")










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



While both sexes have the capacity for phenomenal athletic achievements, women on average must work harder to breathe during strenuous exercise compared to men, according to new research.
The study suggests one possible way sex could affect exercise dynamics and potentially also contribute to differences in how men and women experience airway disorders such as asthma and chronic obstructive pulmonary disease (COPD).
“The amount of work the respiratory muscles have to do to breathe a given volume is greater in women,” said Paolo Dominelli, PhD, assistant professor at the University of Waterloo in Canada.
“It is thought that this is due to women having smaller airways than men, which causes the airflow resistance to be higher.”
Dominelli was scheduled to present the research at the American Physiological Society annual meeting in San Diego this month.
Though the meeting, to be held in conjunction with the 2020 Experimental Biology conference, was canceled in response to the COVID-19 outbreak, the research team’s abstract was published in this month’s issue of The FASEB Journal.
The research team recruited six men and five women to perform two maximal exercise tests, in which participants gradually increased their level of exertion on a stationary cycle until they were exercising as hard as they could.
Participants breathed through a mouthpiece attached to a large bag. During one session, the bag was filled with normal room air.
During the other, the bag was filled with a mixture of oxygen and helium. Each bag contained the same amount of oxygen, and participants were not told which mixture they were breathing on which day.
A small tube was inserted into participants’ nose and throat during the tests to monitor the pressure inside the esophagus.
This procedure allowsthe researchers to measure the amount of work required to breathe. When the bag contained the helium mixture, the results showed no differences in the work of breathing between men and women. When it contained room air, breathing required significantly more work for women than men.
The experiment was designed to mimic how men’s larger airways reduce breathing resistance. The helium mixture is much less dense than room air and, as a result, flows in a more laminar manner.
In a laminar flow, air molecules are all flowing in the same direction, like water in a smooth river. In a turbulent flow, air molecules swirl in different directions, akin to the eddies that form around a boulder in the middle of a river.
Turbulent flow in the airways causes more resistance, which requires more work to overcome.
“Two big factors that determine whether flow is laminar or turbulent is the size of the airway and the flow,” Dominelli explained.
“At rest, the rate of air flow is very low, so even though women have smaller airways than men, air flow is still laminar. As exercise intensity increases, you breathe faster, and at some point the airflow goes from laminar to turbulent.
Air flow in men’s airways will also eventually turn from laminar to turbulent, but this requires a higher rate of air flow than is required in women.”
Dominelli cautioned that the differences observed in the study relate to size and sex, and that there is great variability in airway size among different individuals. Although men on average have larger airways, a man and woman of the same height could have similar-sized airways.
Nonetheless, the research provides useful insights on basic physiology at a population level and could also help researchers better understand how airway diseases affect the transition from laminar to turbulent flow in women and men.
Chronic obstructive pulmonary disease (COPD) is a progressive disorder characterized by airflow limitation and is a major cause of chronic morbidity and mortality across the world.
Approximately 65 million people suffer from COPD and 3 million deaths occur from it annually, making it the third leading cause of death globally.1
The importance and significance of COPD management has been well documented.2
Until some years ago, COPD diagnosis has in many cases been neglected in women as it was considered a disease that primarily affects men.
According to some of the earlier reports, there was either no gender disparity in undiagnosed COPD3 or women were at the greater risk of undiagnosed COPD.4,5 However, recent studies demonstrated that the prevalence of COPD is similar among men and women.6,7,8,9,10,11
A study by Mamary et al.12 reported that men were more prone to have underdiagnosis of COPD than women. Furthermore, mortality among women due to COPD is higher than from many of the most commonly recognized forms of cancer.10
In a Swedish study, COPD mortality among women increased during 1999–2009, and life expectancy in the COPD population was 9.4 years lower for women (vs. 7.4 years lower in men) compared with that of the average Swedish population.13
Several findings also suggested that health status and quality of life is more impaired in women than in men with COPD.14,15,16,17,18,19
The above-mentioned findings reflect the increased incidence of smoking among females over the past decades in several countries. Although the smoking prevalence in Sweden has decreased during the period of 2006–2016, since many years it is been higher for women than men (9.6% vs. 8.0% in 2016).20
However, in most countries, women smoke less than men, suggesting that females may be more severely affected by COPD than males and are more susceptible to the harmful effects of smoking, thereby developing COPD more easily than males.21
In a large population-based study, female gender was associated with reduction in lung function and more severe disease among COPD patients with early onset of disease or low tobacco exposure.22
According to a systematic review, the annual decline in forced expiratory volume in 1 s was faster in female smokers compared with male smokers despite they smoke less.23
Findings from mainly observational studies point to a gender-specific susceptibility and morbidity, and it is important to generate real-world evidence to better understand the gender aspects of COPD. In Sweden, most patients with COPD are managed in primary care.
