









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A study by scientists from the University of Southampton has examined the chances of catching COVID-19 in a train carriage carrying an infectious person.
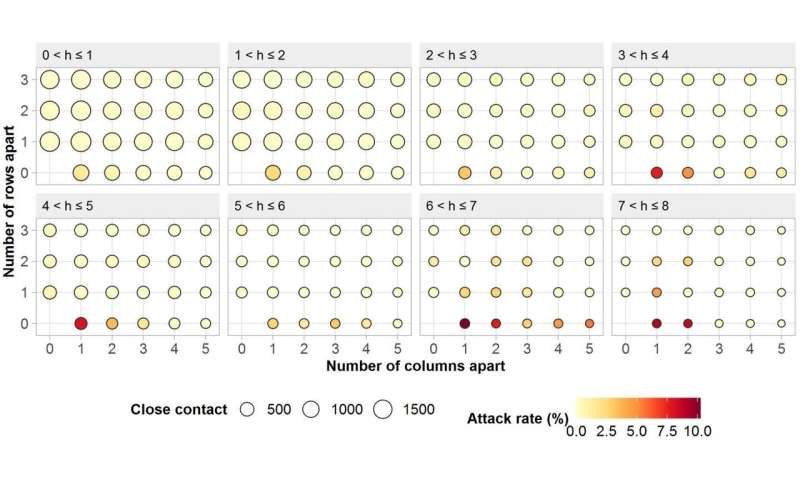
Based on high-speed routes in China, researchers from WorldPop found that for train passengers sitting within three rows (widthwise) and five columns (lengthwise) of an infected person (index patient) between zero and ten percent (10.3) caught the disease.
The average rate of transmission for these ‘close contact’ travelers was 0.32 percent.
The study, in collaboration with the Chinese Academy of Sciences, China Academy of Electronics and Information Technology, and Chinese Centre for Disease Control and Prevention, also showed that passengers traveling in seats directly adjacent to an index patient suffered the highest level of transmission, with an average of 3.5 percent contracting the disease. For those sitting on the same row, the figure was 1.5 percent.
The ‘attack rate’ for each seat – the number of passengers in a given seat diagnosed with COVID-19, divided by the total number of passengers traveling in the same seat – increased by 0.15 percent for every hour that a person traveled with an index patient.
For those in adjacent seats, this rate of increase was higher at 1.3 percent per hour.
Interestingly, the researchers found that only 0.075 percent of people who used a seat previously occupied by an index patient went on to contract the disease.
Details are published in the journal Clinical Infectious Diseases.
The WorldPop team, experts in population mapping, used sophisticated modeling to analyze anonymised itinerary and infection data relating to train passengers on China’s high-speed G train network.
This included those who had COVID-19 at the time of travel and their close contacts (who showed symptoms within 14 days of travel).
The data, covering a period between 19 December 2019 and 6 March 2020, included 2,334 index patients and 72,093 close contacts.
Their travel times ranged from between less than an hour to eight hours.
Lead investigator, Dr. Shengjie Lai, comments, “Our study shows that although there is an increased risk of COVID-19 transmission on trains, a person’s seat location and travel time in relation to an infectious person can make a big difference as to whether it is passed on.
The findings suggest that during the COVID-19 epidemic it is important to reduce the density of passengers and promote personal hygiene measures, the use of face coverings and possibly carry-out temperature checks before boarding.”
The researchers conclude that given the attack rates estimated for passengers in the same row as an index patient, a safe social distance of more than one meter is required for one hour spent traveling together.
After two hours of contact, they consider a distance of less than 2.5 meters may be insufficient to prevent transmission.
Director of WorldPop, Professor Andy Tatem adds: “Our research is the first to quantify the individual risk of COVID-19 transmission on public transport based on data from epidemiological investigations of disease cases and their close contacts on high-speed trains.
“It shows that the transmission risk not only relates to the distance from an infected person, but also the time in their presence.
We hope it can help to inform authorities globally about measures needed to guard against the virus and in-turn help to reduce its spread.”
Infectious agents may spread from their natural reservoir to a susceptible host in different pathways. There are various classifications reported in the literature for modes of transmission of different infectious agents.
Morawska (2006) has presented a classification for virus transmission, including human-human transmission, airborne transmission, and other means of transmission such as endogenous infection, common vehicle, and vector spread.
However, many respiratory viruses are believed to transmit over multiple routes, of which droplet and aerosol transmission paths become paramount, but their significance in transmitting the disease remains unclear (Morawska and Cao, 2020; Shiu et al., 2019).
In general, infected people spread viral particles whenever they talk, breathe, cough, or sneeze. Such viral particles are known to be encapsulated in globs of mucus, saliva, and water, and the fate/behavior of globs in the environment depends on the size of the globs.
Bigger globs fall faster than they evaporate so that they splash down nearby in the form of droplets (Grayson et al., 2016; Liu et al., 2016).
Smaller globs evaporate faster in the form of aerosols, and linger in the air, and drift farther away than the droplets do.
Respiratory particles may often be distinguished to be droplets or aerosols based on the particle size and specifically in terms of the aerodynamic diameter (Hinds, 1999).
