










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The UNC School of Medicine laboratory of Camille Ehre, Ph.D., Assistant Professor of Pediatrics, produced striking images in respiratory tract cultures of the infectious form of the SARS-CoV-2 virus produced by infected respiratory epithelial cells.
The New England Journal of Medicine featured this work in its “Images in Medicine” section, published today.
Ehre, a member of the UNC Marsico Lung Institute and the UNC Children’s Research Institute, captured these images to illustrate how intense the SARS-CoV-2 infection of the airways can be in very graphic and easily understood images.
Her lab conducted this research in collaboration with the labs of Ralph Baric, Ph.D., the William R. Kenan Distinguished Professor of Epidemiology at the UNC Gillings School of Public Health, who holds a joint faculty appointment at the UNC Department of Microbiology and Immunology, and Richard Boucher, MD, the James C. Moeser Eminent Distinguished Professor of Medicine and Director of the Marsico Lung Institute at the UNC School of Medicine.
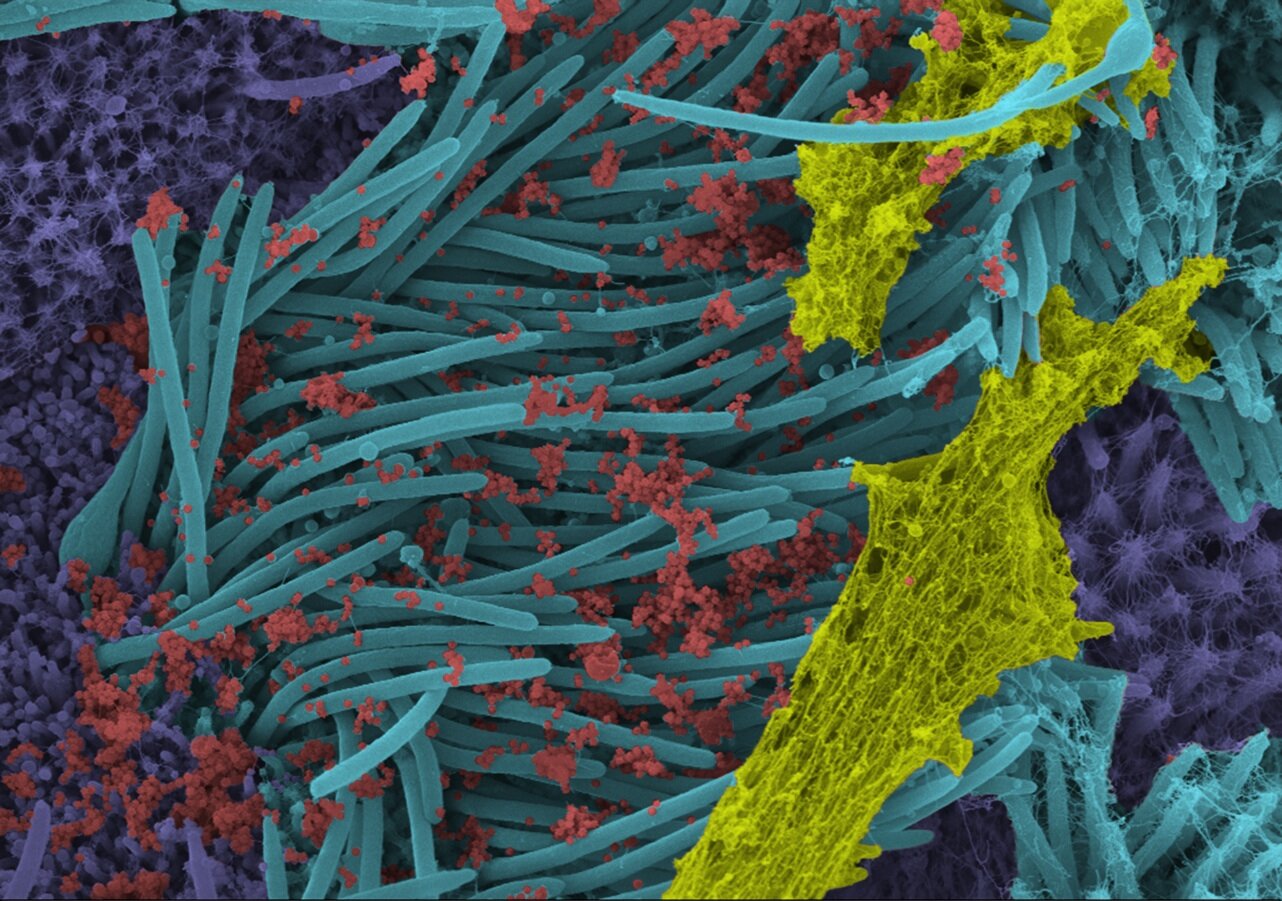
In a laboratory setting, the researchers inoculated the SARS-Co-V-2 virus into human bronchial epithelial cells, which were then examined 96 hours later using scanning electron microscopy.
