











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A pioneering new eye test, developed by scientists at UCL in collaboration with the Western Eye Hospital, London, may predict wet AMD, a leading cause of severe sight loss, three years before symptoms develop.
Researchers hope their test could be used to identify the disease early enough so that treatment can effectively prevent any vision loss.
The findings of the study, funded by Wellcome, are published today in Expert Review of Molecular Diagnostics.
Wet age-related macular degeneration (AMD), also known as macular disease, is the most common cause of permanent and severe sight loss in the UK.
Currently the diagnosis of wet AMD relies on a person developing symptoms, which then leads them to seek advice from a clinician. Initially, someone with wet AMD would notice distortion in their vision, normally interfering with their reading.
Very quickly, this can progress to complete central vision loss, which may be extremely troubling to elderly patients who will fear blindness and loss of independence.
Wet AMD involves abnormal growth of blood vessels, which leak fluid into the retina. The introduction of new treatments has led to much improved results for patients, for a disease that over 20 years ago was regarded as untreatable.
However, patient outcomes could be even better if treatment was started in the very earliest stages of the disease.
The test, called DARC (Detection of Apoptosing Retinal Cells), involves injecting into the bloodstream (via the arm) a fluorescent dye that attaches to retinal cells, and illuminates those that are undergoing stress or in the process of apoptosis, a form of programmed cell death.
The damaged cells appear bright white when viewed in eye examinations – the more damaged cells detected, the higher the DARC count.
One challenge with evaluating eye diseases is that specialists often disagree when viewing the same scans, so the researchers have incorporated an AI algorithm into their method.
Using the same technology (test) the researchers had previously found that they can detect the earliest signs of glaucoma progression.
This new study, which forms part of the same ongoing clinical trial of DARC, assessed 19 of the study participants who had already shown signs of AMD, but not necessarily in both eyes. The AI was newly trained to detect the formation of leaking and new blood vessels, which corresponded with the spots that DARC picked up.
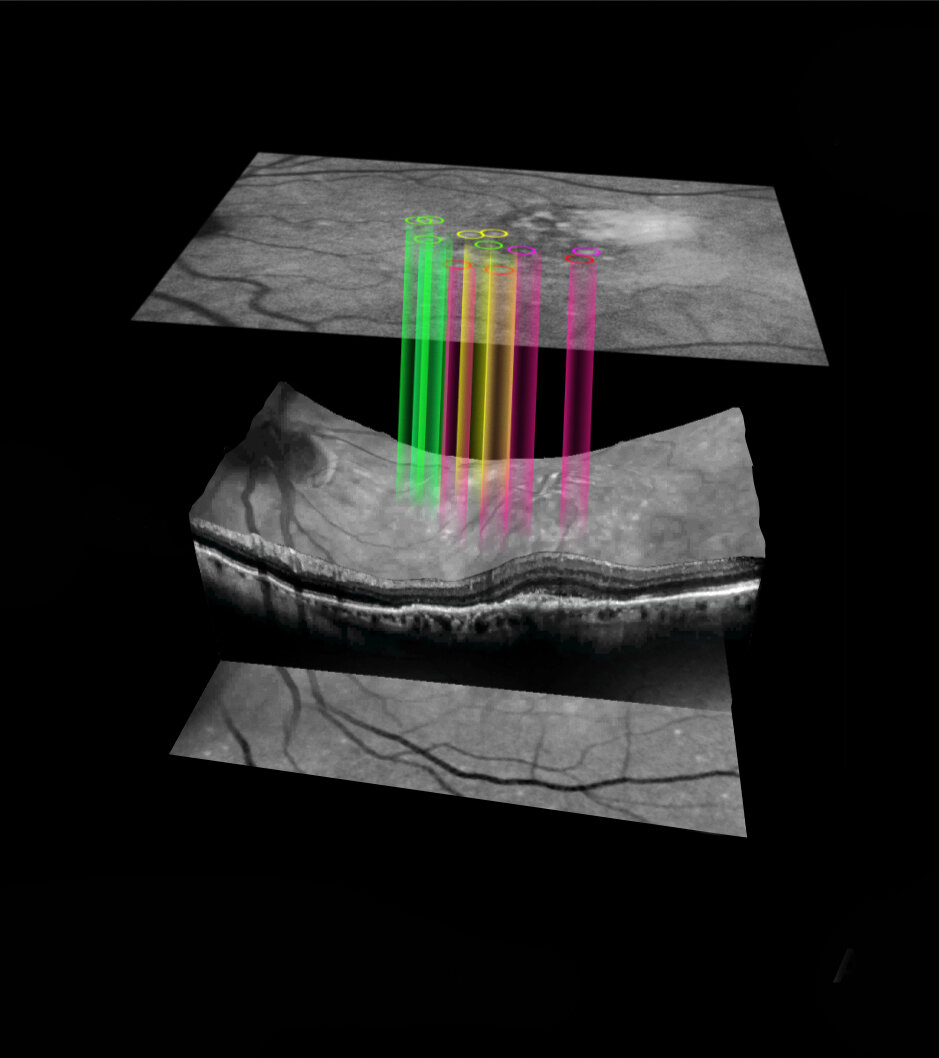
The new analysis found that DARC can uniquely highlight endothelial cells (which line our blood vessels) under stress in the retina. These stressed cells then predict future wet AMD activity with the formation of leaking and new blood vessels seen in patients three years later, using conventional eye scans with Optical Coherence Tomography (OCT).