One could dispute that, unlike larger droplets, aerosols may pose a greater risk of the spread of the COVID-19 disease among many susceptible hosts positioned far from the point of origin.
Nevertheless, it has been proven that viral disease outbreaks via aerosol transmission are not as severe as one would think, because of dilution and inactivation of viruses that linger for extended periods in the air (Shiu et al., 2019).
There has been no discernible evidence on the minimum infectious viral load for COVID-19 pandemic, but many researchers speculate that a few hundreds of SARS-CoV-2 virus would be enough to cause the disease among susceptible hosts (Beggs, 2020; SMC, 2020).
There have been numerous disagreements on the average particle size of droplets and aerosols (Shiu et al., 2019). The World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) postulate that the particles of more than 5 μm as droplets, and those less than 5 μm as aerosols or droplet nuclei (Siegel et al., 2007; WHO, 2014).
Conversely, there have been some other postulations, indicating that aerodynamic diameter of 20 μm or 10 μm or less should be reckoned to be aerosols, based on their ability to linger in the air for a prolonged period, and the reachability to the respirable fraction of the lung (alveolar region) (Gralton et al., 2011; Nicas et al., 2005; Tellier, 2009).
Small aerosols are more susceptible to be inhaled deep into the lung, which causes infection in the alveolar tissues of the lower respiratory tract, while large droplets are trapped in the upper airways (Thomas, 2013).
For easy apprehension, aerosols can be defined as suspensions of solid or liquid particles in the air, which can be generated by either natural or anthropogenic phenomena (Judson and Munster, 2019; Tellier, 2009).
Though social distancing would be promising in combatting the COVID-19, the minimum distances that have been maintained between an infected person and a host are disputable and far from being established based on any scientific evidence. Nevertheless, many have believed that droplets predominate over aerosols in terms of contracting the disease; thus, over time, research work has been focused on acquiring better knowledge on the science of droplet transmission (Morawska and Cao, 2020; Wang and Du, 2020).
However, since the recent past, evidence has been provided to refute the former hypothesis and speculated that aerosols also play a major role in transmitting the disease (Morawska and Cao, 2020; Wang and Du, 2020).
As such, the controversy on the modes of transmission of the SARS-CoV-2 virus seems to be speculating and puzzled among many researchers, including the WHO (Morawska and Cao, 2020).
No conclusive studies have been conducted on differentiating between the modes of transmission of viruses via droplets and aerosols; hence, unresolved dichotomy.
It has also been argued that environmental settings, in which the SARS-CoV-2 virus transmits, trigger the disease adversely or beneficially with a susceptible host exposed to more or lesser payloads, respectively (Morawska, 2006; Tellier et al., 2019).
Such adverse or beneficial scenarios are based on plausible changes in the fate of the virus in the environment caused by altered transport phenomena. There have been myriads of hypotheses corroborating that certain threshold levels of humidity, temperature, sunlight, and ventilation will speed up the virus-laden droplet and aerosol transmission, aggravating the spread of the SARS-CoV disease (Morawska, 2006).
As scientists underpin more conclusive evidence on the modes of transmission via droplets and aerosols, facemasks and respirators worn by billions of people around the globe (both infected persons and susceptible hosts) become a common sight in day-to-day activities.
In the events of the droplet and aerosol transmission, the efficacy of such personal protective equipment in combating the transmission of the SARS-CoV-2 has been poorly understood.
Ever since the COVID-19 has been declared to be a pandemic with incredibly high morbidities and mortalities worldwide, the database of research on controlling the COVID-19, especially in the indoor environment, has been updated with several evidence-based studies.
However, less attention has been focused on the whole in controlling virus-laden droplet and aerosol shedding, their transport phenomena, and plausible methods of their dilution and destruction in different indoor settings.
With more COVID-19 cases reported worldwide, evidence-based decisions need to be adhered to in combating the disease, especially for situations in confined environments.
The transmission of droplets and aerosols within confined spaces becomes profoundly complex phenomena, and the real trajectories under different micro-climatic conditions are poorly understood.
The aggressive nature of the disease is directly connected with the transport phenomena of both droplets and aerosols, and the comprehension of such phenomena is vital in controlling the spread of the disease within such confined spaces.
Aerodynamic engineers, therefore, need to network with virologists to fully understand the possible trajectories of the viral spread within such confined spaces.
In this context, computational fluid dynamics could be made use of, to simulate the trajectories resulting from coughs and sneezes of an infected person within different confined settings.
This review paper is divided into two parts: Part 1 underpins the basic principles underlying the transmission via droplets and aerosols (Sections 2–5), and Part 2, being the common practices adopted by many in controlling the COVID-19 transmission with different masks worn in three confined settings; airplane, passenger car, and healthcare center (Section 6). Fig. 1 depicts an explicative schema of the two parts described in the following sections.

Part-1 enumerates the principles and findings on the transmission of virus-laden droplets and aerosols in literature, and Part-2 deliberates practices that are common in confined settings under different ventilation scenarios.
Size distribution, time taken, and distances transmitted by aerosols and droplets produced by infected people
The SARS-CoV-2 is often said to be transmitted through droplets generated when a symptomatic person coughs, sneezes, talks, or exhales (Morawska and Cao, 2020). Some of these droplets are too heavy to remain in the air, and rather fall on nearby floors or surfaces.
