











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



New Army-funded study looks at effects of sleep deprivation, which can greatly affect Soldiers on the battlefield.
Research conducted at the University of Rochester Medical Center and funded by the Army Research Office, an element of the U.S. Army Combat Capabilities Development Command’s Army Research Laboratory, suggests that people who rely on sleeping during daytime hours are at greater risk for developing neurological disorders.
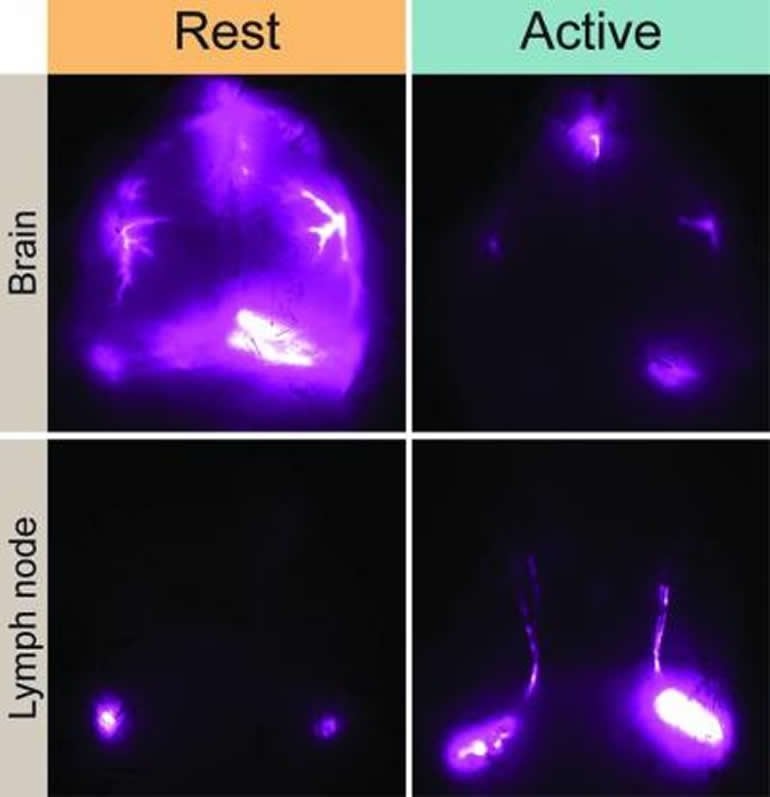
The study, published in Nature Communications, details how the complex set of molecular and fluid dynamics that comprise the glymphatic system – the brain’s unique process of waste removal – are synchronized with the master internal clock that regulates the sleep-wake cycle.
“Establishing a role for communication between astrocytes and the significant impacts of circadian timing on glymphatic clearance dynamics represent a major step in understanding the fundamental process of waste clearance regulation in the brain,” said Dr. Frederick Gregory, a program manager for ARO’s neurophysiology of cognition initiative.
“This knowledge is crucial to developing future countermeasures that offset the deleterious effects of sleep deprivation and addresses future multi-domain military operation requirements for Soldiers to sustain performance over longer periods without the ability to rest.”
The glymphatic system, first discovered by the URMC Nedergaard lab in 2012, consists of a network that piggybacks on the brain’s blood circulation system and is comprised of layers of plumbing, with the inner blood vessel encased by a ‘tube’ that transports cerebrospinal fluid.
The system pumps the fluid through brain tissue primarily during sleep, washing away toxic proteins and other waste.
“These findings show that glymphatic system function is not solely based on sleep or wakefulness, but by the daily rhythms dictated by our biological clock,” said neuroscientist Maiken Nedergaard, M.D., D.M.Sc., co-director of the Center for Translational Neuromedicine at URMC and senior author of the study.
The research team and others have shown the role that blood pressure, heart rate, circadian timing, and depth of sleep play in the glymphatic system’s function and the chemical signaling that occurs in the brain to turn the system on and off.
They have also shown how disrupted sleep or trauma can cause the system to break down and allow toxic proteins to accumulate in the brain, potentially giving rise to a number of neurodegenerative diseases, such as Alzheimer’s.
Circadian rhythms, 24-hour body clocks, are maintained in a small area of the brain called the suprachiasmatic nucleus. This clock regulates several important biological functions, including the sleep-wake cycle.
The new study, conducted in mice, showed that when the animals were anesthetized all day long, their glymphatic system still only functioned during their typical rest period – mice are nocturnal, so their sleep-wake cycle is the opposite of humans.
“Circadian rhythms in humans are tuned to a day-wake, night-sleep cycle,” said Dr. Lauren Hablitz, first author of the new study and a research assistant professor in the Center for Translational Neuromedicine at URMC.
“Because this timing also influences the glymphatic system, these findings suggest that people who rely on cat naps during the day to catch up on sleep or work the night shift may be at risk for developing neurological disorders.
In fact, clinical research shows that individuals who rely on sleeping during daytime hours are at much greater risk for Alzheimer’s and dementia along with other health problems.”
The study singles out cells called astrocytes that play multiple functions in the brain. Scientists believe that astrocytes in the suprachiasmatic nucleus help regulate circadian rhythms.
Astrocytes also serve as gatekeepers that control the flow of cerebrospinal fluid throughout the central nervous system.
The results of the study suggest that communication between astrocytes in different parts of the brain may share the common goal of optimizing the glymphatic system’s function during sleep.
The researchers also found that during wakefulness, the glymphatic system diverts cerebrospinal fluid to lymph nodes in the neck.
Because the lymph nodes are key waystations in the regulation of the immune system, the research suggests that cerebrospinal fluid may represent a fluid clock that helps wake up the body’s infection fighting capabilities during the day.
Overview of sleep
Sleep wake states can be classified as waking, rapid eye movement (REM) and non-rapid eye movement (NREM) sleep based on characteristics of electroencephalography (EEG) and electromyography (EMG) signals. Waking is defined by high-frequency, lower amplitude EEG signals and a robust EMG signal, owing to active postural and kinetic muscle activity.
In contrast, NREM sleep EEG exhibits lower frequency, higher amplitude signals following more synchronized neural firing patterns and a reduced amplitude EMG. REM sleep EEG reverts back to high-frequency, lower amplitude signals reminiscent of waking, yet the EMG signals are devoid of activity, referred to as atonia, which is used to differentiate REM from waking in polysomnographic recordings [6].
