













 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The organ of balance in the inner ear is surrounded by the hardest bone in the body. Using synchrotron X-rays, researchers at Uppsala University have discovered a drainage system that may be assumed to play a major role in the onset of Ménière’s disease, a common and troublesome disorder. These results are published in the journal Scientific Reports.
Ménière’s disease is manifested in sudden onset of severe dizziness (vertigo) attacks, hearing impairment and tinnitus.
Accumulation of excess fluid in the inner ear is thought to cause the disorder, from which approximately an estimated 30,000 people in Sweden suffer.
The researchers behind the new scientific article have investigated the organs in the human inner ear, which are very difficult to study. This part of the ear is enclosed by the body’s hardest bone.
Using synchrotron X-ray imaging, an advanced and powerful form of computer tomography (CT), the scientists were able to study the organ of balance with its surrounding blood vessels.
Since the technology generates energy too high for use on living humans, donors’ temporal bones were used.
The images of the inner ear were reconstructed to make a three-dimensional model in the software, Inside the hard bone, the researchers discovered a drainage system that is thought to explain how the fluid in the inner ear is absorbed.
This discovery may bring about an improved understanding of how and why Ménière’s disease arises.
The synchrotron imaging investigation was carried out in Saskatoon, in the Canadian province of Saskatchewan. The study was conducted jointly with Dr. Sumit Agrawal and Dr. Hanif Ladak, who are researchers in London, Ontario (Canada).
Micro-computed tomography (Micro-CT)
Micro-CT and 3D modelling identified the VA and its accessory canals; however, the soft tissue matter could not be reproduced. Simulated 3D “castings” of the labyrinth were created by a contrast enhancement technique between boundaries.
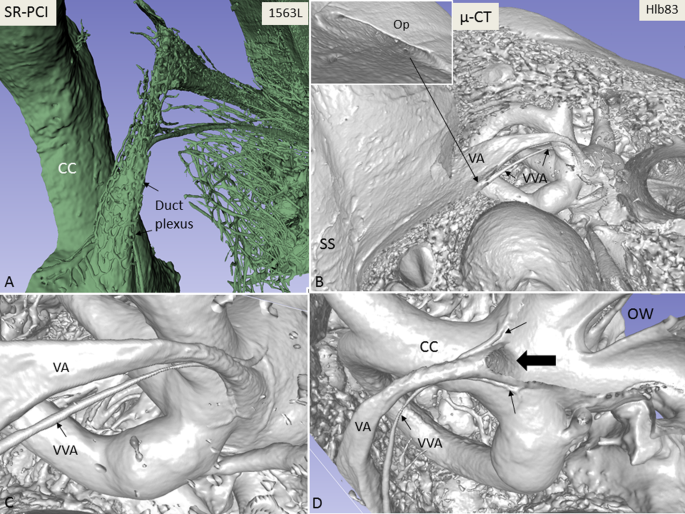
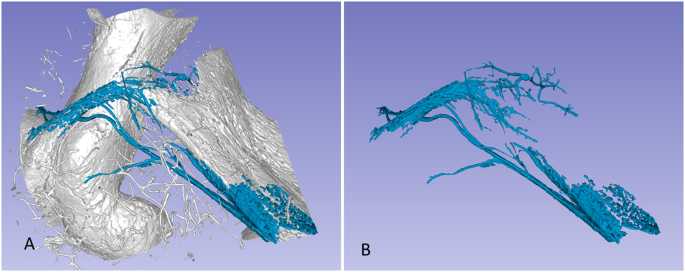
A comparison between SR-PCI and micro-CT reproduction of the VA is shown in Fig. 1. While the bony VA and VVA were well visualised on micro-CT and SR-PCI (Fig. 1B–D), the channel plexus around the ED was only seen in SR-PCI (Fig. 1A).
Bone transparency and cropping visualised the 3D bony outline. Extensive variations were noted in the VA and accessory canal anatomy. In general, two to three venous bone channels were observed at the internal aperture of the VA (Fig. 1D).
These channels merged into the VVA channel that opened into the floor of the extra-osseous part of the ES (Fig. 1B, inset). The location of the opening of the accessory channel varied greatly but was mostly located at the inferior–medial aspect of the VA.
The mean volume of the VA, measured from the internal aperture to the isthmus, was 0.32 µL (range, 0.24–0.43 µL). No difference was detected in the resolution of the tissue between macerated and freshly fixed bones.