The researchers say their test could be valuable in detecting new lesions in someone affected by AMD, often in the opposite, unaffected eye, and may eventually be useful for screening people over a certain age or with known risk factors.
Lead researcher Professor Francesca Cordeiro (UCL Institute of Ophthalmology, Imperial College London, and Western Eye Hospital Imperial College Healthcare NHS Trust) said: “Our results are very promising as they show DARC could be used as a biomarker for wet AMD when combined with the AI-aided algorithm.
“Our new test was able to predict new wet AMD lesions up to 36 months in advance of them occurring and that is huge – it means that DARC activity can guide a clinician into treating more intensively those patients who are at high risk of new lesions of wet AMD and also be used as a screening tool.”
The study team hope to continue their research with a clinical trial with more participants, and hope to investigate the test in other eye diseases as well.
Chief Executive of eye research charity Fight for Sight, Sherine Krause said: “Our Time to Focus report on the social and economic impact of sight loss stressed the importance of early detection for prevention of sight loss, and so this is a very encouraging development in tackling the leading cause of blindness.”
Glaucoma is the leading cause of irreversible blindness affecting more than 70 million people worldwide [1]. Its physiopathological process results in the excavation (“cupping”) of the optic nerve and irreversible visual loss if the disease is not detected early. Whilst it is common for this disease to progress slowly over many years, this also makes visual field changes difficult to detect over short periods of time in order to make the diagnosis.
This problem demonstrates the necessity to develop more surrogate markers which can accurately predict future vision loss. A surrogate marker is defined by its ability to predict a clinically relevant outcome such as vision loss or decrease in quality of life, as well as correlating with the disease process. In addition, the effect of a treatment on the surrogate must have an effect on the clinical outcome [2]. Their predictive power not only allows earlier diagnoses, but also affords shorter, and therefore more economical clinical trials and thus are an attractive prospect from many perspectives [2].
Presently, the most important risk factor for glaucoma is raised intraocular pressure (IOP). The Ocular Hypertension Treatment Study (OHTS) has shown that an increased IOP of 1 mm Hg is associated with a 10–25% increased risk of disease progression [3]. Although IOP is accepted as an important risk factor, its use as a surrogate has never been properly validated [4] as IOP does not always correlate with disease.
For instance, patients with normotensive glaucoma have an IOP within “normal” limits despite having progression of disease [5]. Alternatively, some patients with ocular hypertension (OHT) do not experience any perceivable visual field loss [4, 6]. Therefore, interventions such as surgery to lower IOP may not provide any benefit to some patients, whilst still exposing them to the risks of the treatment. In the Low-pressure Glaucoma Treatment Study (LoGTS), patients were treated either with timolol or brimonidine (BMD). Both treatments showed a similar reduction in IOP, but BMD was more effective at protecting from progressing visual field defects [7]. By not “capturing” the extra beneficial treatment effect in the BMD group, the results suggest that IOP may be deficient as a surrogate marker for glaucomatous progression.
With the emergence of new imaging techniques during the last decade, the use of imaging of structural biomarkers as a surrogate has been investigated. The clear structure-function relationship between visual field defects and visible changes in the optic nerve gives more comprehensive information on disease progression than IOP [8]. Indeed, some studies have shown that progressive changes in imaging of the retinal nerve fibre layer thickness is predictive of visual field loss over 5 years [9]. However, there lacks a strong correlation between these parameters measured at a single visit and future visual field loss [4]. With validation of functional endpoints, structural surrogates may prove a better biomarker for the assessment of neuroprotective therapies, as their primary goal is not to lower the IOP. This validation with functional endpoints is required in order to avoid endorsing novel therapies that have a positive effect on a structural parameter but provide no benefit to visual function.