Sleep and waking are both active processes in the brain, yet different mechanisms drive each state. Cognitive arousal is largely mediated by excitatory brainstem structures and neurochemicals such as the peduncolopontine nucleus (acetylcholine), locus coeruleus (norepinephrine) and raphe (serotonin), as well as the midbrain tuberomamillary nucleus (histamine) that activate thalamic and cortical structures. In contrast, inhibitory cells in the hypothalamus (ventrolateral preoptic area) send γ-aminobutyric acid (GABA) and galanin projections to inhibit these structures, amongst others, to initiate sleep.
Recent evidence from another midbrain inhibitory structure, the rostromedial tegmental nucleus [7], suggests a distributed ventral inhibitory system may exist that promotes sleep (Jhou and Good et al., unpublished data) [8].
One explanation of this reciprocal relationship is referred to the “flip-flop circuit” theory proposed by Saper et al. to finitely explain hypothalamic regulation of NREM sleep and NREM transitions to REM and waking states [9, 10].
During development, sleep/wake patterns change such that infants require approximately twice the amount of sleep time as mature adults, but do so in a fragmented pattern throughout the day and night [11,12,13].
As development progresses, the number of sleep bouts gradually consolidate to the adult cycle consisting of a single ~8 h nightly sleep episode during which the individual transitions through NREM and REM stages. In adolescents and early adulthood there is an increase in sleep pressure that can escalate sleep need and duration to ~9 h per night [14, 15], and shift bedtimes and awakenings to later hours.
This time period coincides with the age group who typically enlists in the United States (US) military post-high school (17–20 years of age) [16]. At this ontogenetic time, sleep/wake cycles are still transitioning to adult patterns [11]. This runs counter to the sleep/wake schedules of military training to which these adolescents enter, where <6 h of sleep per night and rise times of 04:30 are commonplace [17,18,19,20].
Unfortunately, insufficient sleep <6 h per night becomes chronic and normative during early training and is pervasive even at elite military academies [17, 19]. To test the impact of sleep schedules on health and performance, Miller et al. shifted the sleep schedules of US Army trainees during Basic Combat Training to better align with the natural sleep drive and habits of adolescents.
Results showed reductions in mood disturbances, improvements in marksmanship and less fatigue, as well as overall improvements in scores of sleep quality [18], highlighting the significant impact of natural sleep drive on human performance.
It’s hypothesized that these early adolescent improvements in sleep hygiene during basic training, a time when most trainees sleep patterns are still developing, could carry forward to increased resiliency against future circadian/sleep disruptions or mental illness.
Longitudinal studies suggest that sleep disturbances in young adults serve as an early risk factor for developing major depression [21,22,23], and this risk could persevere for many years [24]. Additionally, pre-deployment insomnia is a significant contributor to post-deployment PTSD and suicidal ideation [25,26,27].
A recent model of insomnia in US military veterans identifies early sleep problems as an initial, precipitating stressor that may reduce resilience to subsequent stressors, including persistent sleep problems [28]. This feed-forward pattern could impair an individual’s adaptive capacity to cope with additional or larger stressful events, predisposing them to depression, anxiety or PTSD.
Whereas it remains unknown if mitigating sleep disturbances early during basic training could afford protection against future mental illness in military populations, effort should be directed to determining if early intervention to minimize sleep debt could reduce subsequent negative outcomes in this susceptible population.
Although, given the military culture where sleeping less is common throughout ones career, and is largely viewed as a sign of mental and physical toughness, it is unclear if early improvements in sleep hygiene could overcome many subsequent years of disordered sleep.
Nightly sleep duration for US service members is truncated, as compared to civilian counterparts. The National Sleep Foundation, American Academy of Sleep Medicine, and Sleep Research Society all recommend a minimum of 7 h of sleep per night for adults 18 years of age or older [15, 29]. Indeed, a large national US epidemiology study found that 63% of Americans slept 7–8 h per night, whereas only 28% slept 6 or fewer hours per night, consistent with short sleep duration (SSD) [30].
This contrasts with two US military studies which found 72 and 69% of service members were classified as SSD with less than 6 h of sleep per night, and only 27 and 30% obtained the recommended 7–8 h of sleep, respectively [3, 31]. Redeployed US Army Soldiers with prior combat exposures were most likely to have SSD, whereas being wounded or injured during combat was a strong predictor of sleeping less than 5 h per night post-injury [31].
Operationally, SSD truncates opportunities to maximize the recuperative value of sleep required of highly mentally and physically demanding tasks inherent of military operations. SSD also degrades next-day performance as found in a sleep duration study of artillery marksmanship [32, 33], compromising personal safety as well as resources.
Consequences of military work schedules
The biological impact of rotating work schedules has been extensively studied, yet examples focused on military personnel and operations are sparse despite operational work cycles of 12 h and 24 h being common-place. This is due in part to the non-controlled dynamic settings in which data would have to be collected, where the mission comes first and duties cannot be routinely interrupted for data collection efforts.
Even prospective studies evaluating the effects of shift schedules are challenging in the military population due to the variable and temporary nature of most work schedules and environments, and are more likely to yield less conclusive results than civilian studies where work schedules tend to be more consistent.
Further, the confounding and variable factors that must be statistically accounted for across subjects would be immense given the situation and task specific nature of service member’s duties. Fortunately, there are numerous human studies of cognitive, endocrine, and molecular function during reverse sleep cycles (i.e., night shift work), 24 h work schedules, and rotating (rapidly shifting) work schedules in healthcare (e.g. nurses) and public service (e.g., firefighters) workers with translational value to military personnel.
One military population that is more conducive to short-term studies of shift work is the Navy, where Sailors are deployed on ships for days to weeks at a time and tend to have more defined watch duties while at sea. Researchers located at the Naval Postgraduate School have published a number of studies that leveraged this population, with particular emphasis on deriving watch schedules that better align with circadian rhythms [34] and offer more time for dedicated sleep [35] than the common rotating 5 h on/10 h off watch schedule [20].
These studies consistently suggest that Sailors prefer the 3 h on/ 9 h off watch schedule, with less reported daytime sleepiness and improved mood and reaction times with fewer errors. Although this military population is more amenable to studying the effects of shift schedules, care still must be taken when generalizing sleep and physiology results across ship departments [36, 37].