Fomites collect droplets contaminated with SARS-CoV-2, and touching of such surfaces by a susceptible host would get infected. However, some droplets, when ejected from an infected person, convert to aerosol particles (also known as bioaerosols) with relatively smaller aerodynamic diameters and, consequently, become airborne (Morawska, 2006).
Such virus-laden aerosol particles are capable of infecting people who inhale such particles, thereby spreading the disease. Further, there have been several transport phenomena where larger droplets become smaller through evaporation so that such smaller particles are called droplet nuclei.
Such aerosol particles with the encapsulation of viruses could be termed as bioaerosols or droplet nuclei; hence, the term ‘aerosol’, ‘bioaerosol’, and ‘droplet nuclei’ is used in this paper interchangeably.
The scenarios in respect of the generation of droplets and aerosol, particularly in the indoor environment, have not been adequately understood, and thus, insights into the plausible mechanisms are worthy of being explored.
Duguid (1945), for the first time, has explored the characteristics of droplets and aerosol from human expiratory activities with chest infections, and such information is presented in Table 1 .
Duguid (1945) has observed that 95% of particles were often smaller than 100 μm, and the majority were between 4 and 8 μm. The findings corroborated that breathing and exhalation originated from the nose have shed up to a few hundreds of droplets of which some were aerosols.
In contrast, talking, coughing, and sneezing have produced more aerosols than droplets (Table 1).
Table 1
Detailed information of droplets and aerosols generated from human expiratory activities (Source: Duguid, 1945).
| Activity | Number of droplets and aerosols generated (1–100 μm) | Presence of aerosols (1–2 μm) | Region of origin |
|---|---|---|---|
| Normal breathing (for 5 min) | None – few | Some | Nose |
| Single strong nasal expiration | Few – few hundred | Some | Nose |
| Counting loudly – talking | Few dozen – few hundred | Mostly | Front of the mouth |
| A single cough (mouth open) | None – few hundred | Some | Faucial region |
| A single cough (mouth initially closed) | Few hundred – many thousand | Mostly | Front of the mouth |
| Single sneeze | Few hundred thousand – few million | Mostly | Front of the mouth |
| Few – few thousand | Some | Both from the nose and the faucial region |
On the contrary to what Duguid (1945) has presented, a study conducted by Papineni and Rosenthal (1997) with five healthy individuals has manifested that 80–90% of particles from human expiratory activities were aerosols with the diameter being smaller than 1 μm.
The study also corroborated that the highest aerosol densities were generated during coughing and the lowest from nasal breathing, of which exhaled breath would be more responsible in transmitting the viruses (size of the order of 0.1 μm) when compared with transmitting the bacteria (> 1 μm).
It has been found that vomiting by a SARS-CoV infected person in the corridor of a hotel in Hong Kong in 2003 has contracted the disease on several people nearby by aerosol transmission (Morawska, 2006).
The physicochemical processes affecting the fate of airborne aerosols constitute evaporation, interaction with other types of particles, transport, and removal from the air by deposition on solid surfaces (Morawska, 2006).
Particles in the air are often subjected to Brownian motion, gravity, electrostatic forces, thermal gradients, electromagnetic radiation, turbulent diffusion, and inertial forces (Baron and Willeke, 2001).
Of these mechanisms, the diffusion is a key mechanism of transmitting viruses with particles in the lower sub-micrometer range, together with other aerosol particles (Baron and Willeke, 2001).
For droplets larger than 1 μm, gravity becomes significant than Brownian motion in deciding the fate of such particles (Cox, 1995). Under the standard atmospheric conditions, droplets smaller than 100 μm often evaporate before reaching the ground, and the evaporated droplet residues linger in the air for prolonged periods (Morawska, 2006).
When the droplets contain infectious bioaerosols, such as viruses, bioaerosols will remain in the air, even after the liquid content evaporates (Morawska, 2006).
However, the time interval that a virus survives in the air varies from one type of bioaerosol to another type. Droplets in the range of 0.5–20.0 μm lingering in the air are more likely to be retained in the respiratory tract and produce the infection (McCluskey et al., 1996).
However, droplets seem to be not present in the air for longer periods; instead, evaporation takes place, transforming droplets to bioaerosol residues, which could linger in the air for extended periods.
Hui and Chan (2010) have investigated that in different indoor environments, SARS-CoV could be transmitted through the airborne route.
Another retrospective study has found that the airborne transmission in an aircraft from an infected person to passengers located seven rows of seats ahead, indicating that the SARS-CoV virus could travel for a distance more than 1 m horizontally (Olsen et al., 2003).
Another case has been reported on infecting more than 1,000 persons in an apartment complex in Hong Kong because of aerosols generated by the building’s sewage system (McKinney et al., 2006).
These observations manifest that the aerosol-laden SARS-CoV virus transmission is a phenomenon, which would impart greater havoc than one thinks, and precautionary measures are, therefore, of paramount importance.
The SARS-CoV-2 virus has been found to remain viable in aerosols for 3 h, while it, in the form of droplets, is more stable on plastic and stainless steel, copper, cardboard, and glass with durations detected up to 72, 4, 24, and 84 h, respectively (van Doremalen et al., 2020).
