong association between arterial stiffness, estimated with a beat-to-beat analyzer in a hypertensive population, and Systolic BPV was shown.[29]
Our study confirms, in an in-hospital elderly population, the association between high beat-to-beat BPV and the magnitude of vascular damage measured by pulse wave velocity obtained with an independent method (24hBP and PWV monitor).
The fact that arterial stiffness confirms a correlation with the amplitude of BP fluctuations, does not, however, tell us in which way BPV itself impacts on the progression of vascular damage.
In our data, moreover, PWV was significantly higher in the High-BPV group. Finally, a rise in PWV correlates with an increase in BP variability for both 24hBPM and measurements obtained by physicians.
Recently, great interest was shown in exploring the contribution of different classes of antihypertensive medications on BPV. In our study, we attempt to provide an estimation of the impact of calcium antagonists, diuretics, alpha-blockers, beta-blockers, and renin angiotensin aldosterone system inhibitors on BPV.
As suggested from previous findings, we confirm the association between the use of calcium antagonists and low BPV values. Interestingly, the effect of calcium antagonists on beat-to-beat BP variability was not previously highlighted.
Furthermore, increasing the interest in the topic, it was shown in a previous study, that BPV reduction related to calcium antagonist treatment was associated with a concomitant improvement in baroreflex sensitivity, suggesting this mechanism as one of the components of BP stabilization.[30]
Diuretics and, as recently shown, alpha- blockers, confirm on the contrary an association with higher BPV values.[31]
Moreover increasing evidence suggests a relationship between BPV and, falls, symptomatic hypotension and syncope, mostly in elderly people.[32,33]
However, in our study, due to the limited number of patients admitted for the cited diagnoses, we were unable to conduct a targeted sub-analysis. For the same reason, even if some diagnoses justifying hospital admission, especially infections, could impact BPV, we did not investigate their potential role.
We have to acknowledge some limitations of our study. Firstly, the observational design, which does not allow to conclude definitively about causality.
Moreover, some strong associations found in our data could not be recognizable in younger patient or in population samples with other characteristics. As a consequence of structural vessel changes, diminished baroreflex sensitivity and enhanced response to sympathetic activation related to increased arterial stiffness, elderly patients represent, in fact, a population with a non-linear and extremely variable pattern of arterial aging and BP behavior. [34]
Moreover, our study was conducted in hospitalized patients; in a setting far from the patient’s everyday life in which blood pressure shows a peculiar pattern, related to several influencing factors (e.g., stress generating circumstances, prescription of drugs influencing BP,…), susceptible to impact on reliability and variability and associated with a higher prevalence of symptomatic and asymptomatic orthostatic hypotension.[35]
Finally, even if we did not consider the BP values of the first 2 days, to reduce in particular the impact on BP of the adrenergic response to environmental adaptation and the magnitude of white coat hypertension, we cannot exclude a residual hospital mediated “stress-response”.
In this fascinating but still cloudy research field, we can conclude on 1 hand that, individual characteristics and antihypertensive treatments are susceptible to producing peculiar blood pressure variability patterns and on the other that, the way blood pressure is measured and variability is calculated play a significant role.
Age, PWV, diuretics, alpha-blockers, but also measurements obtained by nurses, increase blood pressure variability while calcium antagonists reduce it.
The cited factors of variability are highly prevalent in the in-hospital internal medicine population; setting in which antihypertensive treatments are often readapted.
Blood pressure profiles obtained on the wards, potentially provide important information; they are however difficult to interpret and influenced by numerous biases.
A unique consensus about the way of measuring blood pressure variability and their significance as a function of the patients’ characteristics would be helpful.
