











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



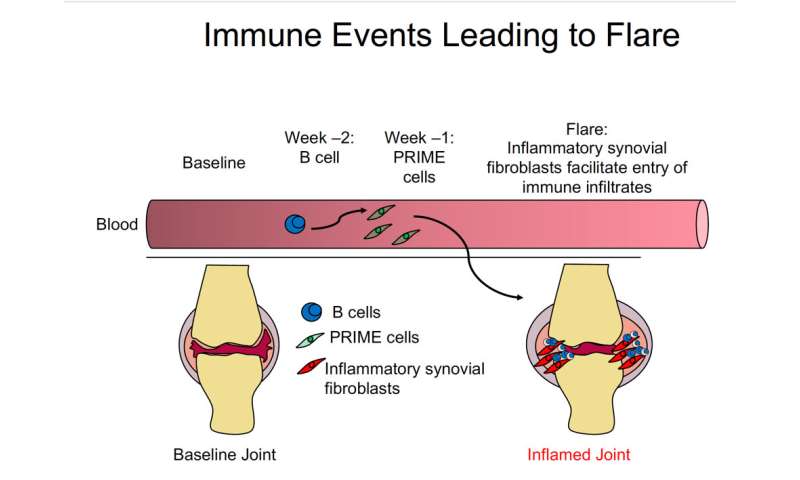
AThe cells, dubbed “PRIME cells,” accumulate in the blood during the week prior to disease flare-ups, Howard Hughes Medical Institute Investigator Robert Darnell’s team reports July 15, 2020, in the New England Journal of Medicine.
The findings could lead to better prediction of when severe pain and swelling, called “flares” will occur, as well as provide new avenues for treatment.
“PRIME cells are one thing you might want to target to arrest the flare before it happens,” Darnell says. “That’s the ideal of medical science – to know enough about a disease that you can put your finger on what’s about to make someone sick.”
Rheumatoid arthritis is a disease of the immune system that causes inflammation in the joints, especially around the hands and feet. It can be debilitating and frequently strikes people in their 30s or 40s.
The symptoms come in waves, with stretches of relative quiet interspersed with painful flares. Current therapeutics, chiefly steroids, can treat these symptoms, but there’s no cure.
To study this sort of disease, where symptoms vary dramatically from week to week, it’s critical to track changes in the body over an extended time. But it’s hard for patients to trek to a clinic for frequent testing.
So Darnell, a neuro-oncologist at Rockefeller University, and his colleagues developed an at-home blood collection system. Patients with rheumatoid arthritis did simple finger sticks and sent their blood to his lab. Each participant also kept a record of symptoms to identify when flares occurred.
Armed with these records, the researchers tested the blood samples, looking for molecular changes preceding the onset of symptoms. By analyzing the RNA of cells in the bloodstream, Darnell’s team could identify which types of cells were present during symptom-free times and in the weeks preceding a flare.
In samples collected two weeks prior to a flare, researchers saw an increase in immune cells called B cells. That’s not surprising, Darnell says – researchers already knew these cells attacked patients’ joints in rheumatoid arthritis.
But in samples collected one week before a flare, his team noticed something odd. They saw an increase in RNA that didn’t match the genetic signature of any known type of blood or immune cell.
“That got us thinking there was something fishy going on,” says study coauthor Dana Orange, a rheumatologist at Rockefeller. The RNA signature instead resembled that of bone, cartilage, or muscle cells – cells not typically found in the blood.
Darnell’s team called the newfound cell type a PRIME cell, for “pre-inflammation mesenchymal” cell. (Mesenchymal cells are a type of stem cell that can develop into bone or cartilage.)
In the patients, PRIME cells accumulated in the bloodstream a week before the flare but disappeared during the flare. This observation, combined with previous work from another lab in mice, suggests a possible role for PRIME cells in rheumatoid arthritis flares, Darnell says.
One of the team’s next steps is to test in more patients whether the presence of these cells can predict a flare, Darnell says.
The researchers are still recruiting patients for this study; currently the team’s blood collection system is only available for use in research. Darnell also wants to study PRIME cells’ molecular characteristics.
If the cells do indeed take part in causing flares, he says, “understanding the unique aspects of PRIME cells might enable us to target them with a drug and get rid of them.”