The images, re-colorized by UNC medical student Cameron Morrison, show infected ciliated cells with strands of mucus (yellow) attached to cilia tips (blue).
Cilia are the hair-like structures on the surface of airway epithelial cells that transport mucus (and trapped viruses) from the lung.
A higher power magnification image shows the structure and density of SARS-CoV-2 virions (red) produced by human airway epithelia.
Virions are the complete, infectious form of the virus released onto respiratory surfaces by infected host cells.
These images make a strong case for the use of masks by infected and uninfected individuals to limit SARS-CoV-2 transmission.
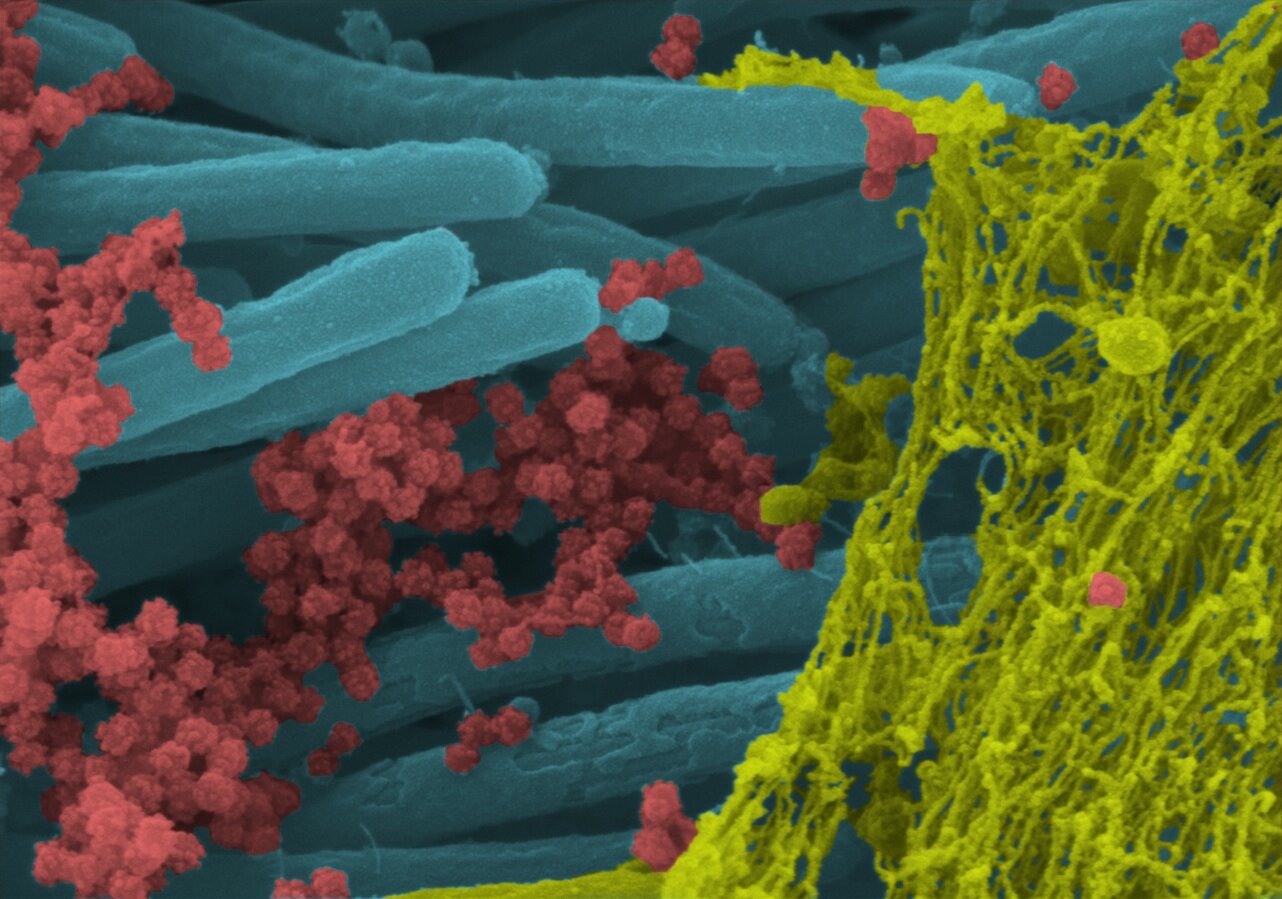
This imaging research helps illustrate the incredibly high number of virions produced and released per cell inside the human respiratory system. The large viral burden is a source for spread of infection to multiple organs of an infected individual and likely mediates the high frequency of COVID-19 transmission to others.
SARS-CoV-2 pathogenesis
Lipids play important roles at different stages in the CoVs life cycle. CoVs recruit intracellular membranes of the host cells to produce new compartments, or double membrane vesicles, which are used for the replication of the virion particle genome [55]. Recently, an important lipid processing enzyme, known as cPLA2 α has been reported to be related to the formation of double membrane vesicle and CoV’s amplification [56].
It has been demonstrated that the enzyme, phospholipase A2 group IID, is involved in anti-inflammation or proresolving lipid mediator regulation which may lead to worse outcomes in a SARS-CoV infection animal model by modulating the immune response [57].