Principles of Detection of Apoptosing Retinal Cells
Annexin-A5 is an endogenous ubiquitous protein present in animals and humans. It has the ability to bind to phosphatidylserine (PS) which is an early marker of cell apoptosis [10]. PS is normally found on the internal leaflet of the cell membrane; however, when a cell is in the early stages of apoptosis, PS flips to the exterior leaflet of the cell membrane allowing annexin to bind it in the presence of calcium [10].
Annexin V has been widely used in research during the last decade. Animal studies using radiolabelled annexin in combination with positron emission tomography or single-photon emission computed tomography have shown an increased uptake of annexin in areas where apoptosis occurs [11]. Human studies have also been performed in relation to myocardial infarction [12], cardiac tumours [13], cardiac allograft rejection [14], and neck and head carcinomas [15]. All these studies showed an accumulation of radiolabelled annexin in the areas of interest. However, the resolution of these techniques is limited by the opacity of these organs and often deep location within the body.
Due to the transparency of ocular media, the eye is a unique organ which permits direct visualisation of retinal cells. The detection of apoptosing retinal cells (DARC) is a technique using modified confocal scanning laser ophthalmoscopy (cSLO) which takes advantage of these properties of the eye in order to allow real-time visualisation of apoptotic retinal cells at a single cell level, using fluorescently labelled annexin-A5 [16] (Fig. 1).
Diagrammatic representation of DARC technology. Annexin-A5 (ANX) binds to phosphatidylserine (PS) on the outer leaflet of cells in early apoptosis. The attached fluorophore is then detected using scanning laser ophthalmoscopy.
In vivo Experimental Studies Using DARC to Date
Since the DARC technique was established in 2004 [16], we have used various experimental animal models for characterisation of the natural history of disease and assessment of neuroprotective agents. Retinal ganglion cell (RGC) apoptosis occurs not only in ocular disease, such as glaucoma and other optic neuropathies, but also neurological disorders, including Alzheimer’s disease (AD) [17-19] and Parkinson’s disease (PD) [20]. DARC imaging has been demonstrated to be a useful tool for screening drug efficacy in those models [20-24]. In this review, we only focus on DARC applied to therapeutic strategies in disease models.
Glaucoma-related models can be induced either surgically or chemically to cause RGC apoptosis. To evaluate DARC sensitivity and accuracy in monitoring RGC apoptosis, we firstly assessed its performance in well-established rat models of chronic OHT and optic nerve transaction (ONT) [16] and found RGC apoptosis was occurring over time and peaked at 3 weeks in OHT and 7 days in ONT models. At the end of experiments, RGC apoptosis accounted for a total RGC loss of 60% at 16 weeks in OHT and 76% at 12 days in ONT models. Using DARC, we also detected RGC apoptosis in a mouse model following intravitreal administration of staurosporine [25].
Glutamate excitotoxicity has been implicated in RGC death in glaucoma [25-27]. Blocking NMDA receptors by specific antagonists, such as memantine, an uncompetitive NMDA antagonist used in AD treatment [28], was reported to be effective in reducing RGC death in experimental glaucoma [29-31]. Using DARC, we have firstly assessed the effects of different glutamate modulation strategies, including a nonselective (MK801) and a selective (ifenprodil) NMDA receptor antagonists and a metabotropic glutamate receptor agonist (mGluR Group II, LY354740), in a staurosporine-induced rat model of RGC apoptosis [22].
We found that all three single agents significantly reduced RGC apoptosis in a dose-dependent manner, but combining low-dose MK801 with LY354740 appeared to be most effective compared to either agent alone. We then applied the most optimal combination regimens to the OHT model at different time points (0, 1, and 2 weeks following IOP elevation). DARC results revealed the most effective timing of treatment was at 0 weeks (the time of IOP elevation). We believe this is due to maximal inhibition of glutamate release after primary insult, resulting in reduction of secondary degeneration that can lead to neuronal degeneration far beyond the primary injury site [32].
Amyloid-β (Aβ) plaques in the brain are a hallmark in AD, with Aβ deposition also found to be implicated in the development of RGC apoptosis in glaucoma by us and others [23, 33, 34]. Aβ is derived from the proteolytic cleavage of amyloid precursor protein (APP). Two catabolic pathways are identified for APP processing. One is the nonamyloidogenic pathway via α-secretase activation, resulting in secretion of soluble forms of APP (sAPPα), and the other is the amyloidogenic pathway, where β- and γ-secretase activation leads to Aβ generation. Using DARC, we have assessed the effects of targeting the amyloidogenic pathway on RGC protection in the OHT rat model, by examining three different agents: an anti-Aβ antibody, a β-secretase inhibitor, and Congo red (CR).
