 Competitive Coexistence: Post-War Strategic Outlook")









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Over recent years, diets which see people fast on a few days each week have increased in popularity, reinforced by images of people’s miraculous weight transformations, and backed by celebrity endorsements.
Published in the prestigious journal Science Translational Medicine, the new study from a team of physiologists at the University of Bath builds this evidence and indicates that there is ‘nothing special’ about fasting.
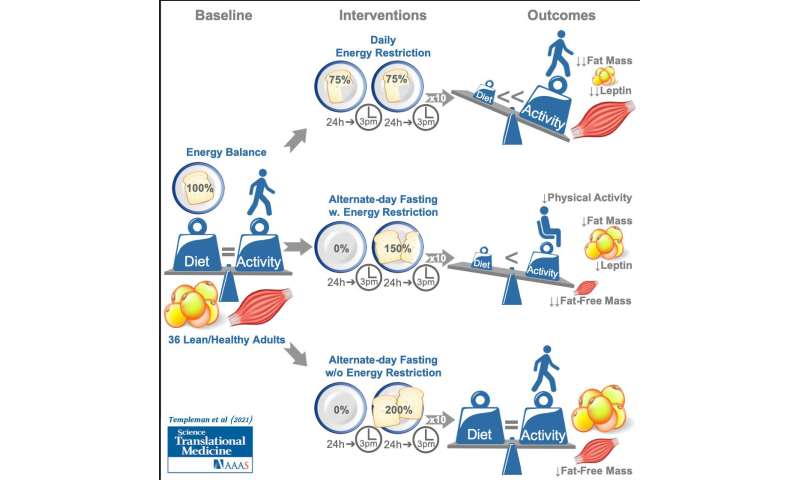
The trial, organised by a team from the University’s Centre for Nutrition, Exercise & Metabolism (CNEM), saw participants allocated into one of three groups:
- Group 1 which fasted on alternate days with their fast day followed by a day of eating 50% more than usual.
- Group 2 which reduced calories across all meals everyday by 25%.
- Group 3 which fasted on alternate days (in the same way as Group 1) but followed their fast day with one day eating 100% more than usual.
Participants across all three groups were consuming a typical diet of around 2000-2500 kcal per day on average at the start of the study. Over the course of the three-week monitoring period, the two energy restricted groups reduced this to be between 1500-2000 kcal on average. Whereas groups 1 and 2 reduced their calorie intake by the same amount in different ways, group 3’s diet saw them fast without reducing overall calories.
Their results found that the non-fasting dieting group (Group 2) lost 1.9 kg in just three weeks, and DEXA body scans revealed this weight loss was almost entirely due to a reduction in body fat content.
By contrast, the first fasting group (Group 1) who experienced the same reduced calorie intake by fasting on alternate days and eating 50% more on non-fasting days, lost almost as much body weight (1.6 kg) but only half this weight loss was from reduced body fat with the remainder from muscle mass.
Group 3, who fasted but increased their energy intake by 100% on non-fasting days, did not need to draw on their body’s fat stores for energy and therefore weight loss was negligible.
Professor James Betts, Director of the Centre for Nutrition, Exercise & Metabolism at the University of Bath who led the research explains: “Many people believe that diets based on fasting are especially effective for weight loss or that these diets have particular metabolic health benefits even if you don’t lose weight.
“But intermittent fasting is no magic bullet and the findings of our experiment suggest that there is nothing special about fasting when compared with more traditional, standard diets people might follow.
“Most significantly, if you are following a fasting diet it is worth thinking about whether prolonged fasting periods is actually making it harder to maintain muscle mass and physical activity levels, which are known to be very important factors for long-term health.”
These results focused on participants who were defined as ‘lean’ (i.e. body mass index 20-25 kg/m2). 36 people participated in the study which was conducted between 2018—2020 and funded by the University of Bath.
The full study “A randomized controlled trial to isolate the effects of fasting and energy restriction on weight loss and metabolic health in lean adults” is published in Science Translational Medicine on Wednesday 16 June.
The current obesity epidemic in developed countries is staggering in terms of its magnitude and public health impact. Healthy weight individuals (body mass index (BMI) of 18.5–25 kg/m2) are now the minority in the United States [1]. Medical spending attributable to overweight and obesity has been estimated to be over 90 billion dollars in the Unites States alone [2]. Reducing the daily calorie intake is the most widely prescribed strategy to induce weight loss [3].