In comparison, the SARS-CoV virus was also found to be airborne in the form of aerosols for 3 h, indicating that both SARS viruses behave more or less in the same manner in the air. Nevertheless, the SARS-CoV virus remains stable and viable in the form of droplets on plastic and stainless steel, copper, cardboard, and glass with durations (half-lives) lasting to 72, 8, 8, and 96 h, respectively (van Doremalen et al., 2020).
The half-lives of the SARS-CoV-2 and SARS-CoV are almost the same in aerosols, with median estimates of approximately 1.1–1.2 h, indicating that both viruses have similar stability characteristics in transmitting through the air (van Doremalen et al., 2020).
However, more profound epidemiological sustenance of SARS-CoV-2 virus may, therefore, be because of some other factors, including high viral loads in the upper respiratory tract and the capability of persons infected with COVID-19 to shed and transmit the virus while remaining asymptomatic (Bai et al., 2020; Zou et al., 2020).
Based on a study carried out by Nicas et al. (2005), it has been estimated that particles emitted from a cough of an infected person of a respiratory illness quickly decrease in diameter (with initial diameters of less than 20 μm) mainly because of the water loss by approximately half of the initial volume, amounting to 6 × 10−8 mL.
Exhaust ventilation, particle settling, die-off, and air disinfection methods are some prominent mechanisms by which the removal of viable airborne pathogens often takes place; each removal mechanism follows a first-order reduction rate (Nicas et al., 2005).
Based on 3-h viability of SARS-CoV-2 in the air (van Doremalen et al., 2020), prerequisites for the disease such as exposure, inhalation, and infection could occur minutes or a few hours later near and far from an aerosol source even in a stagnant environment (Bourouiba, 2020).
The actual airborne times for droplets may be greater in an environment where there are significant cross-flows (WHO, 2009). Such scenarios could be expected in quarantine and healthcare centers (e.g., with doors opening, bed and equipment movement, and people walking back and forth, constantly).
Conversely, airborne durations for smaller droplet nuclei or aerosols may be profoundly shorter when they are subject to a significant downdraft (e.g., if they pass under a ceiling supply vent) (WHO, 2009).
When the flow of mucus or saliva ejects from an infected person, its trajectory is determined primarily by the size of droplets and airflow patterns that govern the paths of movement (Tang et al., 2006).
The Stokes’ law describes the resultant trajectory of the droplets subjected to the forces of gravity downwards and air friction upwards, which governs the droplet movement in the air (Wells, 1934).
Coughs and sneezes usually constitute a turbulent cloud of buoyant gas with suspended droplets of various sizes. The larger droplets follow a ballistic trajectory irrespective of flow in the gas phase, whereas the aerosols are buoyant to a varying degree within the turbulent gas cloud (Bourouiba et al., 2014).
In general, there exists an accepted notion of a 2-m safe exclusion zone to prevent possible droplet transmission from an infected person to a susceptible host; however, there are no comprehensive studies to support such a phenomenon.
Wells (1934) has supported the 2-m exclusion zone concept taking into account the evaporation-falling curve. Wells (1934) has postulated that large droplets (> 100 μm) will fall to the floor within a horizontal distance of 2 m from the source.
Simple calculations, assumptions, and inadequate empirical data of Wells’s study have been later speculated by Xie et al. (2007). Xie et al. (2007) have corroborated that for respiratory exhalation flows, the larger droplets (diameter between 60 μm and 100 μm) were, depending on the exhalation air velocity and relative humidity of the air, carried away for more than 6 m of horizontal distance with the exhaled air having a velocity of 50 m/s at the point of expiration (Fig. 2 a).
Such scenarios simulate sneezing events. Conversely, larger droplets were found to carry for more than 2 m afar at a velocity of 10 m/s reordered at the point of exit, simulating coughing bouts (Fig. 2b).
The same for exhaling events for which the velocity is at 1 m/s was found to carry large droplets only up to about 1 m horizontally (Fig. 2c). Other studies also have proven that when an infected person of a respiratory illness coughs or sneezes, a cloud of pathogen-bearing droplets of different sizes appears to come out and travels even up to 7–8 m from the point of source (Bourouiba et al., 2014; Bourouiba, 2016).

Trajectories of droplets and aerosols from an infected patient (a) event of sneezing with droplets travelled for 6 m at a speed of 50 m/s within 0.12 s (b) event of coughing with droplets travelled for 2 m at a speed of 10 m/s within 0.2 s (c) event of exhaling with droplets travelled for 1 m at a speed of 1 m/s within 1 s.
Moreover, recent experiments conducted after COVID-19 contagion by Bourouiba (2020) and Loh et al. (2020) have been in agreement with the findings of Xie et al. (2007). Xie et al. (2007) have reported that pathogen-bearing droplets of all sizes can travel for almost 7–8 m during sneezes and for more than 2 m (maximum of 4.5 m) during coughs.
Surprisingly, there have been contradicting insights on the distance to be maintained between healthcare workers and COVID-19 infected patients [e.g., 1 m (WHO, 2020e) and 2 m (CDC, 2020b)]. However, most of the studies on the COVID-19 virus mentioned above have been carried out in laboratories with expiration devices set on manikins; hence, no convincing information can be deduced.