CR is a dye commonly used to stain Aβ histologically and has been shown to block Aβ aggregation [35, 36]. Our DARC data showed that all three single agents altered the profile of RGC apoptosis in a temporal manner by delaying the development of peak RGC apoptosis and reducing peak levels. However, although anti-Aβ ab appeared to be more effective in prevention of RGC apoptosis than the other two agents, a combination of three agents demonstrated to be the best regimen, resulting in the maximal reduction of RGC apoptosis [23].
Modulation of the nonamyloidogenic pathway has also been investigated in the OHT rat model. BMD and clonidine (Clo) are α2-adrenergic receptor agonists (α2ARAs), drugs used to lower IOP in glaucoma patients [37]. Both BMD and Clo have been reported to be neuroprotective [38-40]. Using DARC, we have recently demonstrated that systemic administration of α2A agonists BMD and Clo significantly reduced OHT-induced RGC apoptosis in vivo.
Our results revealed that the protective effect of α2A agonists was associated with reduced levels of Aβ deposition in RGC layers, where an increase of Aβ immunostaining was found in the OHT model [23, 37]. In this study, we also found that α2ARAs modulated the levels of laminin and MMP-9 (metalloproteinase-9), potentially linked to changes in Aβ through APP processing, promoting the non-amyloidogenic pathway.
Mitochondrial dysfunction and oxidative stress mediate RGC death in glaucoma [41, 42]. Coenzyme Q10 (CoQ10) is a mitochondrial targeted antioxidant and plays an essential role in the normal function of the electron transport chain. CoQ10 exhibits neuroprotection in neurological disorders such as AD, PD, and Huntington’s disease [42], and also experimental glaucoma [43]. Using DARC, we have recently evaluated topical administration of CoQ10/TPGS (α-tocopherol polyethylene glycol succinate) micelles in the OHT rat model [44]. DARC data demonstrated that topical CoQ10 treatment significantly reduced OHT-induced RGC apoptosis compared to vehicle controls. DARC results are consistent with retinal whole-mount histology outcomes, in which topical CoQ10/TPGS but not TPGS controls can protect Brn3a+ RGCs against apoptosis as indicated by the preservation in RGC density and nearest neighbour distance.
Optic neuropathy describes a collection of disorders characterised by damage to the optic nerve and loss of RGCs due to any cause including glaucoma, ischaemia, trauma, and genetic predisposition. Experimental models of optic neuropathy can be made by transection of the optic nerve fully (ONT) or partially (pONT) [45]. The pONT model represents a reliable and reproducible model for studying secondary degeneration, a phenomenon believed to occur in the central (CNS) and peripheral nervous systems, where injury from initial lesions can lead to widespread damage to neurons beyond the primary injury site. We have used the pONT model to assess therapeutic effects on secondary degeneration [45].
Cell-based therapies are increasingly recognised as a potential strategy to treat retinal neurodegenerative disease. Their administration, however, is normally indirect and complex, often with an inability to assess in real-time their effects on cell death and their migration and integration into the host retina. Using DARC to monitor RGC apoptosis, we have assessed a novel delivery route, direct optic nerve sheath (DONS) application of Schwann cells (SC) in a pONT rat model [45].
DARC data showed that the DONS application of Schwann cells significantly reduced pONT-induced RGC apoptosis at 7 and 21 days, compared to untreated controls. The DARC results were comparable to histological findings, where SC/DONS therapy significantly increased Brn3a+ RGC survival in retinal whole-mounts, by mostly targeting secondary degeneration.
Adenosine is a neuromodulator in the CNS, with its biological effects mediated through G protein-coupled receptors. The adenosine A3 receptor (A3R) is believed to be involved in a variety of different intracellular signalling pathways. RGCs express A3R, and activation of A3R is neuroprotective. Using DARC, we have assessed the effects of intravitreal administration of A3R against RGC apoptosis on the pONT model. We found that A3R significantly reduced number of apoptotic RGCs compared to the non-treatment group. The in vivo findings were consistent with histological observations of reduced Brn3a+ RGC loss [46].
PD is an important cause of dementia worldwide; however, there are currently no effective biomarkers for early diagnosis and no effective treatments for altering disease progression. Although it is a neurological disorder, mounting evidence shows that the eye, particularly the retina, is also affected [47]. Using a rotenone-induced rat model of PD, we have assessed therapeutic strategy by DARC imaging.