Current guidelines recommend continuous energy restriction (CER; a daily energy deficit of ~500 or 750 kcals, or a 30% restriction from baseline energy requirements), along with a comprehensive lifestyle intervention, as the cornerstone of obesity treatment [4]. On average, this approach produces modest weight loss (5–10% sustained for ≥1 year) [4]. The magnitude of weight loss with CER is minimally influenced by variations in diet macronutrient content, especially during long-term follow-up [5,6,7,8,9,10]. Regardless of diet and macronutrient content, adherence to CER typically declines within 1–4 months [11]. As a result, the majority of individuals who lose weight with CER regain significant weight within 1 year [12,13,14].
Because of the relative ineffectiveness of traditional CER approaches for achieving and sustaining weight loss, there has been increased interest in identifying alternative dietary weight loss strategies. One such approach is prolonging the fasting interval between meals (i.e., intermittent energy restriction, IER). The premise of this approach is that individuals do not fully compensate during fed periods for the energy deficit produced during extended periods of fasting between eating bouts. Furthermore, these regimens may be easier to adhere to and maintain over time than CER. Finally, IER may lead to metabolic adaptations that favor a greater loss of fat mass, the preservation of lean mass, and a greater ability to sustain weight loss [15].
Various IER regimens have gained popularity in recent years as strategies for achieving weight loss and other metabolic health benefits [16,17,18]. These paradigms involve recurring periods with little or no energy intake (e.g., 16–48 h), with intervening periods of ad libitum food intake. Studies in rodents have demonstrated that IER strategies such as intermittent fasting (IMF; ≥60% energy restriction on 2–3 days per week, or on alternate days) and time-restricted feeding (TRF; limiting the daily period of food intake to 8–10 h or less on most days of the week) exert beneficial effects on the body composition, energy expenditure, and substrate oxidation. However, clinical studies comparing weight loss with IER regimens to traditional CER in adults with overweight and obesity are limited.
The objective of this review is to summarize the current evidence for IER regimens as treatments for overweight and obesity. We first review the evidence from pre-clinical studies to provide a background on the purported mechanisms by which IER induces long-term benefits for body weight and composition.
We then present a narrative review of randomized trials of ≥8 weeks in duration performed in adults with overweight or obesity (BMI ≥ 25 kg/m2) in which an IER paradigm (IMF or TRF) was compared to CER and the primary outcome was weight loss. We identified studies to include in this literature review by using specific search terms in PubMed and cross-referencing citations. The final goal of this review is to identify gaps in the current evidence base and outstanding scientific questions regarding IER strategies for weight loss.
Intermittent Energy Restriction (IER) Strategies Defined
A major problem in the field is a lack of standardization of terminology to describe different intermittent energy restriction paradigms. Mattson et al. [15,19] have used intermittent fasting as the umbrella term to define “eating patterns in which individuals go extended time periods (e.g., 16–48 h) with little or no energy intake, with intervening periods of normal food intake, on a recurring basis”.
They further “distinguish studies of short-term frequent fasting periods from studies of less frequent but longer fasting periods” by using the term periodic fasting (PF) to refer to IMF regimens with periods of fasting lasting from 2 to as many as 21 or more days. The term time-restricted feeding (TRF) is used as a subcategory of IMF to describe “an eating pattern in which food intake is restricted to a time window of 8 h or less every day”.
The categorization of TRF as a type of IMF diet is problematic because TRF is fundamentally different from a complete day of fasting or even a modified fast day (generally defined as a day on which individuals consume up to 25% of daily energy needs). As will be discussed below, TRF is simply an appropriate eating pattern (eat during the day and not at night) that humans have veered away form in the past several decades.
Rodent studies have shown that reducing the daily eating duration has beneficial effects on weight, body composition, and metabolism. Importantly, these effects are seen even without a reduction in daily energy intake [20,21,22]. For these reasons, we propose the use of the umbrella term IER, which has two distinct categories—IMF and TRF (see Figure 1).