Aerodynamic behavior of SARS-CoV-2-laden droplets and aerosols in different confined spaces
Many people are reported to contract the COVID-19 in confined spaces. Thus, it is worthwhile to describe how such phenomena help intensify the mass occurrence of the COVID-19 in different confined spaces under varying microclimatic conditions.
In this respect, three confined spaces such as inside the cabin of an airplane, interior space of a car, and common dormitory-type space of a healthcare or isolation center were selected.
Airplane cabin
Since over two billion people travel on commercial flights each year (Silverman and Gendreau, 2009), the behavior of SARS-CoV-2 in the cabin is paramount to be understood.
Air travelers spend extended periods in enclosed spaces, even for more than 10 h, which usually facilitates a conducive environment for the spread of infectious diseases.
Extensive aerodynamic modeling has been performed to get an insight into how the buoyant jet of coughing by an infected person of a respiratory illness spreads in the cabin of a flight (Redrow et al., 2011; Yang et al., 2017).
The hypothesis on the most affected zones within the cabin is, therefore, highlighted below.
The cabin of a flight is usually provided with airflow from cabin air outlets and individual outlets located in the overhead compartment that runs the length of the cabin.
A sheet of airflow typically in the form of a jet with lower temperatures (< 25 °C) is projected down, and finds its way towards the bottom of the cabin (return air grills located on the sidewalls) from which it goes to the underfloor area.
However, looking at a more detailed picture, there are two typical airflow fields developed (Fig. 5 a). The first zone called the jet zone, established in the upper deck areas of the cabin, is characterized in terms of large-scale circulations, while the collision zone found in the middle and lower floor area is characterized by interactions of two lateral jets (Li et al., 2017) (Fig. 5a).
In general, about 3.6–7.4 L/s of air per passenger is provided, of which half of the volume is the filtered and recirculated air, and the other half is outside air (Bagshaw and Illig, 2019). Such an arrangement brings in a complete cabin air exchange every two to 3 min (20–30 air changes per hour (ACH)) (Bagshaw and Illig, 2019).
The high air exchange rate controls the temperature gradients, prevents stagnant cold areas, maintains air quality, and dissipates payloads of virus-laden droplets and aerosols. In a typical aircraft, the recirculated air is passed through high-efficiency particulate air (HEPA) filters, with which in excess of 99.97% of particles characterized by aero-diameter of 0.3 μm could be removed from the ingress of cabin air.
Exhaled droplets and aerosols from passengers and crew often increase the humidity to an average of 6–10%, which is below the 20% normally accepted as comfort level (de Ree et al., 2000).

Trajectories of droplets and aerosols from an infected patient in the event of coughing in an aircraft (a) airflow pattern of the cabin without any cough-jet expiration (b) without any mask (c) with surgical mask (d) with N95 respirator.
In the flight cabins, because of the densely packed environment, the cough-jet released by a SARS-Cov-2 infected person is expected to break the local airflow, particularly the jet zone, and travels both forward and backward directions in the proximity of the point of exit (Fig. 5b).
Since the velocity of exiting the violent expiration (coughs) is around 10 m/s, the droplets may travel four to five seats ahead, and the aerosol-cloud could go even further away (Fig. 5b).
However, there is no lateral movement expected except the immediate passenger on either side. In contrast to the forward movement, there is a backward movement of droplets typically by one seat, but the aerosol movement may be more.
This phenomenon illustrates that about five to ten people could get infected with the disease with an infected person onboard. Nevertheless, the propensity of getting sick by exposure to a plume of aerosols produced by cough-jet is poorly understood, and the actual number of contracted cases may be far from recorded.
The Brownian motion followed by airflow jet movement governs the aerosol plume, after the dissipation of advective transport. Such movement supports an agglomeration of virus-laden aerosols in fomites at passenger levels.
It is, therefore, crucial to decide by all airlines that such suspicious fomites such as papers, magazines, pillows, and blankets be disposed of perhaps subjected to thermal destruction until the COVID-19 pandemic recedes.
Fig. 5c illustrates how the cough-jet trajectory travels with the patient equipped with a surgical mask. With the surgical mask worn, the droplets are meant to travel up to one-two seats forward, and one seat backward.
Such phenomena maybe because of the jet coming out from either side of the mask, as the mask is not tight enough on both sides. Nevertheless, the aerosol cloud will travel far from two seats front and one seat behind by the Brownian motion coupled with the airflow trajectories of the cabin.
The streamlines of airflow are usually directed downward so that there will be a contribution of virus-laden aerosols back to the people on board. The illustration in Fig. 5d is more or less the same as that of 5c, with the exception that both droplets and aerosols do not travel far.
With the N95 mask worn, an infected patient sheds droplets forward and backward by one seat and more than one seat for aerosols. The behavior of virus-laden aerosols resulted from a cough-jet has not yet been aerodynamically modeled with reasonable accuracy; hence, the actual level of impact that a single cough-jet envisages could not be simulated well.