Etiology
Inflammatory arthritis includes infectious arthritis, crystal-induced, immune-related arthritis and reactive arthritis. Organisms causing infectious arthritis include Staphylococcus aureus, Streptococcal pneumoniae, Neisseria gonorrheoae, anaerobic bacteria, mycobacterial species, brucellosis, Borrelia burgdorferi, sporotrichosis, coccidioidomycosis, viruses (Parvovirus, Enterovirus, and Rubella).
The causative organism varies by age and geographic location. Septic arthritis is usually monomicrobial. Polymicrobial infections are usually less common and occur in the setting of penetrating trauma involving joint space. Septic arthritis due to gram-negative bacteria is observed in the setting of trauma or intravenous drug abuse. [3][4]
Crystal-induced arthritis includes gout and pseudo-gout. Deposited monosodium urate crystals in the joint space cause gout. Hyperuricemia is a predisposing factor of gout, but most of the hyperuricemic individuals never develop gout. Multiple factors play a role in the deposition of the crystal in joint and subsequent inflammation.
It can be caused by the absolute or relative impairment of renal uric acid secretion, overproduction of uric acid and overconsumption of purine-rich foods. Risk factors linked to the development of gout include male gender, obesity, alcohol, thiazide or loop diuretics, chronic kidney disease.
Pseudo-gout is due to the deposition of calcium pyrophosphate crystal deposition causing an inflammatory response. Most of the cases of CPPD crystal deposition are idiopathic, but joint trauma, familial chondrocalcinosis, hemochromatosis can be associated with the illness.
Immune-related arthritis includes arthritis due to rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, polymyositis, Sjogren syndrome, and systemic sclerosis. Reactive arthritis is usually seen after or during an infection elsewhere in the body after which micro-organisms cannot be recovered from the joint. A specific list of gastrointestinal (GI) and urogenital pathogens could be considered causative which includes Chlamydia trachomatis, Yersinia, Salmonella, Shigella, and Campylobacter.[5]
Pathophysiology
Inflammatory arthritis is characterized by an influx of inflammatory cells such as macrophages, lymphocytes, and granulocytes from the bloodstream into the synovial membrane and is associated with hyperplasia of synovial fibroblasts. In some cases, damage to the cartilage and bone can cause joint destruction.
The virus may directly invade the joint resulting in the infection of the synovium or the joint tissues. Rubella, Parvovirus, and enteroviruses utilize this mechanism. Viral particles may act as the antigenic component of immune complexes formed by the humoral response to the viral infection.
These immune complexes may accumulate in the joints and skin leading to arthritis, arthralgia, and skin rash. This type of presentation is seen mostly in hepatitis B, hepatitis C, and Parvovirus.[9][10][11]
Rheumatoid arthritis (RA) is a combination of pre-determined genetic and environmental factors. Susceptibility to RA is mostly defined by a pattern of inherited genes with human leucocyte antigen (HLA) and major histocompatibility (MHC) genes as the most important.
Environmental factors include smoking which can interact with the genes to increase susceptibility to 20 fold. The mechanism is the repeated activation of the immune system until some unknown process directs the balance towards clinically apparent disease. Smoking induces peptide arginine deiminase expression in alveolar macrophages.
These enzymes convert arginine to citrulline in the airway causing neoantigens that can be recognized by the adaptive immune system. Increased immune reactivity to the neoepitopes created by protein and protein citrullination and anti-citrullinated protein antibodies is unique to rheumatoid arthritis.
Once the inflammatory process is fully established the synovium is RA organizes itself into an invasive tissue that can degrade cartilage and bone.
The initiation of the acute inflammatory process in gout is the deposition of monosodium crystals in the joint which produces more inflammation. Binding of immunoglobulin to the MSU crystals results in increased release of super-oxide and lysosomal enzymes from the neutrophils accelerating the inflammatory cascade.
History and Physical
With a good history and proper physical examination, clinicians can reach a diagnosis. The duration of symptoms, the extent of joint involvement, and the patient’s age narrow the differentials to reach a diagnosis.
Systemic lupus erythematosus (SLE) and reactive arthritis occur more frequently in the young; whereas, RA is more frequent in middle age. Gout, spondyloarthritis, and ankylosing spondylitis are more common in men than in women; whereas, RA and lupus are more frequent in women than in men.
Racial predilections may be evident as well. Polymyalgia rheumatica commonly affect whites; whereas, sarcoidosis and SLE more commonly affect African Americans. Familial aggregation is most common with ankylosing spondylitis and gout.