Therefore, the aim of this study was to provide real-world evidence on gender differences with respect to diagnosis and outcomes among COPD patients in the Swedish primary care setting and to identify areas for improvement and management of such patients.
Results
Patient demographics
Of the identified 18,586 eligible patients with a COPD diagnosis listed in electronic medical records (EMRs), 291 patients were excluded because they were diagnosed with COPD before 40 years of age. Following case–control matching, a total of 17,479 patients with COPD (International Classification of Diseases, tenth revision [ICD-10] code: J44) were included under cases and they were compared with 84,455 age- and gender-matched controls.
The patients were followed for a mean (standard deviation) duration of 12.4 (4.6) years. Patient demographics of the COPD patients and the reference population stratified by gender are summarized in Table 1.
In the COPD cohort, the mean age was 68.2 years for females and 68.9 years for males. The proportion of females (54.4%) was higher compared with males (45.6%). At baseline, women were younger and had a lower Charlson comorbidity index (CCI) value compared with men.
Prevalence of asthma was also significantly higher in women (p < 0.0001). Furthermore, although women had a higher number of primary care contacts, they had fewer overnight stays than men.
The healthcare resource utilization data included both COPD and non-COPD, that is, comorbidity-related events. A significantly higher number of women used inhaled corticosteroids (ICSs) and oral corticosteroids (OCSs) compared to men.
However, no significant difference was observed with respect to body mass index between the genders in both COPD and reference population.
Table 1 Patient demographics of the COPD and reference groups stratified by gender.
| Variable | Females, COPD (N = 9506) | Males, COPD (N = 7973) | p value | Females, ref. population (N = 47,744) | Males, ref. population (N = 36,711) | p Value |
|---|---|---|---|---|---|---|
| Age (years), mean (SD)a | 68.19 (11.4) | 68.87 (10.7) | <0.0001 | 65.2 (12.5) | 64.7 (11.1) | <0.0001 |
| Body mass index (kg/m2), mean (SD) | 25.92 (5.9) | 26.24 (5.0) | 0.0744 | 27.47 (5.6) | 27.23 (4.2) | 0.1807 |
| CCI valueb, mean | 1.62 | 1.78 | <0.0001 | 1.30 | 1.37 | <0.0001 |
| Healthcare utilizationa | ||||||
| Outpatient visits per year, mean ± SD | 1.74 | 1.82 | 0.17 | 1.54 | 1.44 | <0.0001 |
| Primary care visits per year, mean ± SD | 10.39 | 9.46 | 0.0006 | 5.12 | 4.45 | <0.0001 |
| Overnight stays, n (%) | 3148 (33.12) | 2894 (36.30) | <0.0001 | 10,869 (22.77) | 8628 (23.50) | 0.01 |
| Patients with outpatient hospital visits, n (%) | 5740 (60.38) | 4835 (60.64) | 0.73 | 28,290 (59.25) | 20,367 (55.48) | <0.0001 |
| Comorbiditiesa,c, n (%) | ||||||
| Respiratory diseases (including COPD and asthma) | 3613 (38.01) | 2769 (34.73) | <0.0001 | 6774 (14.19) | 4376 (11.92) | <0.0001 |
| Cardiovascular diseases | 3417 (35.95) | 3319 (41.63) | <0.0001 | 10,257 (21.48) | 9315 (25.37) | <0.0001 |
| Hypertensive diseases | 2170 (22.83) | 1849 (23.19) | 0.57 | 6418 (13.44) | 5275 (14.37) | 0.0001 |
| Asthma | 1554 (16.35) | 977 (12.25) | <0.0001 | 2649 (5.55) | 1428 (3.89) | <0.0001 |
| Any cancer | 1180 (12.41) | 1121 (14.06) | 0.0013 | 5179 (10.85) | 3875 (10.56) | 0.1739 |
| Other forms of heart diseases | 1138 (11.97) | 1366 (17.13) | <0.0001 | 2539 (5.32) | 2849 (7.76) | <0.0001 |
| Fractures | 678 (7.13) | 448 (5.62) | <0.0001 | 2734 (5.73) | 1335 (3.64) | <0.0001 |