Popular variations of intermittent energy restriction. Within the circles, each ring represents a distinct 24 h day. Green shaded areas represent eating periods. Grey shaded areas indicate the sleeping time, and white circles/spaces indicate fasting periods. Intermittent fasting (IMF) is characterized by recurring periods (e.g., 16–48 h) with little or no energy intake. Many variations have been used to study the effects of IMF on body weight, including (A) alternate day fasting (zero calorie intake on fast days), (B) alternate day modified fasting (>60% energy restriction on fast days), and (C) fasting or modified fasting on two days per week (2DW). (D) Periodic fasting involves fasting for 2 to as many as 21 or more days. This IMF paradigm is acknowledged in the present review but will not be discussed as there are few studies in the literature. Time-restricted feeding (TRF) is characterized by eating patterns that are restricted to a short (<8–10 h) interval each day, such as during the (E) early or (F) middle portion of the day.
Intermittent fasting regimens involve 60–100% energy restriction on fast days with ad libitum energy intake on fed days. Various IMF regimens have been proposed, with the most popular being alternate day fasting (ADF) and a regimen of fasting for two days per week (2DW). A common and appealing feature of IMF is that dieters do not have to restrict calories every day [17]. Weight loss likely occurs because individuals do not fully compensate on non-fasting days for the calorie deficit that occurs on fasting days [23,24,25,26,27]. Furthermore, the periodic nature of fasting may mitigate the constant hunger associated with CER [28]. For example, several studies using a modified fasting paradigm (~25% of energy requirements on fast days) have shown that hunger decreases [23,29] or remains unchanged [30,31] from the baseline over an 8–12 week IMF intervention.
TRF refers to an eating pattern in which the food intake is restricted to a time window of 8–10 h or less every day. Recent studies in humans suggest that the median duration of eating is approximately 14.5 h per day, and the assumption that most individuals regularly undergo an “overnight fast” may thus be incorrect [32]. Eating “around the clock” has been suggested to have detrimental effects on health and body weight, leading to a desire to study time-restricted feeding as a weight loss strategy [15]. Limiting the eating duration may be an effective strategy to reduce the overall caloric intake; however, TRF does not necessarily have to involve caloric restriction. TRF is distinct from IMF because it involves an element of timing optimally aligned to the biological day.
Effects of IMF on Body Weight, Body Composition, and Metabolic Outcomes: Evidence from Preclinical Studies
A key research question is whether IMF elicits benefits for body weight and peripheral/tissue-specific metabolism that are at least comparable to CER. This question is challenging to rigorously address in human clinical trials because of issues with adherence to energy intake prescriptions and the lack of a criterion method for measuring the actual free-living intake. In contrast, manipulating the energy intake and determining the actual intake can be accomplished with a high degree of accuracy in animal models.
Alternate day fasting has been the most thoroughly studied IMF protocol in laboratory rodents [15,33,34,35]. A few studies have used a CER protocol for 3–6 consecutive days, followed by a ‘break’ period of ad libitum feeding (e.g., 4 days of a CER followed by 3 days of ad libitum feeding) [15,19]. However, for the purposes of this review, we will only consider preclinical studies of ADF as this protocol is most consistent with the definition of IMF that we have provided here and with previous definitions proposed by Mattson et al. [15,19].
Compared to ad libitum fed animals, ADF appears to improve several circulating and tissue-specific biomarkers associated with the metabolic health status (for reviews, see refs [15,19]). In mice, ADF mitigates the adverse effects of ad libitum high-fat feeding, resulting in a lower fat mass, and thus reducing plasma glucose, insulin, and leptin levels, and improving glucose tolerance [15,19].
To our knowledge, only two preclinical studies (Anson et al. [34] and Mager et al. [33]) have performed head-to-head comparisons of ADF and CER regimens and measured longitudinal weight change and metabolic outcomes. Anson et al. [34] studied mice over a period of ~20 weeks assigned to one of four groups: mice fed ad libitum; mice provided ad libitum access to food every other day (i.e., ADF); mice provided with a limited daily food allotment of 60% of that eaten by the ad libitum fed animals (i.e., CER); and pair-fed mice that were provided a daily food allotment equal to the average daily intake of mice in the ADF group.
The fourth group provided an opportunity to isolate the effects of total calorie intake versus ADF. Over ~20 weeks, the ADF mice compensated for periods of fasting by almost doubling the food intake on fed days, thus gaining weight at rates similar to the ad libitum-fed mice. As expected, the pair-fed mice gained an identical amount of weight to the ADF and ad libitum-fed mice, while the CER mice maintained a significantly lower weight.