Synchrotron radiation phase-contrast imaging (SR-PCI)
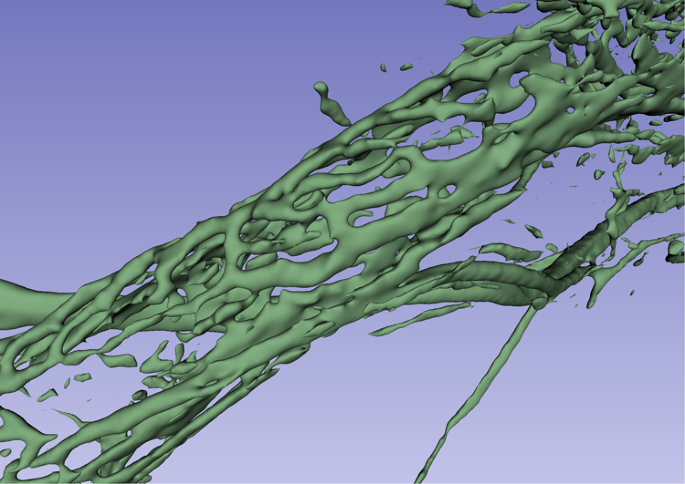
SR-PCI and 3D reconstructions of the temporal bones revealed a rich plexus of channels around the VA (Figs. 2 and 3). This was done by making the bone transparent with a scalar opacity mapping tool. This technique enhanced the surface density differences and increased the contrast to visualise small bone channels.
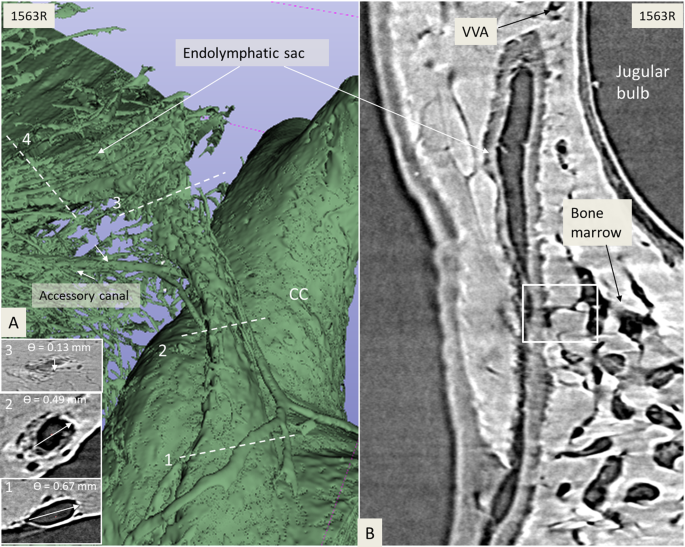
The ES epithelium and sub-epithelial connective tissue were visualised on X-ray sections. Vessels were sometimes reproduced inside the bone channels. The plexus was located in the bony rim of the VA and was connected to vessels around the ED.
Channels were sinusoid-like; they developed proximally and emptied distally into the collecting channels leading to the VVA near the isthmus portion of the VA.
The VVA further drained into the sigmoid sinus or jugular bulb. Several channels were typically connected at the distal ED with the accessory canal. Occasionally, the channels were connected to the proximal ES. The VVA was mostly derived from two uniting veins, namely the anterior and posterior branches, as described by Nabeya(Nabeya, D. A study in the comparative anatomy of the blood-vascular system of the internal ear in Mammalia and Homo. Acta Scholae Medicinalis, Kyoto University 6, 1–132 (1923).).
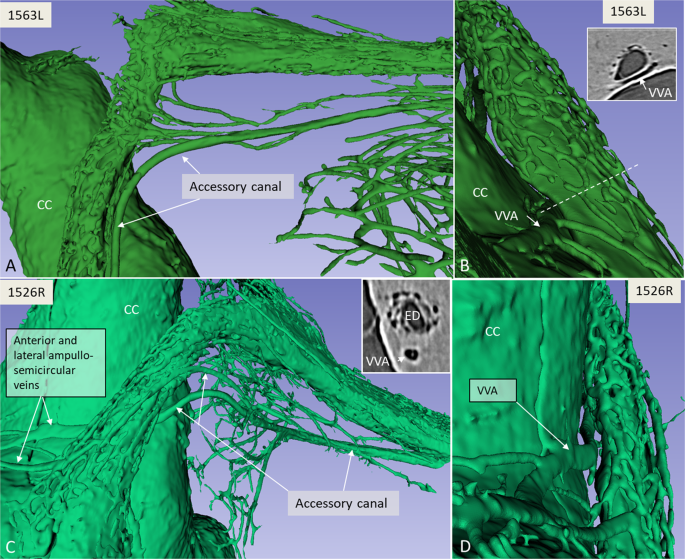
The anterior branch was the largest, with twigs from the anterior and lateral ampullo-semicircular and common crus (CC) branches. The posterior branch was derived from the posterior ampullo-semicircular branch and approximated the VA inferiorly.