| Depression | 649 (6.83) | 313 (3.93) | <0.0001 | 1510 (3.16) | 668 (1.82) | <0.0001 |
| Diabetes, type II | 546 (5.74) | 707 (8.87) | <0.0001 | 1745 (3.65) | 2114 (5.76) | <0.0001 |
| Anxiety | 455 (4.79) | 243 (3.05) | <0.0001 | 956 (2.00) | 439 (1.20) | <0.0001 |
| Rheumatoid arthritis | 204 (2.15) | 97 (1.22) | <0.0001 | 624 (1.31) | 184 (0.50) | <0.0001 |
| Diabetes, type I | 160 (1.68) | 180 (2.26) | 0.006 | 677 (1.42) | 743 (2.02) | <0.0001 |
| Kidney disease | 114 (1.20) | 209 (2.62) | <0.0001 | 259 (0.54) | 340 (0.93) | <0.0001 |
| Lung cancer | 88 (0.93) | 88 (1.10) | 0.2404 | 99 (0.21) | 82 (0.22) | 0.6180 |
| Polymyalgia rheumatica | 81 (0.85) | 40 (0.50) | 0.0054 | 281 (0.59) | 101 (0.28) | <0.0001 |
| Nasal polyps | 39 (0.41) | 53 (0.66) | 0.0206 | 124 (0.26) | 218 (0.59) | <0.0001 |
| Medication usec, n (%) | ||||||
| Inhaled corticosteroids | 2623 (27.59) | 1816 (22.78) | <0.0001 | 5550 (11.62) | 2892 (7.88) | <0.0001 |
| Oral steroids | 1897 (19.96) | 1219 (15.29) | <0.0001 | 4028 (8.44) | 2222 (6.05) | <0.0001 |
- ATC anatomical therapeutic chemical, CCI Charlson comorbidity index, COPD chronic obstructive pulmonary disease, ICD International Classification of Diseases, Ref. reference, SD standard deviation
- aAge at index date; comorbidities and healthcare utilization and medication use 2 years before the index date
- bCCI is a method of categorizing comorbidities of patients based on the ICD diagnosis codes found in administrative data, such as hospital abstracts data. Each comorbidity category has an associated weight (from 1 to 6) based on the adjusted risk of mortality or resource use, and the sum of all the weights results in a single comorbidity score for a patient. The higher the score, the more likely the predicted outcome will result in mortality or higher resource use
- CICD-10 codes and ATC codes are reported in Supplementary Tables 1 and 2, respectively
COPD incidence
COPD was more frequent among females than males during the observation period. The percentage of incident distribution for females had been fairly constant at 53.8%. However, a small downward trend was observed among females towards the later years of the observation period.
Presence of asthma (ICD-10: J45/J46)
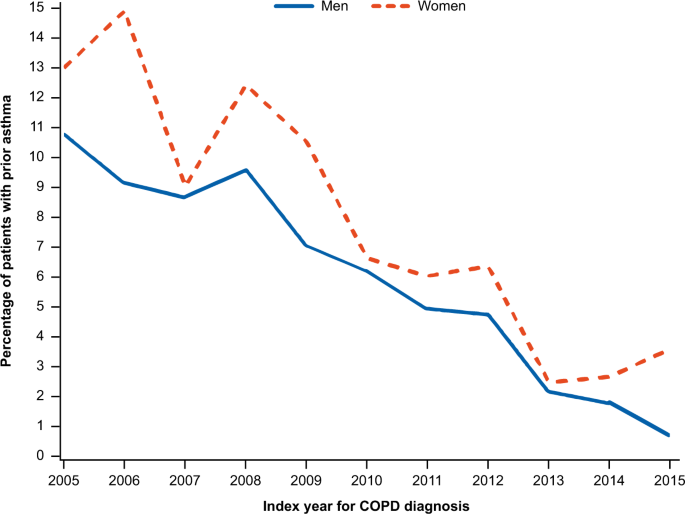
Of the 17,479 COPD patients, 6026 (34.5%) patients had a diagnosis code for asthma at any time point during the study. Of these 6026 patients, 1924 (31.9%) patients had an asthma diagnosis before the index date, while 1272 patients (21.1%) had an asthma diagnosis 0 to 2 years after the index date and 417 (6.92%) patients had an asthma and COPD diagnosis on the same date.
Before the index date, the asthma diagnosis showed marked difference between genders; more females than males had asthma (12.3% vs. 9.4%; p < 0.0001). Towards the later years of the observation period, the percentage of incident patients with the asthma had decreased significantly in both genders (Fig. 1).
Furthermore, no significant difference was observed between males and females in the time period from the asthma diagnosis to the index date (difference: 3.1 years; p = 0.9284).
Comorbidities
The frequency of all comorbidities was higher in the COPD population compared with the reference population when analyzed 3 years before and 3 years after the index date. A gender difference was observed in some of the comorbidities in both COPD and reference populations, and the magnitude of this difference was generally observed to be higher in the COPD population compared with the reference population.