It has been shown that there is a distinct insert that includes basic AAs in the S1/S2 priming loop of SARS-CoV-2, which is not found in SARS-CoV or any SARS-associated CoVs.
It may substantially alter the entry pathway of SARS-CoV-2 compared with other viruses of the β-CoVs lineage B [58]. In a recent report it was shown that SARS-CoV-2’s S-protein entry into 293/human ACE2 receptor cells is primarily mediated via endocytosis, and that PIKfyve, a TPC2 and cathepsin L are crucial for virus entry.
PIKfyve is the key enzyme in the early endosome involved in the synthesis of PI(3,5)P2 and its main downstream effector, TPC2. The S protein of SARS-CoV-2 could also stimulate syncytia in 293/human ACE2 cells independently of exogenous protease [59].
In a study of 452 SARS-CoV-2 infected patients, it was found that severely affected cases had lower numbers of blood lymphocytes, percentages of monocytes, basophils and eosinophils as well as increased leukocytes numbers and neutrophil-lymphocyte-ratio. In most patients with unfavorable progression of COVID-19, elevated concentrations of infection-associated markers and inflammatory cytokines was observed.
The frequency of T cells was significantly lower, and less effective in severely affected subjects. Both T helper (Th) cells and suppressor T cell numbers in patients with COVID-19 were below the reference range. The percentage of naive helper T cells was increased, and memory helper T cells and regulatory T cells reduced in severe conditions [60].
Furthermore, simultaneous to the infection with SARS-CoV-2, CD4+ T lymphocytes are quickly over-activated to switch to the pathogenic Th1 cells producing GM-CSF. The cytokines environment activates inflammatory CD14+CD16+ monocytes, leading to over-expression of IL-6 and enhances the inflammatory response.