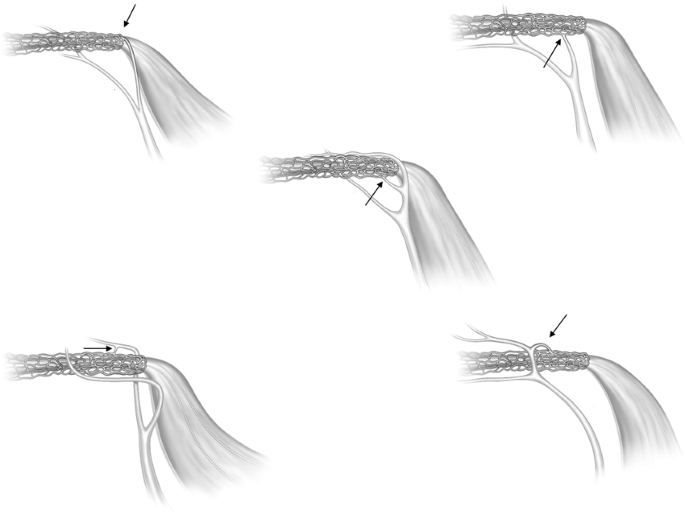
According to Nabeya(Nabeya, D. A study in the comparative anatomy of the blood-vascular system of the internal ear in Mammalia and Homo. Acta Scholae Medicinalis, Kyoto University 6, 1–132 (1923).), the VVA receives branches from all semicircular canals and a part of the vestibule. The VVA anatomy differed depending on the vestibular venous anatomy. Occasionally, the anterior and lateral branches united and ran on the lateral side between the VA and CC.
In other specimens the anterior ampullo-semicircular branch ran on the lateral sides of the VA and united with the VVA. The veins sometimes surrounded the VVA on both sides. Various types of anatomy are displayed in Fig. 4.
The plexus was not a portal system derived from the VVA but arose locally around the proximal ED and emptied distally into the VVA. In one specimen the channel system was manually modelled (Figs. 5 and 6). Here, branches of the plexus also surrounded the proximal and distal portions of the ES; however, in all cases, the plexus was more developed around the ED. Occasionally channels were interconnected with surrounding bone marrow spaces at the ES.
The ED, at its narrowest point (isthmus), measured 0.18 mm (range, 0.14–0.26 mm), and at the internal aperture, the longest distance was 0.76 mm (range, 0.54–0.88 mm) and the shortest distance was 0.35 mm (range, 0.26–0.54 mm). The diameters of the VVA branches were measured as close to the ED as possible; branch 1 measured 0.08 mm (range, 0.05–0.13 mm) and branch 2 measured 0.07 mm (range, 0.05–0.10 mm) (Table 1).
Table 1 Dimensions of the VA and VVA (Measurements in mm).
| Specimen | VA Diameter* | VA Diameter** Long | VA Diameter** Short | Diameter of Branch 1 of the VVA | Diameter of Branch 2 of the VVA |
|---|---|---|---|---|---|
| 2R | 0.26 | 0.81 | 0.37 | 0.11 | 0.10 |
| 1526R | 0.17 | 0.75 | 0.30 | 0.13 | 0.05 |
| 1563L | 0.18 | 0.54 | 0.26 | 0.06 | 0.07 |
| 1563R | 0.14 | 0.83 | 0.30 | 0.06 | 0.09 |
| 1571X | 0.16 | 0.88 | 0.54 | 0.05 | 0.05 |
| Mean | 0.18 | 0.76 | 0.35 | 0.08 | 0.07 |
| SD | 0.04 | 0.12 | 0.10 | 0.03 | 0.02 |
- *Diameter of the narrowest part of the VA (isthmus). **Diameter at internal aperture of the VA, shortest and longest distances. The branches 1 and 2 of the VVA were measured at a point nearest the VA. VA; vestibular aqueduct. VVA; vein of the vestibular aqueduct.
More information: Charlotta Kämpfe Nordström et al, A Micro-CT and Synchrotron Imaging Study of the Human Endolymphatic Duct with Special Reference to Endolymph Outflow and Meniere’s Disease, Scientific Reports (2020). DOI: 10.1038/s41598-020-65110-0



{kind=link}