Interestingly, despite different body weights and levels of intake, fasting glucose and insulin concentrations were improved to a similar extent in the ADF and CER groups, an effect that was not observed in the pair-fed or ad libitum-fed mice. This is in contrast to a study conducted by Mager et al. [33] that reported unchanged glucose concentrations in Sprague-Dawley rats following a period of ADF, and reduced glucose concentrations in a group of rats following a 40% CER regimen. Similar to the results of Anson et al. [34], the body weight remained lower in the CER rats compared to the rats that received ADF.
An additional study worth noting (Gotthardt et al. [35]) compared ADF combined with either a low- or high-fat diet to groups of mice that were fed low- and high-fat diets ad libitum. This study is relevant to human weight loss because animals were placed into the diet groups after a period of weight gain. C57/BL6 mice were fed a high-fat diet (HFD; 45% fat) ad libitum for 8 weeks to promote an obese phenotype and mice were then divided into four groups that were either maintained for four weeks on an ad libitum high-fat diet (HFD), maintained on an ad libitum low-fat diet, received a high-fat diet every other day (ADF-HFD), or received a 10% low-fat diet every other day (ADF-LFD).
At 4 weeks, body weights were significantly lower in the ADF-HFD group (~13% reduction) and ADF-LFD group (~18% reduction) compared with the HFD group. All three diet groups had a statistically similar energy intake during the intervention. Mice on the ADF-LFD maintained a ~12% higher lean mass over 4 weeks compared to the ad libitum LFD and HFD groups. Only the ADF-LFD group had improved glucose tolerance at 4 weeks compared to the other groups. Although a limitation of the study is that it lacked a diet-specific calorie-restricted group, the results suggest that the dietary macronutrient composition potentially modifies the metabolic response to ADF.
Taken together, the effects of ADF on body weight and glucose (at least in rodents) seem to depend on a number of factors, such as the energy and macronutrient content of the diet. Importantly, in contrast to humans, rodents fed normal chow every other day tend to fully compensate on fed days for the negative energy balance incurred on fast days [34] (see next section). The lack of well-controlled preclinical studies comparing ADF to CER represents a key evidence gap that could be addressed in future studies by including both CER and ADF groups and ideally, animals pair-fed to the IMF group, as was done in the work conducted by Anson et al. [34].
Future studies should also carefully consider how the CER group receives its daily allotment of food. Calorically-restricted rodents tend to eat all of their food as soon as it is made available (e.g., 3–6 h time window) [36]. This is a confounding factor that adds a timing component to the reduction in calories and extends the fasting duration, potentially rendering the CER group indistinguishable from the ADF animals.
Effects of TRF on Body Weight, Body Composition, and Metabolic Outcomes: Evidence from Preclinical Studies
In contrast to IMF, there have been no preclinical studies directly comparing TRF regimens to CER in the context of weight loss, so it is unknown whether this form of IER differentially impacts metabolic responses to weight loss. Therefore, we will briefly address the studies that have examined metabolic responses to TRF compared to an energy-matched ad libitum feeding group (i.e., no time restriction).
Panda et al. [20,21,22] have investigated a diet paradigm where rodents fed an HFD ad libitum are compared to rodents allowed to consume the same number of calories within a restricted time interval of 8–10 h aligned to the active period. In these studies, TRF mice are protected from diet-induced obesity and have increased energy expenditure and fat oxidation. One hypothesized mechanism to explain the attenuated weight gain despite the high-fat feeding in TRF mice appears to be optimizing the alignment of the feeding interval to the appropriate circadian time.
Molecular circadian “clocks” act together to promote energy intake mostly during an organism’s active phase [37]. This circadian control of energy intake involves a primary clock in the suprachiasmatic nuclei of the hypothalamus that synchronizes to the solar light–dark cycle and secondary clocks located in other hypothalamic and brainstem regions. Rhythms in central metabolic hormones, circulating nutrients, and neural inputs transmit timing cues to peripheral organs which allow peripheral organs to anticipate feeding and fasting periods and prime metabolic responses appropriately.
Another mechanism through which TRF may improve body weight regulation is that of an extended fasting duration. Similar to what occurs in IMF, extending the daily fasting duration likely promotes the mobilization of free fatty acids (FFA), increases fat oxidation, and increases the production of ketones [22]. Whether these effects are potentiated when TRF is combined with CER and whether this combination is superior to CER alone are open research questions in both pre-clinical and clinical research.