For instance, salivary cortisol levels can vary across individuals due to increased stress in noisy departments (e.g., engine rooms and gun turrets), whereas light intensity can shift melatonin levels depending on duty station (e.g., interior control room versus outdoor ship bridge) [37]. In another military population, surveyed US Army Aviation personnel working a reverse sleep cycle reported that they did not achieve adequate daytime sleep when working this schedule [38], which can lead to pilot errors [39].
Night shift work (reverse sleep cycles)
In general, night shift work of any kind and duration increases morbidity and mortality, negatively impacting both physiological and psychological health. Regarding physiological health, night shift work in female nurses leads to unhealthy lifestyles that excludes exercise [40] and increases overall caloric intake and craving for high-fat, high-sugar, and protein-deficient foods [41] by means of altering gut-derived release of hormones regulating hunger and satiety (ghrelin) [42].
Interestingly, positive stress such as exercise has even been shown to exacerbate clinically significant endocrine disruption of ghrelin, leptin, insulin, and triglyceride levels [43] induced by night shift work [44, 45], indicating that the timing of exercise must also be properly calibrated in night shift workers.
These results have direct corollaries with military populations, leading to reduced ability to control one’s weight despite semi-annual evaluations in order to maintain current military occupation and to determine odds of deployability (AR 600-9). In the long-term, a higher body mass index (BMI) “set point” in service members manifest from shift work may lead to gastrointestinal tract issues and type 2 diabetes as found in civilian counterparts [40, 46, 47].
Night shift work can also reduce skeletomuscular (isometric) strength by 20% in civilian populations [48], can contribute to increases in musculoskeletal symptoms in US Navy crewmembers [49], and lead to cardiovascular stress through an increase of the blood-borne marker, cyclooxygenase-2 (COX-2) [50].
As a longitudinal consequence of night shift work (20,142 shift workers studied across 22 years), new cases of hypertension increased by >10% [51]. This trifecta of hypertension, reduced isomeric strength, and higher BMI increase the risk for cardiovascular disease.
Finally, night shift work in police officers – a civilian occupation with many overlapping responsibilities as military personnel – have heightened blood-borne markers of inflammation (increased white blood cell counts, lymphocytes, and monocytes) [52], potentially leading to new cancer cases specific to biological sex (breast [female] and prostate [male]).
In the short-term for military personnel, this trifecta could increase the risk of musculoskeletal injuries [49] and/or myocardial infarction while engaging in physically demanding tasks specific to military occupation. Post-military service, this trifecta could contribute to the increased risk for heart disease in veterans [53]; a finding that could be compounded by the lack of mandatory early morning exercise sessions and field training that are no longer part of a service members routine, as well as injuries or neurological disorders incurred during service, amongst other factors.
Regarding psychological health and performance, basic and advanced cognitive processes such as reaction time to respond to visual cues and the ability to quickly and correctly perform mental calculations are impaired in nighttime healthcare workers compared to daytime counterparts [54, 55].
Similar to healthcare workers, military occupations have unique skill sets requiring service members to accurately and rapidly attend to, process and integrate new information specific to one’s occupational duties as part of a military mission. Cognitive shortfalls in the ability to quickly learn, remember, and execute a specific task can lead to mission failure and can compromise individual and unit safety as well as national security.
Further, night shift work leads to long-term elevations in psychological stress and “burnout” that can be detrimental to sustained performance [56]. The extent of reduced attention and vigilance during night shift work can be predicted by, and is directly related to, the extent of misalignment between working schedules and two distinct physiological processes: (a) daytime peaks in core body temperature (when alertness is higher); and (b) nighttime peaks in dim-light melatonin onset (DLMO; when alertness is lower) [57].
Two separate population-based cohorts derived from the Swedish Twin Registry (largest twin registry in the world) demonstrated a clinically significant, dose-response relationship between duration of shift work and night shift work (in years) and incident risk for neurocognitive disorder (as determined from International Classification of Disease [ICD] and Anatomical Therapeutic Chemical Classification System [ATC] codes from patient registers) [58].
This risk was amplified in carriers of the APOE4 mutation [58], common in individuals of European descent [59], who worked a shift or night schedule for more than 20 years. Results from this study suggest that shift work of any duration could increase the risk for neurocognitive disorder many years later, although this needs to be confirmed in other populations.
Similar studies should be explored in military veterans, where medical histories, occupation, and work histories, and deployments are documented. The interplay between shift work, night shift work, and traumatic brain injury is another avenue that could yield insight into increased risk for subsequent neurocognitive disorders.
Rapid time-zone, light/dark shifts
In general, light is the most potent environmental stimulus capable of entraining, but also phase-shifting, the mammalian sleep/wake cycle. Depending on when white- or blue-enriched light (but not red-enriched light) of any duration is presented at night, light will phase-delay or advance the sleep/wake cycle, as characterized by the photic phase-response curve [60, 61].
This physiological response to timed light exposure can help ameliorate the negative consequences of night shift work as first shown >20 years ago [62]. Light timing and quality does matter as evidenced by the implementation of light “recipes” [63,64,65] and the efficacy of light-block wearables for optimizing immediate physiological alertness under various night shift schedules [66]. For military personnel, timed light “recipes” can be a solution for phase-shifting sleep/wake cycles for the purpose of “owning the night,” and executing a successful night mission that maximizes performance and reduces risk for injury.
Poor quality and limited artificial incandescent light is common of military installations with 24 h operation centers, necessitating an understanding of the short-term and long-term impact of these conditions on physiological and psychological health in military populations.
Incandescent lighting compared to natural sunlight (>10,000 lux) was shown to reduce sleep quality through a dampening in the amplitude of nighttime melatonin release [67], and natural light compared to artificial light results in better consolidation of a sleep/wake cycle through more robust release of brain-derived melatonin [67]. Rapid changes in sleep/wake patterns can shift melatonin release out-of-phase with military duty schedules and result in increased sleepiness during work hours when vigilance needs are high [37].
Whereas a constant dim light routine typically yields benign impact on physiological and psychological health, chronic bright light was shown to cause sleep/wake arrhythmia and sleep/wake rhythm splitting [68], dampen rhythmic gene expression [69], and functionally lead to reduced insulin sensitivity and immune deficiency in rodent models [70, 71].
Nighttime light pollution is also a significant problem in operating environments. Nearly all service members who have to relieve bodily functions in the middle of the night have to get dressed and walk more than 250 m outside in order to use the latrines [39], which can be located inside a facility that is lit 24 h using incandescent lighting.