We have firstly evaluated retinal changes by longitudinal imaging of RGC apoptosis with DARC and retinal thickness with OCT (optical coherence tomography) and compared them with brain histology. The imaging data revealed that RGC apoptosis significantly increases as early as day 20 of a rotenone insult, accompanied by a transient swelling of retinal layers. However, characteristic histological neurodegenerative changes in the substantia nigra and striatum occur from day 60, suggesting that retinal changes precede the pathological manifestations of PD.
We then evaluated therapeutic effects of systemic administration of different formulations of rosiglitazone by in vivo imaging and found sustained release administration of liposome-encapsulated rosiglitazone to be the most effective among the treatment regimens tested, as evidenced by significant reduction of retinal neuron apoptosis at day 20, and nigrostriatal neurons at day 60. This is the first in vivo evidence of RGC loss and early retinal thickness alterations in a PD model, as well as therapeutic assessment in the model. This would suggest that retinal changes may be a good surrogate biomarker for PD, which may be used to assess new treatments clinically.
DARC in Clinical Trials
The challenge following pre-clinical studies was to reproduce DARC technology in human subjects in order to examine its potential as a clinically useful research or diagnostic tool. DARC has now been trialled in humans, with encouraging results. ANX-776 using the human-variant annexin molecule, RhAnnexin V128, was the fluorescently labelled annexin taken forward to clinical trials. With excitation and emission wavelengths of 771 and 793 nm, respectively, this near-infrared fluorophore lends itself well to clinical translation, being compatible with the 786-nm diode laser excitation and 800-nm barrier filter used in indocyanine green imaging when examining choroidal pathology, such as in idiopathic polypoidal choroidal vasculopathy [48].
The phase I clinical trial of DARC set out to establish the safety and tolerability of the technique in humans using a Storer design [49], enrolling 8 progressing glaucoma patients and 8 healthy volunteer controls. Glaucoma patients were deemed to be progressing based on at least one mode of investigation including visual field testing, OCT scans, and Heidelberg retinal tomography. T
wo glaucoma patients and 2 healthy controls were randomly allocated to a 0.1, 0.2, 0.4, and 0.5 mg intravenous dose of ANX-776. Pharmacokinetic analysis was conducted with peripheral blood sampling at 5, 15, 30, 60, 120, and 300 min post-administration. This showed that ANX-776 was rapidly absorbed and eliminated with dose-dependent levels in the blood and no accumulation.
During the course of the trial and up to 30 days post-administration, no patients withdrew from the study, and there were no serious adverse events recorded. Six adverse events were reported including discomfort and bruising due to phlebotomy, dizziness, headache, influenza, and metatarsal inflammation, all of which were self-limiting, and none deemed to be related to the ANX-776.
A key finding was there was a significant measure of efficacy, both with respect to DARC counts being higher in glaucoma patients compared to healthy controls, but also with respect to predicting future glaucoma disease progression – in fact 18 months before changes in OCT and visual fields. This latter finding suggests that DARC could be a potential surrogate marker.
The phase II clinical trial of DARC was designed to fully characterise the differences between the counts and distribution of DARC spots in health and disease. Patients (n= 116) have been recruited into 5 different groups including healthy volunteers, progressing glaucoma, age-related macular degeneration, optic neuritis, and Down’s syndrome (in whom CNS pathology similar to AD is found [50]). The results of this trial are to be published soon.
The Impact of DARC
There is a clear need for more sensitive biomarkers in the fields of glaucoma and neurodegeneration that will allow us to detect disease earlier, and therefore instigate treatment. This is especially pertinent in neurodegenerative conditions such as glaucoma, whereby late detection may miss the considerable amount of damage that can occur prior to clinically detectable changes in visual fields [51-53].
Furthermore, the theory that cells may have a lower resistance to injury following primary insults [54] would also support early detection to prevent further cell death and subsequent secondary degeneration. Thus, instigating treatments later in the disease course is likely to result in poorer clinical outcomes and reduced observed treatment efficacy, and therefore is often given as a possible explanation for the failure of novel therapeutics in the field of neuroprotective research, as indeed is the sensitivity of diagnostic techniques used in such trials [55].
In contrast to the currently used diagnostic techniques which observe structural or functional damage that has already occurred, DARC holds the potential to observe cellular apoptotic events in real-time, which may later contribute to the changes seen in OCT parameters and visual field tests. Clinically, this has the potential to reduce morbidity from visual field loss, and the ability to conduct neuroprotection clinical trials in a faster, more cost-effective manner, whilst testing treatments in an IOP-independent manner. Further trials are needed to validate these early findings.
reference link : https://www.karger.com/Article/FullText/500527
More information: Expert Review of Molecular Diagnostics, DOI: 10.1080/14737159.2020.1865806



{kind=link}