Finally, one study has suggested that TRF appears to affect host metabolism by altering the gut microbiome to one that is less obesogenic [38]. TRF appears to restore the diurnal variation in several families of bacteria that are involved in nutrient absorption when animals are fed a high-fat diet [39]. In the study by Panda et al. [38], TRF restored diurnal variation in the Lactobacillus and Ruminococcacea families, which have been hypothesized to protect against the metabolic consequences of obesity. TRF mice also excreted more breakdown products of complex carbohydrates (e.g., xylose and galactose), which can only be degraded by gut microflora [39]. These data were interpreted to suggest that complex carbohydrates are less easily absorbed in TRF mice compared to high-fat fed mice.
Current Evidence for IMF as a Weight Loss Strategy: Evidence from Humans? Clinical Studies
We reviewed all randomized weight loss studies performed in adults with overweight or obesity (BMI ≥ 25 kg/m2) that involved a comparison of IMF to CER. Studies included in the review were ≥8 weeks in duration, and the IMF paradigm prescribed ≥60% energy restriction on “fast” days, with intervening “fed” days of ad libitum intake or intake at or above daily energy needs (see Table 1). We did not include studies that utilized ≤60% energy restriction on fast days to remain consistent with prior definitions of IMF in the literature [15].
Interventions of less than 8 weeks were not included because 8 weeks is not a sufficient duration to provide meaningful, clinically relevant information in regard to weight loss. Eleven studies met our criteria and are summarized in Table 1. Because there are no commonly accepted definitions and terminology used to describe the various IMF paradigms, a description of each intervention is provided in the table. Harvie et al., 2011 [40]; Harvie et al., 2013 [41]; Carter et al., 2016 [42]; Carter et al., 2018 [43]; Schübel et al. [44]; Conley et al. [45]; and Sundfør et al. [46] all evaluated various forms of the 2DW IMF diet (either 25% [40,44] or 30% [41] of energy intake (EI) or specific calorie goals on 2 restricted days per week [42,43,46], with no restriction on the other 5 days).
Catenacci et al. [25] evaluated zero-calorie alternate day fasting (100% energy restriction on fast days alternating with ad libitum intake on fed days), while Varady et al. [47], Trepanowski et al. [48], and Hutchison et al. [49] evaluated alternate day modified fasting (ADMF) (25% [47,48] and 37% [49] of energy requirements on fast days alternating with either ad libitum intake on fed days [47] or the provision of 100–145% [48,49] of EI on fed days).
These studies generally enrolled participants who were physically inactive or engaged in light or low amounts of physical activity at the baseline. All studies had a majority of female participants, with the exception of Schübel et al. [44] and Sundfør et al. [46], both of which included 50% males, and Conley et al. [45], which included only older male war veterans. Four studies—Varady et al. [47], Catenacci et al. [25], Trepanowski et al. [48], and Hutchison et al. [49]—provided meals to study participants during some or all of the intervention; all other studies gave energy intake goals but allowed participants to eat their own food.
The level of dietary counseling and contact with dietitians was variable across studies. Studies that provided food generally did not include dietary counseling [25,47], while other studies provided weekly [49] or biweekly [40,41,42,43,44,46] dietary counseling in person or over the phone. A few studies did not provide exercise recommendations during the intervention [42,43,49], but most studies recommended that participants maintain their habitual physical activity levels [25,40,44,46,47,48]. Only the Harvie et al., 2013 [41] study provided the recommendation of gradually increasing the frequency and intensity of exercise. The only study that objectively measured physical activity (Trepanowski et al. [50]) found no change in the number of steps per day in any group.
Overall, the available evidence suggests that IMF paradigms produce equivalent weight loss when compared to CER, with 9 out of 11 studies reviewed showing no significant differences in weight or body fat loss between IMF and CER groups. Our findings are consistent with a recent systematic review and meta-analysis conducted by Harris et al. [51] that included four studies comparing IMF to CER published through November 2015.
We excluded two studies included in that systematic review and meta-analysis (Hill et al. [52] and Viegener et al. [53]) due to the fact that the regimens did not include intervening days of ad libitum food intake, but alternated periods of significant (600–900 kcal/day) with moderate (1200–1500 kcal/day) energy restriction. In the Harris et al. review, the authors found no significant difference between IMF and CER (−1.03 kg, 95% CI −2.46 kg to 0.40 kg).