However, there exists evidence to showcase a profound risk of COVID-19 being spread in an aircraft when a symptomatic or even asymptomatic patient is on board. Further, the environmental factors such as moderately low relative humidity (50%), low temperature (< 25 °C), and moderate ACH (< 30 per hour) would set the platform for the SARS-CoV-2 to sustain for extended periods within the cabin. Strict guidelines for the minimization of such pandemic events are, therefore, paramount.
Passenger car
International Organization of Motor Vehicle Manufacturers (OICA) has estimated that over 1 billion passenger cars travel on roads by 2019 worldwide, indicating that one out of seven people of the world has a passenger car.
When the world is open back to normalcy by lifting the present state of lockdown, people will resort to traveling by passenger cars, and consequently, there will be a propensity of spreading the COVID-19 unless precautions are taken.
We, therefore, bring in a hypothesis to illustrate the best possible ways of preventing the COVID-19 from spreading while traveling in a passenger car.
A crucial attribute that supports the spread of COVID-19 is the interior ventilation rate in the passenger vehicle, usually expressed in ACH, which depends on the vehicular speed, ventilation setting and window positions (Ott et al., 2007).
Engelmann et al. (1992) have estimated that with the air-conditioning (AC) system off, the ACH for a stationary vehicle was in the range of 0.42–1.09 per hour. With the AC on, ACH was between 1.96 and 3.23 per hour, and with the AC off and the fans on, it varied in the range of 8.7–10.7 per hour. Park et al. (1998), with the windows closed and no mechanical ventilation, have reported the ACH between 1.0 and 3.0 per hour, and with the ventilation set on recirculation, between 1.8 and 3.7 per hour.
With the windows closed and the fan set on fresh air, the ACH was between 13.3 and 26.1 per hour, and with windows open, but no mechanical ventilation, the ACH ranged from 36.2 to 47.5 per hour (Park et al., 1998).
Offermann et al. (2002) have measured the ACH by letting the vehicle move with an average speed of 29 km/h and have found that with the window open and the ventilation system off, an ACH of 71 per hour, with the ventilation system on and the windows closed, 60 per hour, and when the ventilation system was turned off, 4.9 per hour.
Following the study done by Khatoon and Kim (2020), a typical pattern of velocity streamlines inside the vehicular cabin with a moderate level of ACH assigned to a vehicle moving at a moderate speed under conditions of “AC on and windows closed” is shown in Fig. 6 a. Fig. 6a illustrates that cooled air travels to the back seats and returns towards the front on either side at a lower level.
Under such circumstances, an infected person sitting in the back seat may cough and the resultant cough-jet in the form of droplets and a plume of aerosols (with an average speed of 10 m/s; relative humidity < 50%; temperature < 25 °C; ACH < 60 per hour) spreads towards the front seat, and the plume of aerosols may drop the advective transport phenomena with lower velocities and get carried away with existing velocity streamlines once again towards the back seats (Fig. 6b).
Such phenomena may expose all passengers in the vehicle, and the risk of contracting the disease seems to be high. Two such cases have been reported in Sri Lanka, where an infected passenger had travelled sitting at the back seat in a rented car for a period not greater than 1 h with AC on and windows closed, and the driver was subsequently reported to have got infected of the COVID-19.
The other case was reported that a person had accompanied one of his siblings (an asymptomatic person) in his car with AC on and windows closed for more than 15 min. Such situations seem to be somewhat controlled when the infected person wears a surgical mask.
However, the risk factor remains the same, as loose ends of the mask shed both droplets and aerosols, although the expiration from the front of the mask is substantially reduced (Fig. 6c).
Conversely, when the infected passenger is equipped with an N95 respirator, under the same conditions, a minute payload of droplets and a faint cloud of aerosols may come out (Fig. 6d).
However, because of the circulation within the cabin, one cannot rule out that there is no element of risk. Thus, a hypothesis could be built speculating that traveling in a passenger vehicle with people aboard under conditions of AC on and window closed, has a discernible risk factor of getting susceptible hosts infected, though masks are worn.

Trajectories of droplets and aerosols from an infected patient in the event of coughing in a car with air-conditioner switched on (a) airflow pattern inside the car without any cough-jet expiration (b) without any mask (c) with surgical mask (d) with N95 respirator.
When a passenger car moves at a certain speed with windows open, the velocity streamlines are generated from front and rear windows, and finally, sweeping the passengers aboard, they exit the cabin from the rear windows (Fig. 7 a).
Such transport-phenomena are simulated using computational fluid dynamics, but detailed information on the behavior of streamlines under different environmental settings is poorly investigated.
In the case of passenger cars with windows open, different behaviors could be expected depending on the environmental settings prevailing in different geographical regions. In other words, the environmental settings for temperate climates such as East Asia, Europe, and North America (relative humidity < 50%; temperature < 25 °C; ACH > 60 per hour) and tropical climates, including South East Asia, Africa, and South America (relative humidity > 50%; temperature > 25 °C; ACH > 60 per hour) could be expected.
The studies done on the sustenance of SARS-CoV-2 have manifested that there may be a better chance for the viral-laden cough-jets to sustain in temperate climates than tropical climates, as the daily mortality of COVID-19 has been positively associated with diurnal temperature range, but negatively with the absolute humidity (Ma et al., 2020).