Stadium-type lighting is also used to illuminate these trekked paths on operating bases, further compounding light pollution in already poor living quarters for restorative sleep. In both instances, the bright light can serve as a zeitgeber that reduces an individual’s ability to fall back asleep upon returning to their bunk, further dysregulating their sleep patterns.
With better integration of more natural lighting on military installations, service members could maximize their opportunities for achieving restorative sleep on non-training days and, most importantly, to maximize this opportunity for “sleep banking” leading up to sleep loss during multi-day training exercises or operations [72].
Sub-acute physical and psychological stress can act as non-photic zeitgebers in rodent models by means of altering circadian-controlled rhythms of corticosterone [73, 74]. Physiological stress reactivity in humans is circadian-controlled [75], suggesting that stressors may potentially alter circadian rhythms at specific times of the day.
It is well known that service members are exposed to more acute physiological and psychological stress in operating environments compared to the general population. Therefore, amplitudinal and phase-shifts in cortisol rhythms induced by acute stressors experienced by service members may also serve as a zeitgeber [37], similar to bright light exposure, but certainly warrants further investigation.
Nonphotic stimuli such as exercise [76,77,78,79] and social interaction [80] are also capable of entraining and phase-shifting the mammalian sleep/wake cycle, [78, 79, 81, 82], yet nonphotic cues are highly complex and can cancel out the phase-shifting actions of light in animal models [81].
In humans, exercise can phase-shift circadian rhythms; an effect that is additive to bright light exposure [83]. Time of day also plays a role, with recent evidence suggesting multiple time windows to include exercise to adjust circadian rhythms [84]. These exciting results suggest the timing of novel non-photic stimuli (e.g., military warrior tasks and battle drills) must be carefully controlled when seeking to purposefully and effectively phase-shift a sleep/wake cycle with enriched light for greater performance operability at night. Although, this level of circadian coordination is not currently adopted by military units.
To add to the problem, around-the-clock military operations often result in routine back-to-back phase-advances and subsequent phase-delays of traveling from “safety bases” >2 time zones away from the front line of troops. Recent research in an animal model demonstrated that phase-advances and subsequent phase-delays (or vice versa) can be a “zero sum game” by means of creating circadian decoupling and dampening rhythmic gene expression [85] and functionally impairing memory encoding and recall [86, 87].
Therefore, there is a critical need to better understand these biological underpinnings of human performance in response to novel photic/non-photic stimuli specifically for military personnel in order to better operate at night, while also ensuring that the physiological and psychological health of military personnel are being optimized in the short- (combat) and long-term (career and retirement).
24 h operational tempos
In contrast to the majority of civilian occupations, US military operations are around-the-clock.
Unpredictable and ever changing duty schedules and >24 h operations are not only common during deployment to a combat zone (i.e., operating environment), but are also seen stateside (i.e., in garrison) in order to create a continuous information flow to and from the operating environment.
Service members must often engage in mid-night teleconferences with a unit operating >8 time zones away in the Middle East or Pacific Islands (anti-phasic coordination), and then still perform their daily duties the next day under shortened and fragmented sleep.
The reverse is also common; higher military headquarters communicating during daylight hours in Washington, DC with units engaging in nighttime operations in the Middle East often means that service members executing nighttime operations are awake >12 h preparing for the mission even prior to the overnight mission itself.
This scenario is exemplified by the US military’s pride in “owning the night,” meaning that high-risk operations against enemy forces are prioritized at night instead of during the day (e.g., mid-night capture of Osama bin Laden in Abbottabad, Pakistan in 2011).
Although we, as a nation, will also often remember and glorify these highly publicized overnight missions, many smaller scale and lesser publicized nighttime missions have significantly compromised the health and safety of US service members and have resulted in mission failure as a consequence of long-standing nighttime shift work, coupled with chronic insufficient sleep, that affords many opportunities for performance decrements and errors following this operational schedule.
Outside of combat operations, it is also very common for service members to go on multi-day training exercises and sleep <5 h per night (Skeiky et al., unpublished data). Thus, around-the-clock military operations continue to place added risk on life-and-death decisions made by sleep-deprived service members working in highly stressful environments across many geographical regions and battlefield domains (i.e., land, sea, and air) with increasingly advanced weapon and data systems requiring a high degree of cognitive throughput.
Given the requirement to complete physically and mentally demanding tasks on a consistent basis during mission execution, the inability to perform and recover due to the inability to achieve restorative sleep, is a setup for mission failure.
Studies examining the consequences of a single night of >24 h sleep deprivation and chronic sleep restriction (<7 days) have yielded immediate, short-term compromises in physiological and brain health at levels of neural connectivity, endocrine and molecular signaling cascades, and psychological/behavioral outcomes.
For instance, a study of real-time brain function via positron-emission tomography (PET) found that a single night of >24 h sleep deprivation rapidly increased tau- and amyloid plaque accumulation – two gold-standard signatures of brain inflammation and risk for Alzheimer’s disease – that did not fully return to baseline levels after recovery sleep [88].
Immediate, clinically significant declines in anabolic processes such as decreases in blood-borne testosterone and growth hormone release [89, 90], concurrent with increases in catabolic processes such as blood-borne cortisol release [89,90,91,92,93] and oxidative stress [94] have been reported following acute sleep deprivation.
Extended sleep deprivation also phase-shifts and dampens the amplitude of biochemical substrates of glucose, fatty acid, and amino acid metabolism: including cholesterol [95], acylcarnitines [96], oxalic acid [97, 98], and diacylglycerol [97, 98]. At the most microscopic, cellular levels of study, sleep deprivation alters the human DNA transcriptome [99] and ATP synthesis [94].
These human studies show the broad neural, endocrine, tissue, and cellular impacts of a single night of >24 h sleep deprivation and chronic sleep restriction (<7 days) on both physiological and psychological health that are highly relevant to the duties of service members.
Sleep and psychiatric disorders
It is estimated that over 60% of service members who never, previously, or were currently deployed sleep less than 6 h per night, with those previously or currently deployed more likely to report sleeping <5 h per night [100]. There are several factors contributing to the lack of sufficient sleep in the military, including combat operations, shift work, and the comorbidity of psychiatric disorders in service members.
Although real-time physiological and psychological health data in active duty personnel during deployed military operations is sparse, sleep disturbances, namely insomnia and obstructive sleep apnea (OSA), have been broadly studied pre- and post-deployment and across sexes in medical treatment facilities [3,4,5, 101, 102].