The comorbidities that were more prevalent in females included asthma, fractures, osteoporosis, rheumatoid arthritis, rhinitis, depression, and anxiety. The comorbidities that were more prevalent in males included type I and type II diabetes, kidney diseases, and cardiovascular diseases. The comorbidities where no gender difference was observed included respiratory diseases (excluding COPD and asthma: ICD-10 code J41–J45), polymyalgia rheumatica, nasal polyps, any cancer, lung cancer, dementia, and hyperlipidemia.
Source:
Experimental Biology
References
- 1.Lozano, R. et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (Lond., Engl.) 380, 2095–2128 (2012).
- 2.Chapman, K. R. Increasing awareness of COPD: two steps forward, one step back. Chronic Obstr. Pulm. Dis. 5, 228–230 (2018).
- 3.Hill, K. et al. Prevalence and underdiagnosis of chronic obstructive pulmonary disease among patients at risk in primary care. CMAJ 182, 673–678 (2010).
- 4.Ancochea, J. et al. Underdiagnosis of chronic obstructive pulmonary disease in women: quantification of the problem, determinants and proposed actions. Arch. Bronconeumol. 49, 223–229 (2013).
- 5.Chapman, K. R., Tashkin, D. P. & Pye, D. J. Gender bias in the diagnosis of COPD. Chest 119, 1691–1695 (2001).
- 6.World Health Organization. Available from: http://www.who.int/en/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (2017). Accessed 29 Nov 2018.
- 7.Afonso, A. S., Verhamme, K. M., Sturkenboom, M. C. & Brusselle, G. G. COPD in the general population: prevalence, incidence and survival. Respir. Med. 105, 1872–1884 (2011).
- 8.Bischoff, E. W. et al. Trends in COPD prevalence and exacerbation rates in Dutch primary care. Br. J. Gen. Pract. 59, 927–933 (2009).
- 9.Rycroft, C. E., Heyes, A., Lanza, L. & Becker, K. Epidemiology of chronic obstructive pulmonary disease: a literature review. Int. J. Chron. Obstruct. Pulmon. Dis. 7, 457–494 (2012).
- 10.Tsiligianni, I., Rodriguez, M. R., Lisspers, K., LeeTan, T. & Infantino, A. Call to action: improving primary care for women with COPD. NPJ Prim. Care Respir. Med. 27, 11 (2017).
- 11.Waatevik, M. et al. Increased prevalence of chronic obstructive pulmonary disease in a general population. Respir. Med. 107, 1037–1045 (2013).
- 12.Mamary, A. J. et al. Race and gender disparities are evident in COPD underdiagnoses across all severities of measured airflow obstruction. Chronic Obstr. Pulm. Dis. 5, 177–184 (2018).
- 13.Stallberg, B. et al. Management, morbidity and mortality of COPD during an 11-year period: an observational retrospective epidemiological register study in Sweden (PATHOS). Prim. Care Respir. J. 23, 38–45 (2014).
- 14.Agusti, A. et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir. Res. 11, 122 (2010).
- 15.Carrasco-Garrido, P. et al. Characteristics of chronic obstructive pulmonary disease in Spain from a gender perspective. BMC Pulm. Med. 9, 2 (2009).
- 16.Di Marco, F. et al. Anxiety and depression in COPD patients: The roles of gender and disease severity. Respir. Med. 100, 1767–1774 (2006).
- 17.Ferrari, R. et al. Gender differences in predictors of health status in patients with COPD. J. Bras. Pneumol. 36, 37–43 (2010).
- 18.Martinez, F. J. et al. Sex differences in severe pulmonary emphysema. Am. J. Respir. Crit. Care Med. 176, 243–252 (2007).
- 19.Naberan, K., Azpeitia, A., Cantoni, J. & Miravitlles, M. Impairment of quality of life in women with chronic obstructive pulmonary disease. Respir. Med. 106, 367–373 (2012).
- 20.Folkhalsomyndigheten. Available from: https://www.folkhalsomyndigheten.se/folkhalsorapportering-statistik/folkhalsans-utveckling/levnadsvanor/tobaksrokning-daglig/ (2018). Accessed 29 Nov 2018.
- 21.de Torres, J. P. et al. Gender and COPD in patients attending a pulmonary clinic. Chest 128, 2012–2016 (2005).
- 22.Sorheim, I. C. et al. Gender differences in COPD: are women more susceptible to smoking effects than men? Thorax 65, 480–485 (2010).



{kind=link}