Regarding the increased infiltrations of inflammatory cells that have been found in lungs of severe SARS-CoV-2 infected patients [61,62], these population of abnormal and noneffective pathogenic Th1 cells and inflammatory granulocytes may go to the pulmonary circulation and by immune stimulation, lead to functional impairment of the lungs and eventually death [63].
Inflammasomes are very large intracellular poly-protein signaling complexes which are constitute in the cytosol as an inflammatory immune reaction to endogenous danger stimuli [64]. NLRP3 responds to wide spectra of pathogens and endogenous signals, and is involved in the molecular pathway of various auto-inflammatory disorders [65].
It has been reported that the SARS-CoV can induce the NLRP3 inflammasome in macrophages through ORF8b. Whereas SARS-CoV infects macrophages or monocytes, sufficient ORF8b may be present to impact on the autophagy-lysosome pathway, and NLRP3 inflammasomes. SARS-CoV replicates efficiently in lung epithelial cells.
These cells also amplify NLRP3 and support assembly of NLRP3 inflammasomes. In SARS-CoV patients, the full effect of the ORF-8b on these inflammatory cascades was observed in the lung epithelium. Interestingly, ORF8b may be involved in the ‘cytokine storm’ or ‘cytokine cascade’ and inflammasome induction which happens within intensive SARS-CoV infection [66].
SARS-CoV-2 infection stimulates the immune response in two stages. In the early stages, a particular adaptive immune response is necessary to eradicate the virus and to impede progress to a more severe condition. The protective immune response at this phase requires that the host should have excellent general health and a suitable genetic context which provides antiviral immunity [67].
Although, when the immune response protection is disabling, virus will disseminate and great damage to the affected tissues occurs, particularly in organs with a high levels of ACE2 receptor expression. The injured cells activate innate inflammation within the lungs which is mainly mediated through pro-inflammatory macrophages/monocytes. Lung inflammation is the major reason for the fatal respiratory disease at the severe stage of COVID-19 [68].
In viral infections, host antiviral microRNAs participate in the regulation of immune response to virus and are capable of targeting viral genes and interfere with replication, mRNA expression and protein translation of virion particle gene. Sardar et al. predicted the antiviral host-microRNAs specifically for COVID-19. They reported a list of six microRNAs related to COVID-19 including hsa-let-7a, hsa-miR101, hsa-miR126, hsa-miR23b, hsa-miR378 and hsa-miR98 which has been previously reported to be related to other viral infections, such as HIV [69].
Clinical presentation
Virion particles spread from the respiratory mucosa, by binding to the ACE2 receptors on ciliated bronchial epithelial cells, and after that may engage with other cells [70]. In one report from Wuhan, the average incubation period of 425 SARS-CoV-2 infected patients was 5.2 days, but it this differed between individuals [71,72].
Until now, most patients with COVID-19 have initially presented with mild manifestations in other words dry cough, sore throat and fever which spontaneously resolve. Although, some patients have developed other more severe disease such as organ failure, septic shock, pulmonary edema, dyspnea, myalgia, fatigue and acute respiratory distress syndrome [73].
In contrast to SARS-CoV, patients infected with SARS-CoV-2, development of upper respiratory tract signs and manifestations are less common, suggesting that SARS-CoV-2 may target cells in the lower airway [74].
Among cases with severe dyspnea, more than 50% have required intensive care. Some COVID-19 cases do not present with fever or radiologic abnormalities on admission, which makes initial diagnosis difficult [75].
The main characteristics of COVID-19 on preliminary CT examination including bilateral multi-lobar ground-glass opacities with a peripheral/posterior distribution and patchy consolidation, primarily in the lower lobes and fewer inside the right middle lobe [76].
The main reported laboratory test abnormalities in cases with severe COVID-19 infection include: increased levels of liver enzymes (LDH, ALT and AST), total bilirubin, creatinine, cardiac troponin, D-dimer, prothrombin time, procalcitonin and CRP [77].
The histology of liver specimens of SARS-CoV infected patients have revealed a remarkable liver injury with an increase in mitotic cells, along with eosinophilic bodies as well as balloon-like hepatocytes [78].