In the present review, the only studies that showed differences in weight or body fat loss were Harvie et al., 2013 [41] and Hutchison et al. [49]. The Harvie et al., 2013 study included a 2DW IMF regimen which required two consecutive days/week of either a low-carbohydrate diet (70% energy restriction and 40 g carbohydrate) or a less restrictive low-carbohydrate 2DW IMF diet that allowed ad libitum protein and monounsaturated fatty acids. The 2DW IMF diets were compared to an isocaloric 25% CER Mediterranean-type diet.
While there was no significant difference in weight loss between the groups, there was a greater loss of body fat (measured using bioimpedance) with both 2DW regimens compared to CER over 3 months: mean change in body fat was −3.7 kg (95% CI −2.5, −4.9) for the low-carbohydrate 2DW group, −3.7 kg (95% CI −2.8, −4.7) for the low-carbohydrate 2DW plus ad lib protein group, and −2.0 kg (95% CI −1.0, 3.0) for the CER group.
The Hutchison et al. [49] study included an ADMF group that was provided a diet at 70% of the calculated baseline energy requirements per week (ADMF 70), an AMDF diet at 100% of the calculated baseline energy requirements per week (ADMF 100), and a CER group at 70% of the calculated baseline energy requirements daily (CER). The two ADMF groups were provided meals on their fed days (~100% energy requirements for ADMF 70 and ~145% energy requirements for ADMF 100) and were asked to consume breakfast (32% of energy requirements for ADMF 70 and 37% in ADMF 100) before 8 am on 3 nonconsecutive fast days per week, followed by a 24 h fast until 8 am the following day. ADMF 70 produced greater weight loss (−5.4 ± 0.5 kg) and fat loss (−3.9 ± 0.4 kg) compared to both CER (−3.9 ± 0.4 kg; −2.8 ± 0.4 kg) and ADMF 100 (−2.7 ± 0.5 kg; −2.3 ± 0.4 kg). Importantly, both the ADMF 100 and ADMF 70 groups ate less than provided on fed days, resulting in an overall average weekly deficit of ~9% and ~2% more than prescribed, respectively, such that energy restriction in ADMF 70 was greater than CER.
This spontaneous energy restriction on fed days was also observed in Harvie et al., 2013 [41] and Trepanowski et al. [48], and has been hypothesized to be a benefit of IMF [54]. Schubel et al. [44] showed a trend toward greater weight loss with 2DW IMF compared to CER (log relative weight change −7.1 ± 0.7% vs. −5.2 ± 0.6%, p = 0.053). Five studies (Harvie et al., 2013 [41], Catenacci et al. [25], Schubel et al. [44], Trepanowski et al. [48], and Sundfør et al. [46]) included maintenance and/or follow-up phases, with relatively minimal contact with participants for 4–26 weeks. In general, there was no difference in weight regain between IMF and CER groups over these follow-up periods.
Current Evidence for TRF as a Weight Loss Strategy: Evidence from Humans? Clinical Studies
There is some evidence to suggest that the timing of meals may impact weight loss. In two weight-loss interventions, individuals who self-reported consuming more calories in the morning compared to the evening lost more weight, even though both the energy intake and self-reported physical activity were similar [55,56]. In addition, food intake at night (as seen with shift work) is linked to obesity, independent of energy intake [57,58,59].
However, only a few human trials of TRF (eating window ≤8–10 h for ≥8 weeks) have been conducted in individuals with overweight/obesity with weight loss as an outcome, and none of these trials compared TRF to CER. Gill and Panda [32] studied eight overweight men and women with a habitual eating duration >14 h who were asked to restrict EI to a self-selected 10–12 h window. Although participants were not instructed to reduce EI, the restricted eating window resulted in a ~20% reduction in the daily caloric intake estimated using photographic food records.
Subjects lost weight (−3.3 kg, 95% CI −5.6 to −0.9 kg) and maintained the weight loss at 1 year. Interestingly, they also reported subjective improvements in sleep satisfaction, less hunger at bedtime, and increased energy levels. In a study by Gabel et al. [60], 23 obese subjects were asked to restrict feeding (without calorie counting) to an 8 h window (10:00 to 18:00) for 12 weeks, and weight loss was compared to historical controls.
TRF resulted in modest weight loss (−2.6 ± 0.5%) compared to the control (no change). In a study by Antoni et al. [61], 16 men and women (BMI 20–39) were randomized to TRF without energy restriction or control for 10 weeks. The TRF group was asked to delay the first energy intake and advance the last energy intake of the day by 1.5 h each. Participants in the TRF group successfully reduced the eating windows by approximately 4.5 h and reduced the overall energy intake compared to the control group. The TRF group had a significant reduction in body fat percentage (1.9 ± 0.3%), as measured by bioimpedance, but there was no significant change in body weight in either group.