The patients’ complaints may evolve differently and can be classified as chronic (RA), intermittent (crystal or Lyme arthritis), or migratory (rheumatic fever, gonococcal, or viral arthritis). The upper extremities are frequently involved in RA and OA; whereas, lower extremity arthritis is characteristic of reactive arthritis and gout at their onset.
Involvement of the axial skeleton is common in ankylosing spondylitis but is infrequent in RA, with the notable exception of the cervical spine. Presence of precipitating factors also help to narrow down the diagnosis; antecedent infection is often seen in reactive arthritis, renal insufficiency and use of drugs (steroids and diuretics) are associated with gout.
Evaluation
Inflammatory arthritis is accompanied by elevated ESR and CRP, thrombocytosis, anemia of chronic disease. Duration of stiffness is prolonged in inflammatory arthritis, and the stiffness improves with activity.
By contrast, in noninflammatory conditions (such as osteoarthritis [OA]), stiffness is shorter in duration (less than 60 minutes), and exacerbated by activity; furthermore, inflammatory markers are absent.
When evaluating a patient with joint pain, clinicians should first find out whether the patient is having articular or nonarticular symptoms. If the complaints are articular, find out the duration. If it has been for less than 6 weeks, it is classified as acute and includes infectious, gout and pseudo-gout.
If the symptoms have lasted for more than 6 weeks, they are classified as chronic. Clinicians classify it as oligo-arthritis if there are less than 3 joints involved and polyarthritis with more than 3 joints involved.
Arthrocentesis should be performed in affected swollen joints to exclude diagnosis including infectious or crystal-induced arthritis. Testing includes complete blood cell (CBC) count, differential, Gram stain, culture, and crystal search. Imaging studies include plain radiograph. Erosions are typically seen in patients with rheumatoid arthritis.[1][12][13]
Septic arthritis usually presents as fever, single swollen painful joint. When there is suspected joint infection, synovial fluid aspiration should be done before antibiotics are administered.
Fluids should be sent for Gram stain and culture, leucocytes with differential, and assessment of crystals. Septic arthritis is characterized by polymorphonuclear lymphocytes greater than 20000 mm3 and inflammatory arthritis due to autoimmune and crystal deposition is characterized by polymorphonuclear lymphocytes of 2000 to 20,000 mm3.
Needle-shaped yellow crystals are seen in gouty arthritis, and rhomboid-shaped crystals are seen in pseudo-gout. If the cause mentioned above does not explain arthritis and the person meets the criteria for a typical autoimmune disease, then arthritis can be attributed to the autoimmune disease.
Elevation of rheumatoid factor and anti-citrullinated protein antibody, elevated ESR and CRP are consistent with the diagnosis of rheumatoid arthritis. Patients with inflammatory back symptoms, a history of inflammatory bowel disease, or inflammatory eye disease may have spondyloarthropathy. Persons with less than 6 weeks of symptoms may have a viral process such as Parvovirus.
Treatment / Management
Inflammation is generally reversible, while joint destruction is not. Early and appropriate treatment before a definitive diagnosis may prevent disease persistence, joint damage, and disability.
The goal of therapy is the suppression of inflammation and prevention of recurrent inflammation and joint damage. In patients with undifferentiated arthritis such as RA, clinicians use a multidisciplinary management approach that includes patient education, physical and occupational therapy, and pharmacological therapy.
Surgical measures are rarely needed in the early stage of arthritis. Once the patient has evolved from UA to a specific diagnosis that usually occurs within a year or less of presentation, we recommend treatment for the patient’s specific disorder.
Initial drug therapy of patients with UA should follow pretreatment screening which includes baseline routine laboratory testing (CBC, liver and renal chemistries, acute phase reactants), screening for hepatitis B and C and latent tuberculosis.
A baseline chest x-ray should be obtained before starting methotrexate therapy. Combination therapy with 2 or more DMARDs is more effective than monotherapy, but the adverse effects may also be greater. If symptoms are not well controlled with a nonbiologic DMARD, a biologic DMARD should be added.
Tumor necrosis factor (TNF) inhibitors are first-line biologic therapy. If TNF inhibitors are ineffective, additional biologic therapies can be considered, for example, adalimumab. Concurrent use of more than one biologic therapy is not recommended because of an unacceptable rate of adverse effects.
The initial therapeutic goal is to achieve significant clinical improvement within 3 months which may be defined as at least a 50% reduction in disease activity. [7][14][15]
In the patients with upper extremity involvement, or in those who have a positive test for RF, treatment with methotrexate rather than DMARDs is recommended. While in the patients with UA who lack RA and have involvement primarily in lower extremities, treatment with DMARDs is suggested.