Insomnia is often a principal symptom in many psychiatric disorders, most notably in PTSD, depression, and mild traumatic brain injury (mTBI). In a study of service members with combat-related head injuries, 55.2% experienced insomnia symptoms, and 90.5% had at least one comorbid psychiatric condition [103]. Whereas sleep disturbances may result from psychiatric injury, pre-morbid disordered sleep may also predispose a service member to developing PTSD and other psychiatric conditions [104].
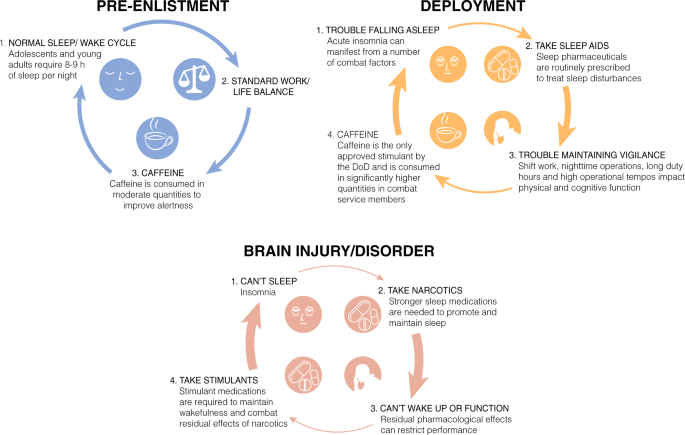
Comprehensive reviews have been written on the integral correlations between sleep and traumatic brain injury (TBI) [105, 106] and PTSD [3, 100, 107, 108], including a review by Neylan et al. appearing in this volume. Although discussing the surrounding literature is outside the scope of the current article, it should be noted that the majority of service members that endorse PTSD will also endorse significant insomnia or other sleep disturbances, (i.e. nightmares), posing a unique challenge to treating this patient population (Fig. 1).
Insomnia
Insomnia is the inability to fall asleep or stay asleep resulting in impaired daytime function and subjective patient distress. Generally, insomnia is characterized as either transient (lasting less than a month) or chronic (>1 month). The first step in treating insomnia is identification of the underlying cause or causes contributing to the patient’s complaint, as often a symptom of an underlying psychiatric condition: PTSD, depression, generalized anxiety disorder, panic disorder, bipolar disorder, and substance dependence. In fact, several studies of active duty military personnel (ADMP) referred to a sleep clinic had insomnia co-morbid with chronic pain, PTSD, anxiety and/or depression [3,4,5].
Military providers screen for mood, anxiety, and substance use disorders prior to referral to a sleep specialist [109]. The causes for patients presenting with transient or short-term insomnia are more easily identified than patients with chronic insomnia.
A service member may experience insomnia at the beginning of a deployment because of changes in their sleeping environment, excessive noise, jet lag, shift work, the stress of being separated from their families, unpleasant room temperature, or anxiety about death or injury during deployment [110].
For instance, a cross-sectional study of deployed US Air Force Airmen found 40% of respondents had a sleep efficiency of <85% or extended sleep-onset latency >30 minutes, whereas 75% reported diminished sleep quality as compared to at home [39]. Further, night shift workers were statistically more likely to have lower sleep efficiency, greater sleep latencies, and report disturbed sleep during daylight hours due to loud noises in their surroundings.
Overuse of psychostimulants such as caffeine or modafinil prescribed for shift work can further disrupt sleep patterns, and can create a feed-forward pattern where more caffeine or prescription medication is required to maintain vigilance during the day, despite the negative consequences it has on falling asleep that night (Fig. 1).
This cycle is confounded by the additional stressors one endures during deployment, as discussed above. Unfortunately, insomnia often does not resolve when the service member leaves a combat zone. Difficulties initiating and maintaining sleep often persist for months after a service member returns home. Other causes of insomnia for the service member include:
Sleep state misperception
This condition is characterized by the patient perceiving that they are not getting enough sleep without objective evidence (i.e., polysomnography) [3, 111, 112].
Inadequate sleep hygiene
Patients engage in non-sleep-promoting activities such as exercise or use of alcohol or stimulants (i.e., caffeinated beverages) prior to bedtime [84, 113,114,115,116,117,118,119].
Altitude Insomnia
Acute adjustment to high altitude (>4,000 feet above sea level) can contribute to insomnia and increased daytime somnolence due to the stimulation of peripheral chemoreceptors [120,121,122,123].
General medical disorders
Disorders such as congestive heart failure, chronic obstructive pulmonary disease, peptic ulcer disease, pain, and gastroesophageal reflux disease are just a few general medical conditions that may contribute to insomnia [124,125,126,127,128].
Neurologic disorders
Neurologic conditions such as strokes, TBI, headache syndromes (i.e., migraine and cluster headache), trigeminal neuralgia, and neurodegenerative disorders. (i.e., Alzheimer’s disease and Parkinson’s disease) all can contribute to insomnia and change sleep architecture [27, 129, 130].
The most effective treatments for chronic insomnia are non-pharmacological, such as cognitive-behavioral therapy (individual and group) [110, 131,132,133], as well as motivational interviewing and mobile health delivery of sleep recommendations [134].
Service members are also asked to complete a sleep diary during treatment for insomnia and complete education about sleep hygiene and stimulus control measures. Despite this, use of sleep pharmaceuticals by military personnel is very high. In 2018, we found that nearly half of active duty Army personnel (>100,000 service members) were prescribed zolpidem (trade name: Ambien) or eszopiclone (trade name: Lunesta) as part of a deployment or routine visit to a military treatment facility for sleep complaints (Devine et al., unpublished data).
Sleep pharmaceuticals largely target inhibitory pathways through GABA signaling, resulting in reduced short-term and long-term neurobehavioral performance in attention and reaction time that can manifest in a dose-dependent manner [135, 136].