Trajectories of droplets and aerosols from an infected patient in the event of coughing in a car with windows opened (a) airflow pattern inside the car without any cough-jet expiration (b) without any mask (c) with surgical mask (d) with N95 respirator.
Fig. 7b shows how the cough-jet behaves in a passenger car with windows open and AC off when the car moves at a speed of less than 30 km/h.
Under such conditions, the droplets fall in the entire length of the vehicle, while the aerosol-cloud drives to the front and returns with the airflow streamlines, spreading the aerosol plume every part of the cabin in no time.
When the car moves at higher speeds (> 30 km/h) with the same environmental settings, the droplets do not travel far and confined to a limited space (even not beyond the driver’s seat), but the cloud of aerosol will drift far and finally exits from the rear windows.
The explanations given in this paper restrict the analysis only for the case where the speed is less than 30 km/h, as such speeds become the worse scenario for the sustenance of the SARS-CoV-2 virus.
The cabin environment becomes much improved when the infected person wears a surgical mask while traveling (Fig. 7c). There seems that only a minimal payload of droplets being shed from the front, but considerable load may come from either side of the mask, as the surgical mask is usually loosely fitted to the face.
Conversely, the aerosol cloud may still travel to the front area of the cabin and returns with the airflow stream coming from outside the vehicle. Nevertheless, the cabin airflow streamlines drive such virus-laden plume out of the cabin in seconds.
The cabin environment is further improved when the infected person wears an N95 respirator (Fig. 7d). Still, one has to admit the fact that there is an element of risk for susceptible hosts to get infected.
When two scenarios (Scenario 1: AC on and windows closed; Scenario 2: AC off and windows opened) are critically reviewed, one can speculate that the scenario 2 will be better in controlling the SARS-CoV-2 virus; hence strongly recommended at least until the COVID-19 pandemic ceases.
For example, the second patient of COVID-19 in Sri Lanka was a tour guide, and when he became symptomatic, he travelled to the hospital by his car driven by his son, with his wife sitting in the front seat. He made it a point to open all windows and sat behind until they reached the hospital.
The traveling time was more than 30 min, and no person in the car was infected with the COVID-19. This story epitomizes the rationale postulated above, and the relevant authorities of affected countries should come out with strict guidelines to get such best practices implemented for reduced morbidities and mortalities.
Conversely, two cases were reported in Sri Lanka, where drivers of rental cars got infected with scenario 1. Besides, letting the car park under direct sunlight with windows open for at least 30 min would be a better option to eradicate the potential payloads of the SARS-CoV-2 virus from the cabins of passenger cars.
Healthcare center
It would be imperative to explore the plausible factors of transmitting SARS-CoV-2 virus within indoor spaces, preferably makeshift hospitals, and healthcare, quarantine and isolation centers where accommodation facilities have large open spaces with many beds laid in a sequence.
Such a facility is, in this paper, described in respect of a healthcare center, but could be applicable for other indoor spaces mentioned above. It is a known fact that the SARS diseases became epidemic and sometimes pandemic, forcing the authorities seek isolation facilities beyond their usual capacities available.
Such gestures invariably drive the authorities to build appropriate healthcare centers or convert other existing facilities in a short period. Such spaces often become large floor areas whose ventilation facilities maybe poor in cleaning the virus-laden airborne plumes.
The transmission of SARS diseases in an epidemic or pandemic situation is usually 2-fold. The first being the non-nosocomial transmission by which suspected patients from outside will be brought into the healthcare center.
In addition, with time, susceptible hosts residing at healthcare centers will contract the disease through nosocomial transmission unless the ventilation facilities (> 6 ACH or 1.6 L/s/m3, negative pressure difference > 2.5 Pa, and the airflow difference > 56 L/s) are adequate (WHO, 2009). The differentiation of both these transmission modes for a given situation is, however, a daunting task and extremely difficult (Bi et al., 2007).
In a confined space of a healthcare center, appropriate management of non-nosocomial transmission should be implemented to control the onset of nosocomial transmission, where ventilation methods play a vital role.
Given the fact that inadequate ventilation prevails in a confined space, another classification indicates that 2-fold transmission types are distinguished; short-range (between individuals, generally less than 1-m apart) and long-range (within a room, between rooms or between distant locations, generally greater than 1-m distances) (Tang et al., 2006).
Expiration of cough-jets of an infected person composed of droplets and aerosols enters and mixes with air in the breathing zone of a susceptible host standing nearby (e.g., medical staff), which is capable of contracting the disease (short-range transmission) between individuals may interact to infect one another.
In the meantime, cough-jet travels long distances depending on the airflow pattern of the space through the aerosol plume (long-range transmission) contracting people a couple of meters away from the infected person.
The airflow in the confined space is often governed by a combination of differences in temperatures and humidity. Fig. 8 a illustrates the airflow patterns of an open area equipped with a series of beds meant for suspected patients with AC on and all openings closed for a tropical climate.
Airflow streamlines are first generated by the AC and pushed down sweeping the patients, and once the advective velocities diminish, airflow mass starts moving up through convective currents, as the temperature becomes hotter. The hot air will then be extracted by the AC and cleaned through a filter before sending back to the same space.

Trajectories of droplets and aerosols from an infected patient in the event of coughing in a healthcare center with ventilation provided by an air conditioner (a) airflow pattern inside the healthcare center without any cough-jet expiration (b) without any mask (c) with surgical mask (d) with N95 respirator.