Treatment of patients who are resistant to initial therapy at 3 months or do not achieve remission or low disease activity after 6 months, combination therapy is preferred. Anti-inflammatory therapies including systemic and intraarticular steroids are used for temporary control of disease in patients who start treatment with DMARDs
Prognosis
Prognosis depends on the cause of arthritis. Several studies have shown that 17% to 32% of the patients progress to rheumatoid arthritis, while 40% to 55% achieve spontaneous remission.
In a study with a 2-year follow up of undifferentiated arthritis, a diagnosis of RA was made in 30% during the follow-up period, arthritis resolved in 41%, and 10% were lost to follow up. In another study, spontaneous remission of arthritis was rare once symptoms exceeded 8 weeks in duration.
The so-called “window of opportunity theory” hypothesis that in an early stage of UA, a period may exist in which the disease course can be altered by the appropriate treatment, preventing it from being a chronic and disabling disease.
The course of reactive arthritis depends on the triggering pathogen and the genetic background of the host. The typical disease duration is 3 to 5 months. Most of the patients have complete remission or have little active disease within 6 to 12 months after presentation, but 15% to 20% may experience chronic persistent arthritis.
Human leukocyte antigen B27 (HLA-B27) testing has been associated with a worse prognosis in some, but not all. An HLA-B27-positive patient is more likely to develop a chronic spondyloarthropathy with radiographic changes. Patients with a triad of post-infectious arthritis, urethritis, and conjunctivitis may also have a poorer prognosis.
References
1.Krenn V, Waldstein W, Najm A, Perino G, Gaulke R. [Histopathological classification principles of rheumatic joint diseases : Contribution of pathology to the diagnosis]. Orthopade. 2018 Nov;47(11):941-948. [PubMed]
2.Berman S, Bucher J, Koyfman A, Long BJ. Emergent Complications of Rheumatoid Arthritis. J Emerg Med. 2018 Nov;55(5):647-658. [PubMed]
3.Kłodziński Ł, Wisłowska M. Comorbidities in rheumatic arthritis. Reumatologia. 2018;56(4):228-233. [PMC free article] [PubMed]
4.Powell AP, English J. Exercise for Athletes With Inflammatory Arthritis. Curr Sports Med Rep. 2018 Sep;17(9):302-307. [PubMed]
5.Premkumar A, Morse K, Levack AE, Bostrom MP, Carli AV. Periprosthetic Joint Infection in Patients with Inflammatory Joint Disease: Prevention and Diagnosis. Curr Rheumatol Rep. 2018 Sep 10;20(11):68. [PMC free article] [PubMed]
6.Sewerin P, Brinks R, Schneider M, Haase I, Vordenbäumen S. Prevalence and incidence of psoriasis and psoriatic arthritis. Ann. Rheum. Dis. 2019 Feb;78(2):286-287. [PubMed]
7.Holroyd CR, Seth R, Bukhari M, Malaviya A, Holmes C, Curtis E, Chan C, Yusuf MA, Litwic A, Smolen S, Topliffe J, Bennett S, Humphreys J, Green M, Ledingham J. The British Society for Rheumatology biologic DMARD safety guidelines in inflammatory arthritis. Rheumatology (Oxford). 2019 Feb 01;58(2):372. [PubMed]
8.Tuncer T, Gilgil E, Kaçar C, Kurtaiş Y, Kutlay Ş, Bütün B, Yalçin P, Akarirmak Ü, Altan L, Ardiç F, Ardiçoğlu Ö, Altay Z, Cantürk F, Cerrahoğlu L, Çevik R, Demir H, Durmaz B, Dursun N, Duruöz T, Erdoğan C, Evcik D, Gürsoy S, Hizmetli S, Kaptanoğlu E, Kayhan Ö, Kirnap M, Kokino S, Kozanoğlu E, Kuran B, Nas K, Öncel S, Sindel D, Orkun S, Sarpel T, Savaş S, Şendur ÖF, Şenel K, Uğurlu H, Uzunca K, Tekeoğlu İ, Guillemin F. Prevalence of Rheumatoid Arthritis and Spondyloarthritis in Turkey: A Nationwide Study. Arch Rheumatol. 2018 Jun;33(2):128-136. [PMC free article] [PubMed]