References
[1] Stevens SL, Wood S, Koshiaris C, et al. Blood pressure variability and cardiovascular disease: systematic review and meta-analysis. BMJ 2016;354:i4098. [PMC free article] [PubMed] [Google Scholar]
[2] Björklund K, Lind L, Zethelius B, et al. Prognostic significance of 24-h ambulatory blood pressure characteristics for cardiovascular morbidity in a population of elderly men. J Hypertens 2004;22:1691–7. [PubMed] [Google Scholar]
[3] Kikuya M, Hozawa A, Ohokubo T, et al. Prognostic significance of blood pressure and heart rate variabilities: the Ohasama study. Hypertension 2000;36:901–6. [PubMed] [Google Scholar]
[4] Li CL1, Liu R, Wang JR, et al. Relationship between blood pressure variability and target organ damage in elderly patients. Eur Rev Med Pharmacol Sci 2017;21:5451–5. [PubMed] [Google Scholar]
[5] Sega R, Corrao G, Bombelli M, et al. Blood pressure variability and organ damage in a general population: results from the PAMELA study (Pressioni Arteriose Monitorate E Loro Associazioni). Hypertension 2002;39:710–4. [PubMed] [Google Scholar]
[6] Parati G, Ochoa JE, Lombardi C, et al. Blood pressure variability: assessment, predictive value, and potential as a therapeutic target. Curr Hypertens Rep 2015;17:537. [PubMed] [Google Scholar]
[7] Morano A, Ravera A, Agosta L, et al. Extent of, and variables associated with, blood pressure variability among older subjects. Aging Clin Exp Res 2018;30:1327–33. [PubMed] [Google Scholar]
[8] Zhang Y, Agnoletti D, Blacher J. Safar ME Blood pressure variability in relation to autonomic nervous system dysregulation: the X-CELLENT study. Hypertens Res 2012;35:399–403. [PubMed] [Google Scholar]
[9] Lucini D, Cusumano G, Bellia A, et al. reduced baroreflex gain a component of the metabolic syndrome? Insights from the LINOSA study. J Hypertens 2006;24:361–70. [PubMed] [Google Scholar]
[10] Omboni S, Posokhov IN, Rogoza AN. Relationships between 24-h blood pressure variability and 24-h central arterial pressure, pulse wave velocity and augmentation index in hypertensive patients. Hypertens Res 2017;40:385–91. [PubMed] [Google Scholar]
[11] Mena LJ, Felix VG, Melgarejo JD, et al. 24-hour blood pressure variability assessed by average real variability: a systematic review and meta-analysis. J Am Heart Assoc 2017;6:e006895. [PMC free article] [PubMed] [Google Scholar]
[12] Abellán-Huerta J, Prieto-Valiente L, Montoro-García S, et al. Correlation of blood pressure variability as measured by clinic self-measurement at home, and ambulatory blood pressure monitoring. Am J Hypertens 2018;31:305–12. [PubMed] [Google Scholar]
[13] Schutte R, Thijs L, Liu YP, et al. Within-subject blood pressure level–not variability–predicts fatal and nonfatal outcomes in a general population. Hypertension 2012;60:1138–47. [PMC free article] [PubMed] [Google Scholar]
[14] Veloudi P, Blizzard CL, Head GA, et al. Blood pressure variability and prediction of target organ damage in patients with uncomplicated hypertension. Am J Hypertens 2016;29:1046–54. [PubMed] [Google Scholar]
[15] Li W, Yu Y, Liang D, et al. Factors associated with blood pressure variability based on ambulatory blood pressure monitoring in subjects with hypertension in China. Kidney Blood Press Res 2017;42:267–75. [PubMed] [Google Scholar]
[16] Parati G, Ochoa JE, Salvi P, et al. Prognostic value of blood pressure variability and average blood pressure levels in patients with hypertension and diabetes. Diabetes Care 2013;36:S312–24. [PMC free article] [PubMed] [Google Scholar]
[17] Suchy-Dicey AM, Wallace ER, Mitchell SVE, et al. Blood pressure variability and the risk of all-cause mortality, incident myocardial infarction, and incident stroke in the cardiovascular health study. Am J Hypertens 2013;26:1210–7. [PMC free article] [PubMed] [Google Scholar]
[18] Kithas PA, Supiano MA. Hypertension in the geriatric population: a patient-centered approach. Med Clin North Am 2015;99:379–89. [PubMed] [Google Scholar]