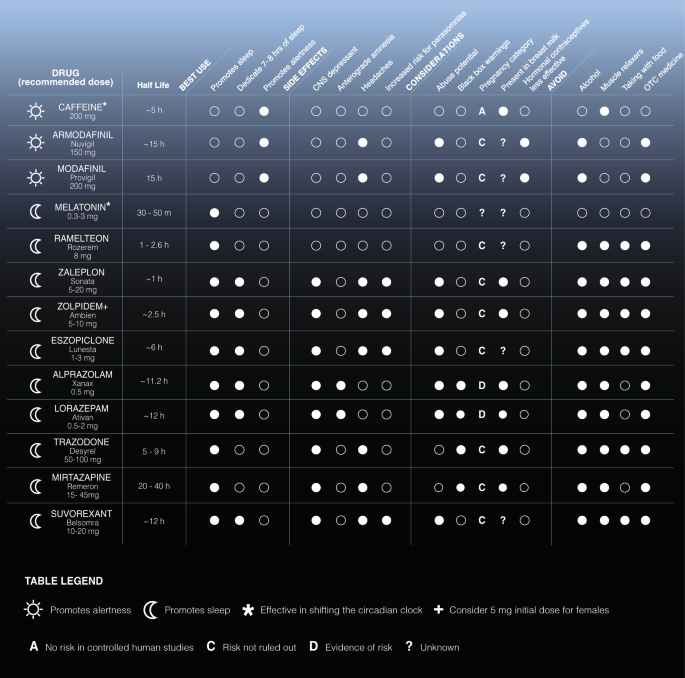
A large list of sleep/wake medications approved for use by military personnel are found in Fig. 2 (half-lives and side effects derived from a Department of Defense formulary search tool). In lieu of residual, inhibitory side effects and increased sleep inertia common of sleep pharmaceuticals, the trade-off is that military personnel must have a high level of personal accountability for use.
Missions require service members to be “on call” for 24 h, especially in combat zones. A service member who used a sleep medication the night prior to a planned mission in the early morning or an unplanned mission after mid-night awakening would likely have reduced combat effectiveness and compromised safety.
As such, US Army guidelines (ATP 6–22.5) dictate that a Soldier have at least 8 h of non-work time after taking a prescription sleep aid, although it is unknown how well this is followed.
To date, one of the most comprehensive studies of sleep amounts, disrupted sleep, and co-morbidity with physiological and psychological health states and persistent sleep disturbances in military personnel comes from the Millennium Cohort Study (MCS) [137, 138].
MCS was a 7-year study of self-reported physiological and psychological health pre- and post-deployment and across multiple deployments in >55,000 service members from all US military service branches who were active duty, Reserve, or National Guard. 22% of this study population were deployed in support of Iraq and Afghanistan. MCS found co-morbidity of insomnia symptoms with lower self-rated health, more lost work days, lower odds of deployment, higher odds of early discharge from military service, and more health care utilization [138].
Co-morbidity was highest for “short sleepers” (<6 h per night) and “long sleepers” (>8 h per night), showing intra-individual variability in a service member’s sleep “homeostat” (set point). Although, the co-morbidity with long sleepers could be explained by an underlying mood disorder (e.g. depression) that was not fully captured by the questionnaires [138].
Further, the MCS determined that sleep duration and insomnia symptoms pre-deployment were risk factors for new-onset mental health disorders following military deployment [25]. Finally, a separate study determined that the prevalence (and impact) of short sleep duration persisted during re-deployment to Iraq and Afghanistan [31].
Obstructive sleep apnea
OSA is pervasive in ADMP [5, 101, 102], similar to studies of OSA prevalence and severity with respect to biological sex in civilian populations [139,140,141]. However, salient differences between the patient populations of civilian studies [139,140,141,142], as compared to ADMP studies [5, 102], exist. Namely, ADMP diagnosed with OSA are younger (<35 compared to >40 years of age), have lower BMI (<28 compared to >30), and are more physically active than civilian counterparts; age, BMI, and physical activity are three key predictors of risk for OSA, in general.
Greater than 30% of ADMP who present with a sleep disturbance have insomnia co-morbid with OSA [5, 101, 102]. Of greatest concern in the OSA studies in ADMP is the high degree of co-morbidity of insomnia and OSA with other physiological (chronic pain) and psychological (anxiety and depression) health states, specifically for women [5, 102].
Although there are far fewer female service members compared to males, recent US government regulations now allow females to serve as combat arms officers and in forward operating units. Whereas studies of insomnia co-morbid with OSA in ADMP do not show any sex differences in self-reported sleepiness and insomnia [5, 102], polysomnography revealed a two-fold longer sleep-onset latency for women with an insomnia-OSA diagnosis and differential time spent in light NREM and REM sleep compared to males [5, 102].
In addition, female service members with a sleep disturbance had greater co-morbidity of an insomnia-OSA diagnosis with anxiety/depression not seen in male counterparts [5, 102]. Of the 100 ADMP females from Capener et al. who had a sleep evaluation, 35% had a diagnosis of insomnia-OSA (compared to 37% with insomnia and 15% with OSA, only) that was additionally co-morbid with pain at a rate of 59%, 49% for anxiety, 47% for depression, and 22% for PTSD. Thus, sex differences in the co-morbidity of insomnia-OSA with physiological and psychological health will continue to be pervasive and a critical decision point for the military as the rate of females serving in forward operating units continues to rise.
Sleep and performance
At present, there is a paradox in military regulations for optimal and minimal sleep amounts. The Leader’s Guide to Soldier Health and Fitness developed by the Office of the Army Surgeon General (ATP 6–22.5) recommends a Soldier sleep >7 h per night whenever possible.
This regulation also recommends >9 h per night in preparation for episodes of inadequate sleep. In contrast, the minimum amount of sleep a US Army Soldier is required to achieve during field training exercises is >4 h per night per Army regulation TR 350–6, for example.
A recent analysis of sleep amounts using wrist-worn actigraphy in armored (Army) battalions revealed the commonality of <5 h of sleep per night during training (at the National Training Center near Death Valley, CA) and deployment (Kuwait; Skeiky et al., unpublished data).
In most cases, these Soldiers did not have consolidated sleep of <5 h per night but rather multiple bouts of <2 h. Twenty years before this study, the same group of researchers demonstrated a strong exponential relationship between nighttime sleep amounts and next-day performance on an artillery exercise at the same training location (National Training Center).
For every hour of sleep lost, combat effectiveness degraded by 15–25% with Soldiers being at 15% total effectiveness with 4 hours per night (the current minimum per Army regulation TR 350-6) [33]. Reductions in combat effectiveness, as evidenced by cognitive performance [20] and marksmanship [197,198,199] decrements, as well as musculoskeletal symptoms [20], have been found following reduced or deprived sleep in recruits and trained warfighters. Whereas individual differences in how sleep loss impacts alertness and performance have been reported [200,201,202], only recently has the military begun exploring means to leverage these findings.