9.Miyoshi M, Liu S. Collagen-Induced Arthritis Models. Methods Mol. Biol. 2018;1868:3-7. [PubMed]
10.Nguyen CT, Bloch Y, Składanowska K, Savvides SN, Adamopoulos IE. Pathophysiology and inhibition of IL-23 signaling in psoriatic arthritis: A molecular insight. Clin. Immunol. 2019 Sep;206:15-22. [PMC free article] [PubMed]
11.Ruiz L, López P, Suárez A, Sánchez B, Margolles A. The role of gut microbiota in lupus: what we know in 2018? Expert Rev Clin Immunol. 2018 Oct;14(10):787-792. [PubMed]
12.Bakker PAC, Ramiro S, Ez-Zaitouni Z, van Lunteren M, Berg IJ, Landewé R, Ramonda R, van Oosterhout M, Reijnierse M, van Gaalen FA, van der Heijde D. Is it Useful to Repeat Magnetic Resonance Imaging of the Sacroiliac Joints After Three Months or One Year in the Diagnosis of Patients With Chronic Back Pain and Suspected Axial Spondyloarthritis? Arthritis & rheumatology (Hoboken, N.J.). 2019 Mar;71(3):382-391. [PMC free article] [PubMed]
13.Ventura-Ríos L, Faugier E, Barzola L, De la Cruz-Becerra LB, Sánchez-Bringas G, García AR, Maldonado R, Roth J, Hernández-Díaz C. Reliability of ultrasonography to detect inflammatory lesions and structural damage in juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2018 Sep 17;16(1):58. [PMC free article] [PubMed]
14.Duruöz MT, Ünal Ç, Ulutatar F, Sanal Toprak C, Gündüz OH. The Validity and Reliability of Turkish Version of the Jenkins Sleep Evaluation Scale in Rheumatoid Arthritis. Arch Rheumatol. 2018 Jun;33(2):160-167. [PMC free article] [PubMed]
15.Zerbini CAF, Abud-Mendoza C, Mendez-Patarroyo P, De Angelo Andrade M, Pedersen R, Vlahos B, Borlenghi CE. Maintenance of low disease activity and remission with etanercept-disease-modifying antirheumatic drug (DMARD) combination therapy compared with treatment with DMARDs alone in Latin American patients with active rheumatoid arthritis: Subset analysis of a randomized trial. Medicine (Baltimore). 2018 Sep;97(36):e11989. [PMC free article] [PubMed]
16.Kloppenburg M, Kroon FP, Blanco FJ, Doherty M, Dziedzic KS, Greibrokk E, Haugen IK, Herrero-Beaumont G, Jonsson H, Kjeken I, Maheu E, Ramonda R, Ritt MJ, Smeets W, Smolen JS, Stamm TA, Szekanecz Z, Wittoek R, Carmona L. 2018 update of the EULAR recommendations for the management of hand osteoarthritis. Ann. Rheum. Dis. 2019 Jan;78(1):16-24. [PubMed]
17.Sanz Sanz J, Beltrán E, Díaz-Miguel Pérez MC, Fernández-Carballido C, Galíndez E, García Porrua C, Gratacós J, Medina J, Queiro R, Ramírez J, Reina D, Rodríguez Lozano C, Rodríguez Martínez FJ, Rubio E, Veroz R. Quality standard for the management of patients with psoriatic arthritis: QUANTUM Project. Reumatol Clin. 2020 May – Jun;16(3):203-215. [PubMed]
18.Muñoz-Fernández S, Otón-Sánchez T, Carmona L, Calvo-Alén J, Escudero A, Narváez J, Rodríguez Heredia JM, Romero Yuste S, Vela P, Luján Valdés S, Royo García A, Baquero JL. Use of prognostic factors of rheumatoid arthritis in clinical practice and perception of their predictive capacity before and after exposure to evidence. Rheumatol. Int. 2018 Dec;38(12):2289-2296. [PubMed]
19.Mouyis M, Flint JD, Giles IP. Safety of anti-rheumatic drugs in men trying to conceive: A systematic review and analysis of published evidence. Semin. Arthritis Rheum. 2019 Apr;48(5):911-920. [PubMed]
More information: Dana E. Orange et al. “RNA Identification of PRIME Cells Predicting Rheumatoid Arthritis Flares,” New England Journal of Medicine. Published online July 15, 2020. DOI: 10.1056/NEJMoa2004114



{kind=link}