Fig. 8b manifests a typical pattern of a cough-jet trajectory of an infected person in the healthcare center with the provision of an AC driven airflow.
The droplets fall within a short distance, creating an environment conducive for short-range transmission of SARS-CoV-2-laden droplets. However, the virus-laden aerosol plume travels far from the immediate neighborhood and gets airborne with the convective currents developed within the confined space (Fig. 8b).
Such aerosol plume developed could follow the airflow trajectories, which are often altered by moving objects, opening and closing of doors and windows, and temperature and humidity variations.
Besides, a certain fraction of the virus-laden aerosols will diffuse towards lateral directions by Brownian motion resulting in nosocomial transmission to many susceptible hosts in the same confined room (not shown in Fig. 8b).
These aerosol-generating plumes cause long-range transmission within the confined space, contracting many susceptible hosts far more than one could imagine.
Fig. 8c shows the cough-jet trajectory with the infected patient wearing a surgical mask. With the surgical mask worn, the payload of droplets from the infected patient reduces drastically and restricted to a small distance.
The neighboring people on either side may not be exposed to direct contamination, but they could contract the disease by touching fomites-laden viruses. However, virus-laden aerosols will travel forward and disappear via convective and diffusion processes.
Such transport phenomena may carry the disease-causing viral loads, promoting nosocomial infection. A similar scenario is observed with a patient wearing an N95 respirator, but to a lesser extent compared to that of a surgical mask (Fig. 8d).
The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team (2020) claims that although the nosocomial transmission of SARS-CoV-2 by coughing is still unclear, 1,716 healthcare workers in makeshift hospitals in China have been infected by February 11, 2020.
Such massive numbers of infections, even with appropriate PPE worn by healthcare workers, may have been propelled by the nosocomial transmission of airborne SARS-CoV-2-laden aerosols that have lingered for many hours because of poor mixing ventilation.
Lu et al. (2020) have reported an AC-propelled COVID-19 infection of a host by an asymptomatic patient in a restaurant in Guangzhou, China, indicating a likelihood of airborne transmission by poor mixing ventilation.
The CDC in a press conference has intimated that as of April 09, 2020, about 9,000 healthcare workers in the USA have shown positive results for the COVID-19 test, which could have been because of nosocomial transmission caused by airborne aerosol clouds.
The mixing ventilation driven by ceiling-held mechanical fans is also popular among developing countries, particularly of tropical regions.
For example, Sri Lanka has converted many confined spaces belonging to the military forces of the country to be mobilized as quarantine centers. Fig. 9 a shows a typical arrangement of such a space where ventilation is provided by ceiling fans.
It is found that the people who are quarantined are given bed facilities at a distance of 1 m between each other, as shown in Fig. 9a. The mechanical ventilation propelled by ceiling fans generates downdraft airflow with an advective force, and it sweeps against people in the confined space.
As the airflow passes the people and objects in the confined area, it becomes warmer and starts moving up through the process of convection (Fig. 9a).
Such warm air travels upward the ceiling and, perhaps, exits from openings. If there are no adequate openings, poor indoor ventilation sustains, and such warm air may fill in the whole confined space resulting in nosocomial infection by SARS-CoV-2-laden plumes. Fig. 9b shows such an occurrence where droplets and a plume of aerosols being shed by an infected person. Fig. 9c and d illustrate environmental settings with the infected person equipped with a surgical mask and an N95 respirator, respectively.
Under both cases, droplet transmission seems to be subdued to a greater extent, but the virus-laden aerosol transmission will be plausible. The common scenarios of healthcare centers such as inadequate openings restricting the fresh air ingress and exit, not having an adequate number of fans to impart acceptable ACH, a large number of people living in such a facility, and inadvertent blockages of air paths by people’s belongings, equipment, and movements, among other things may cause poor ventilation in the environmental settings and trigger COVID-19 outbreak through the nosocomial transmission.
Sri Lanka reports that as of April 30, 2020, in a Naval Complex in Colombo, there have been more than 150 sailors contracted with the COVID-19. The sailors have been on duty in cordoning off of potential areas of COVID-19 pandemic.
However, it has been brought to the notice that when they returned to the base, many of them have stayed in confined areas whose ventilation potential driven by mechanical fans was rather poor.
This scenario has been a classic example of the airborne infection caused by poor ventilation that has promoted the virus-laden aerosol plume to linger for many hours inside the building.

Trajectories of droplets and aerosols from an infected patient in the event of coughing in a healthcare center with ventilation provided by ceiling fans (a) airflow pattern inside the healthcare center without any cough-jet expiration (b) without any mask (c) with surgical mask (d) with N95 respirator.
Taking all case studies mentioned above into consideration, one cannot simply ignore that both droplet and aerosol laden transmissions of COVID-19 are uncertain; hence administrative, clinical, and physical best management practices are paramount in implementing, especially in confined spaces.
More information: Maogui Hu et al. The risk of COVID-19 transmission in train passengers: an epidemiological and modelling study, Clinical Infectious Diseases (2020). DOI: 10.1093/cid/ciaa1057



{kind=link}