Sleep inertia is the transition period between sleeping and waking in which individuals display decrements in reaction performance and alertness, and can be seen as a reorganization of neural activity and connectivity patterns upon awakening from sleep states [203].
Rapid transitions from states of sleep to wakefulness across the nighttime and in the morning after a full night of sleep can degrade vigilance/alertness, as demonstrated by Balkin et al. in a military science laboratory [204], and are important aspects of human physiology to consider for military planning purposes. In fact, performance decrements resulting from sleep inertia experienced in the middle of a nighttime sleep episode after a few hours of sleep is similar to performance decrements under total sleep deprivation (>24 h extended wakefulness) [204].
Sleep inertia is maximal in the middle of the biological night when the circadian signal to sleep is highest, even if sleep requirements via the homeostatic system are met [205]. Sleep inertia is thought to be an operationally significant, yet overlooked problem.
In deployed situations, service members are often rapidly awoken from sleep and must immediately attend to mission requirements that involve high levels of vigilance and life-or-death decision making (e.g. defensively returning fire following a base attack).
To mitigate the effects of sleep inertia, military researchers at WRAIR demonstrated that performance decrements can be minimized through immediate caffeine intake upon waking [206]. It has also been found that sustained low-level caffeine consumption, combined with short naps, may be enough to stabilize performance and minimize sleep inertia under conditions of chronic sleep loss similar to that experienced in operating environments [207].
The ability to “bank sleep” to optimize performance under partial/total sleep deprivation, as well as enhance performance under normal conditions, is a burgeoning area of research that originated out of a military science laboratory (WRAIR) [72]. In Rupp et al., the authors showed that 10 h of time in bed (sleep extension) improved alertness and performance during subsequent sleep restriction (3 h per night) and recovery, as compared to individuals who slept their normal duration prior to sleep restriction.
Mah et al. determined that when high-level collegiate basketball players extended their sleep duration by ~2 h (similar to [72], the players’ sprint times and shooting accuracies statistically improved, and their reaction times decreased, as measured using the psychomotor vigilance test (PVT) [208]. During partial sleep deprivation, napping has also been shown to reduce heart rate and boost short-term memory in athletes [209], as well as improve endurance in runners [210].
In an observational study of habitual sleep amounts in Reserve Officers’ Training Corps (ROTC) tactical athletes, measured through wrist-worn actigraphy, Ritland et al. determined that longer nighttime sleep durations correlated with increased motivation levels and better cognitive processing performance compared to military cadets with shorter sleep durations [211]; although other performance improvements were not found [211].
In another study, the same group experimentally extended sleep duration in ROTC tactical athletes by ~1.5 h and demonstrated statistical improvements in reaction time, athletic performance and motivation [212]. Importantly, some of these improvements persisted for up to four days following the end of sleep extension [212].
Collectively, these studies suggest that extending or “banking” sleep prior to operating missions in which sleep will be restricted could confer critical improvements in reaction time and performance for service members. Given the encouraging results from these studies, additional intervention-based studies of sleep extension are warranted, as the current state of the science regarding sleep duration and long-term health [213,214,215] and performance [216, 217] is heavily driven by large-scale observational/epidemiological studies of the general population.
Psychomotor vigilance test
Despite what occurs in field training environments, sleep research in military laboratories have shown that <5 h sleep per night is not sufficient to sustain performance [72, 218]. These same laboratories have also shown that countermeasures used to stabilize performance across sleep loss are ineffective after 3 days of <6 h sleep per night [218].
Broadly, the temporal relationship between sleep loss and performance decrements has been operationalized in laboratory studies using the PVT. The PVT is a computerized test of reaction time with a means to track inter-individual variability in neurobehavioral performance in real-time [219].
The test has high ecological reliability and validity [220] and translates very well to current military demands in numerous operating scenarios, including watch duty aboard US Navy ships [221]; it can be completed to monitor real-time vigilance in any environment, harsh or benign, with the availability of a smartphone-based version funded by the Army [222].
Current warfare, termed the multi-domain battle space, is one of cognition not attrition. Service members must endure long periods of sustained attention/vigilance during low-level, monotonous activities (e.g., driving in a convoy long distances from one operating base to another), knowing that the current weapon system of choice of our nation’s enemies are IED’s placed along roadsides or rocket-propelled grenades that can injure and kill numerous individuals at a moment’s notice. In this scenario, the PVT is ideal for monitoring ones reaction time and could serve as an early predictor of fatigue or loss of attention that could be detrimental to the entire unit.
With the PVT, researchers have been able to show temporal changes in performance across total sleep deprivation (forced wakefulness) and recovery sleep in order to determine “tipping points” in neurobehavioral decline [223]. In general, performance is stabilized across 24 h forced wakefulness [223] followed by a precipitous decline with >24 h of forced wakefulness [223, 224]. This performance decline can be protected, in part, by sleep extension prior to sleep loss [72], or having a PVT session coincide with a circadian-driven peak in alertness during increasing homeostatic pressure to sleep [224]. Finally, PVT performance is also predictive of the extent of recovery from total sleep deprivation [223].
The PVT has also been widely used to determine inter-individual variability in resiliency (or sensitivity) to sleep loss under both conditions of total sleep deprivation [223,224,225] and chronic sleep restriction [218, 226]. Whereas sleep extension prior to sleep loss helps to protect against performance decline, in general [72], inter-individual variability in resiliency to sleep loss is largely biologically regulated.
Genetic association studies in humans revealed that select genotypes of an adenosine receptor (A2A) mediate the homeostatic drive to sleep [227], whereas select genotypes of dopamine metabolism (COMT) [228], and select genotypes of a clock gene (PER) known to mediate circadian timekeeping [229], can confer enhanced resiliency or sensitivity to varied conditions of sleep loss (total sleep deprivation, chronic sleep restriction; [230,231,232,233,234,235].
Resiliency to sleep loss can also be pharmacologically regulated. Caffeine’s half-life ranges from 3 to 7 h in adults [236], and can protect against performance decline during sleep loss in a dose- [237] and time-dependent manner [238]. Studies demonstrated that the ability of caffeine to sustain vigilance/alertness is genetically dependent.