Cardiac involvement is another prominent manifestation of COVID-19 and is closely related to a poor outcome [79]. In a recent systematic review, the incidence rate of diarrhea varied from 2 to 50% in COVID-19 patients. It may develop earlier, or following the respiratory symptoms. Findings of several studies showed that viral RNA shedding is detect for a longer time period compared with nasopharyngeal swabs [50].
In an investigation on 1099 COVID-19 patients, of whom 23.7% had severe disease with comorbidities of hypertension, 16.2% diabetes mellitus, 5.8% coronary heart diseases and 2.3% cerebrovascular disease [80]. Another study, of 140 patients with COVID-19, found that 30% and 12% had history of hypertension and diabetes, respectively [81].
Analysis of 487 COVID-19 cases, showed that older age (odds ratio [OR] = 1.06; 95% CI: 1.03–1.1), male gender (OR 3.7; 95% CI: 1.7–7.7) and hypertension as a comorbidity (OR 2.7; 95% CI: 1.3–5.6) are related with more severe disease on admission [82]. Moreover, patients with cancer were more vulnerable to severe events from COVID-19 such as admission to the intensive care unit needing invasive ventilation, or death [83].
It has been reported that the highest viral load in throat swabs occurs at the time of development of symptoms. However, viral shedding was reported to occur before the onset of symptoms, and a major proportion of transmissibility happened before first symptoms in the index case [84]. Furthermore, severe COVID-19 cases tend to have an increased viral load and a long virus-shedding time [85].
Executive summary
The severe acute respiratory syndrome coronavirus 2 genome & structure
- All the coronaviruses are positive-stranded RNA viruses with a polycistronic genome with 6–11 open reading frames, encoding several nonstructural proteins at the 5′-end plus four structural proteins (spike surface glycoprotein [S], envelope [E], matrix [M] and nucleocapsid [N]) and multiple lineage-specific accessory proteins at the 3′-end.
- Phylogenetic analysis demonstrates that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) shares 50 and 80.0% nucleotide identity to Middle East respiratory syndrome CoV and SARS-CoV, respectively.
- The S-protein of SARS-CoV-2 is longer than for other viruses such as SARS-CoV and Bat SARS-like CoVs.
SARS-CoV-2 pathogenesis
- Virion particles spread from the respiratory mucosa, by binding to the ACE2 receptors on ciliated bronchial epithelial cells, and after that may engage with other cells.
- The S-glycoprotein mediates binding of the virus to the sensitive human cell surface receptors, followed by fusion of the virus and host cell membranes to assist viral entrance.
- SARS-CoV-2 infection stimulates the immune response via two stages. At the incubation and nonalarming stages, a particular adaptive immune response is needed to eradicate the virus and to impede progress to severe condition.
- The injured cells activate innate inflammation within the lungs, which is mainly mediated through pro-inflammatory macrophages/monocytes. Lung inflammation is the major reason for the fatal respiratory disease at the severe stage of coronavirus disease 2019 (COVID-19) infection.
- The main characteristics of COVID-19 on preliminary computed tomography (CT) examination including bilateral multi-lobar ground-glass opacities with a peripheral/posterior distribution and patchy consolidation.
Diagnosis & treatment of COVID-19
- At present, the diagnosis of COVID-19 is largely based on laboratory tests PCR and chest CT imaging technique. Although, no specific antiviral treatment for COVID-19 is currently advised due to lack of evidence.
- Several pharmacotherapeutic agents have been used for treatment of COVID-19 patients consisting lopinavir/ritonavir, hydroxychloroquine and IFN β-1A.
- Effective SARS-CoV-2 vaccines are urgently needed in order to decrease infection severity, viral shedding as well as human–human transmission. The most advanced candidates have recently moved into clinical development, including mRNA-1273, Ad5-nCoV, INO-4800 and LV-SMENP-DC, and pathogen-specific.
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7451412/
More information: Camille Ehre. SARS-CoV-2 Infection of Airway Cells, New England Journal of Medicine (2020). DOI: 10.1056/NEJMicm2023328



{kind=link}