[19] Hassan AKM, Abd-El Rahman H, Mohsen K, et al. Impact of in-hospital blood pressure variability on cardiovascular outcomes in patients with acute coronary syndrome. J Clin Hypertens (Greenwich) 2017;19:1252–9. [PubMed] [Google Scholar]
[20] Tan Lai Z, Ronald MA H, Coen DA S, et al. Kroon blood pressure variability, arterial stiffness, and arterial remodeling the maastricht study. Hypertension 2018;72:1002–10. [PubMed] [Google Scholar]
[21] Juhanoja EP, Niiranen TJ, Johansson JK, et al. Agreement between ambulatory, home, and office blood pressure variability. J Hypertens 2016;34:61–7. [PubMed] [Google Scholar]
[22] Muntner P, Shimbo D, Diaz KM, et al. Low correlation between visit-to-visit variability and 24-h variability of blood pressure. Hypertens Res 2013;36:940–6. [PMC free article] [PubMed] [Google Scholar]
[23] Abellán-Huerta J, Prieto-Valiente L, Montoro-García S, et al. Correlation of blood pressure variability as measured by clinic, self-measurement at home, and ambulatory blood pressure monitoring. Am J Hypertens 2018;31:305–12. [PubMed] [Google Scholar]
[24] Wei FF, Li Y, Zhang L, et al. Beatto-beat, reading-to-reading, and day-to-day blood pressure variability in relation to organ damage in untreated Chinese. Hypertension 2014;63:790–6. [PubMed] [Google Scholar]
[25] Clement DL, Mussche MM, Vanhoutte G, et al. Is blood pressure variability related to activity of the sympathetic system. Clin Sci 1979;57suppl 5:S217–9. [PubMed] [Google Scholar]
[26] Mancia G, Ferrari A, Gregorini L, et al. Blood pressure variability in man: its relation to high blood pressure, age and baroreflex sensitivity. Clin Sci 1980;59suppl 6:S401–4. [PubMed] [Google Scholar]
[27] Stabouli S, Papakatsika S, Kotronis G, et al. Arterial stiffness and SBP variability in children and adolescents. J Hypertens 2015;33:88–95. [PubMed] [Google Scholar]
[28] Schillaci G, Bilo G, Pucci G, et al. Relationship between short-term blood pressure variability and large-artery stiffness in human hypertension: findings from 2 large databases. Hypertension 2012;60:369–77. [PubMed] [Google Scholar]
[29] Xia Y, Liu X, Wu D, et al. Influence of beat-to-beat blood pressure variability on vascular elasticity in hypertensive population. Sci Rep 2017;7:8394. [PMC free article] [PubMed] [Google Scholar]
[30] Frattola A, Parati G, Castiglioni P, et al. Lacidipine and blood pressure variability in diabetic hypertensive patients. Hypertension 2000;36:622–8. [PubMed] [Google Scholar]
[31] Clements B, Allred N, Riessen E, et al. Effect of antihypertensive class on visit-to visit office blood pressure variability and its effect on all cause mortality. JACC 2018;71(11 Supp):A1909. [Google Scholar]
[32] Goh CH, Ng SC, Kamaruzzaman SB, et al. Evaluation of two new indices of blood pressure variability using postural change in older fallers. Medicine (Baltimore) 2016;95:e3614. [PMC free article] [PubMed] [Google Scholar]
[33] Li TC, Li CI, Liu CS, et al. Visit-to-visit blood pressure variability and hip fracture risk in older persons. Osteoporos Int 2019;30:763–70. [PubMed] [Google Scholar]
[34] Gabutti L, Del Giorno R. Vascular aging processes accelerate following a cubic kinetic: pulse wave velocity as an objective counterpart that time, as we age, goes by faster. Clin Interv Aging 2018;13:305–7. [PMC free article] [PubMed] [Google Scholar]
[35] Cappelleri C, Janoschka A, Berli R, et al. Twenty-four-hour ambulatory blood pressure monitoring in very elderly patients: comparison of in-hospital versus home follow-up results. Medicine (Baltimore) 2017;96:e7692. [PMC free article] [PubMed] [Google Scholar]
More information: Kathrina B. Siaron et al, Blood Pressure measurements are site dependent in a cohort of patients with neurological illness, Scientific Reports (2020). DOI: 10.1038/s41598-020-60414-7



{kind=link}