Habitual caffeine intake has been associated with reduced (self-rated) sleep quality in caffeine-sensitive individuals, but not in caffeine-insensitive individuals [239], regulated in part by single-nucleotide polymorphisms of the adenosine A2A receptor gene (ADORA2A; [239].
Further, ADORA2A polymorphisms not only mediate the extent of habitual caffeine use [240], but also mediate the extent of insomnia-like changes in the EEG induced by caffeine intake [231, 239]. Select genotypes of the adenosine receptor that additionally intersect with genotypes conferring sleep resiliency also confer enhanced (or reduced) sensitivity to the ability of caffeine to stabilize performance across sleep loss [231, 232].
However, it has been shown that the performance-enhancing effects of caffeine are ineffective for stabilizing performance under chronic sleep restriction [218] (<5 h sleep per night) which is the most common type of sleep loss that service members are exposed to (Choynowski et al., unpublished data) [241].
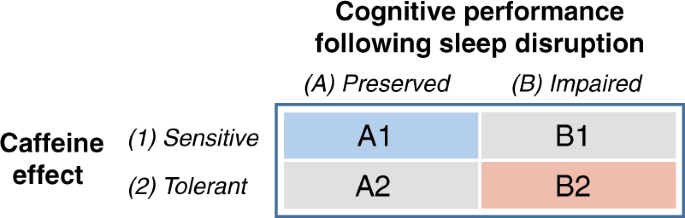
With this information, we have developed a working model to compartmentalize individual variability in sensitivity to sleep loss to determine “fitness for military duty” (Fig. 3). In our model, A1 individuals (blue box) would be most suited to perform in military operations.
These individuals would have a genetic predisposition that allows their performance to be stabilized with sleep loss, but also sensitive to the performance-enhancing actions of caffeine. B2 individuals (red box) would be least suited to perform military operations.
These individuals would have a genetic predisposition that degrades performance across sleep loss, but also linked to high caffeine tolerance. A2 and B1 individuals (gray boxes) would be moderately suited for military operations. There individuals would have stabilized performance with sleep loss (B1) but with a genetic trade-off of high caffeine tolerance (A2).
Since individual variability in performance with sleep loss is high, this lends for the ability of military commanders to capitalize on genetic heterogeneity for the benefit of combat assignment and effectiveness. In fact, the Defense Advanced Research Projects Agency is currently focused on identifying novel genetic targets in order to eliminate subject bias for the candidate selection process, as well as recognizing persons who otherwise would not have been identified using high-throughput gene sequencing techniques. Through partnerships with academia, industry, and government, the intent is to use these rapid and non-invasive high-throughput sequencing techniques to determine fitness for duty and select mission assignment in these populations through a better understanding of genes regulating sleep and circadian synchrony.
Caffeine and sleep medications for fatigue management
Because the military has thrived on 24 h shift work operations, it has a rich history of stimulant and depressant use to maintain alertness or consolidate sleep, respectively.
For instance, “Go” medications such as dextroamphetamine (Dexedrine) were once used to counter fatigue, but are no longer authorized (AFI 11–202, v3; AFSOCSUP 28 JULY 2017).
However, it is widely known that military personnel over-consume caffeine (usually through energy drinks) in order to counteract the negative consequences of shift work, which in turn, amplifies acute stress responses [242].
Caffeine abuse and overuse during training and combat is a chief reason why caffeine-dosing strategies were recently developed by Army research laboratories [238, 243, 244] and implemented into regulations (ATP 6–22.5). Caffeine, taken at the right time and in correct dosage, has the ability to improve performance on certain tasks.
For instance, 200 and 300 mg of caffeine improved marksmanship accuracy and sighting time, as compared to placebo and 100 mg, in sleep-deprived Navy SEAL trainees during Hell Week.
The 200 mg dose group showed rapid improvements at 1 h, whereas the 300 mg dose suggested improvements in accuracy could last past 8 h based on salivary caffeine levels at that time point [198].
Another reason why caffeine is often abused and overused by military personnel is that only select units, such as aviation [245], are permitted access to pharmaceutical-grade wake-promoting agents (modafinil [100–200 mg; Trade name: Provigil] and armodafinil [150 mg; Trade name: Nuvigil]), despite modafinil stabilizing neurobehavioral performance during simulated shift work in a military science laboratory [246].
Whereas in the general population modafinil and armodafinil are prescribed to treat daytime sleepiness co-morbid with narcolepsy [247] and shift work disorder [248], a narcolepsy diagnosis requires medical discharge from the military.
Stimulants and depressants also have the ability to shift sleep/wake rhythms. Independent of genetic regulation of caffeine use and psychoactive effects, one study discovered that caffeine intake (200 mg; equivalent to a 16 ounce energy drink) 3 h before bedtime phase-delayed human endocrine (melatonin) rhythms by 40 min [249] with similar extrapolated findings in human cell culture (osteosarcoma U20S; [249]) and a mouse model [250].
However, beyond elevating daytime alertness, caffeine appears unable to entrain endocrine rhythms, as demonstrated in blind individuals [251]. In humans, caffeine has been shown to alter clock-driven melatonin release [249], but more research is warranted in this area in order develop better wake- and sleep-pharmacologic dosing strategies sensitive to individual and occupational demands.
The SCN is the central circadian pacemaker and has projections onto the mesolimbic system [252], and dopamine signaling in the ventral tegmental area is clock-driven [253, 254]. In animal models, GABA-derived depressants (alcohol) and monoamine-derived stimulants (cocaine) can block the ability of the circadian system to phase-shift to photic and non-photic stimuli [158, 255, 256].
The psychoactive effects of commonly prescribed sleep aids on human circadian rhythms are mild. Trazadone, a tricyclic antidepressant, and zolpidem, a non-benzodiazepine, have both been shown to marginally advance human circadian rhythms of core body temperature [257] and improve re-entrainment to shifted light-dark cycles [258] without affecting the circadian-controlled rhythm of REM sleep propensity [257].
Although research on the ability of vigilance-promoting nootropics and hypnotics to shorten/lengthen, phase-shift, and re-entrain human circadian-controlled rhythms is limited, it warrants further investigation within the context of military operations. Circadian desynchrony has recently been recognized as an operational threat in official military reports regarding future warfare, particularly when taking longer trans-meridian travel in the current geopolitical space into consideration, and more work is needed on means to counter this desynchronization.
reference link : Neuropsychopharmacology volume 45, pages176–191(2020)
Source:US Army Research Laboratory



{kind=link}