Are the Metabolic Benefits of IMF and TRF in Clinical Studies Solely Due to Caloric Restriction and Weight Loss?
In general, the available evidence suggests that IMF offers little to no advantage over CER for improvements in risk factors for cardiometabolic disease (See Table 2). Small reductions in total cholesterol (TC), low-density lipoprotein (LDL) cholesterol, triglycerides, and fasting glucose and insulin with IMF have been reported in several studies [25,40,41,42,44,47,48,49,50,62], but these changes are generally similar in magnitude to those observed with CER.
Because weight loss was similar in most studies, it appears that the magnitude of weight loss, rather than dietary treatment, is the most important factor driving these changes. Although Hutchison et al. [49] reported that decreases in LDL and total cholesterol were greater with ADMF (after adjusting for weight loss), the magnitude of these differences was small [49]. High-density lipoprotein (HDL) levels remained unchanged in most studies, and when significant changes were observed, the changes were not different from those observed with CER.
Several studies reported improvements in insulin resistance measured using the Homeostatic Model Assessment of Insulin Resistance (HOMA) model [40,41,62] with 2DW IMF, and one study demonstrated greater improvements in insulin sensitivity measured using the euglycemic clamp method with ADMF [49], but ADMF participants lost slightly more weight than those of CER. When observed, the changes in HOMA IR appear to be driven by small decreases in fasting insulin.
However, metabolic measurements were secondary outcomes in most of these studies, and thus, it is likely that these studies were underpowered to detect differences between dietary treatments. Nonetheless, the relatively small changes in these measures suggest that any observed changes or differences between groups have minimal clinical importance. It should be noted that most studies to date have enrolled relatively healthy participants with overweight and obesity.
To our knowledge, only one small study has been performed comparing 2DW IMF to CER in individuals with type 2 diabetes [42]. In that study, HbA1c was significantly reduced after the intervention (−0.5% ± 0.2% in the CER group and −0.3% ± 0.1% in the 2DW group), but did not differ by intervention group. Therefore, whether IMF (2DW or another variation) would have greater benefits in individuals with more adverse metabolic profiles remains an area of future investigation.
An important issue to consider in study design is the timing of measurements relative to the fasting periods. Most studies have obtained samples for metabolic measurements on the day following a fed day. The one exception is the study of Hutchison et al. [49], in which samples were obtained following both a fed and fasted day. Ironically, clamp-measured insulin sensitivity tended to worsen in ADMF when measured the day after a fast.
This effect could possibly be due to the acute elevation in fasting FFA following a fast day, which would be expected to impair insulin sensitivity [63]. Nonetheless, this study highlights some of the challenges of performing laboratory measures in studies comparing IMF to CER. To our knowledge, no study has used ambulatory measures (e.g., continuous glucose monitoring) when comparing IMF to CER. Performing such studies in individuals with impaired fasting glucose or type 2 diabetes is warranted.
It is also worth noting that a majority of the participants in these studies were pre-menopausal women, and there is no indication that attempts were made to account for the potentially confounding effects of phases of the menstrual cycle. Because some of these outcomes are known to vary across phases of the menstrual cycle, it is suggested that this potential confounding effect be controlled in studies where metabolic outcomes are being assessed.
Data regarding the metabolic effects of TRF in humans are limited. The study by Gabel et al. [60] showed a reduction in systolic blood pressure in the TRF group versus controls, but weight loss was greater in the TRF group. There were no differences in the diastolic blood pressure, body composition, cholesterol, homocysteine, fasting glucose, or insulin. Antoni et al. [61] showed a significant diet x group interaction for the change in fasting glucose, but this was driven by elevated glucose levels in the control group at the end of the intervention period. No changes in LDL cholesterol were observed.
Limitations of Previous Clinical Studies and Evidence Gaps
Despite the popularity of IMF and TRF as weight loss strategies, it is notable that only eleven randomized trials have compared IMF with CER, and no randomized trials have compared TRF to CER. In addition, many of the IMF trials provided participants in both IMF and CER arms with some [47,48,49] or all [25] of their food, which significantly limits the applicability to a real-world setting.
Moreover, while current obesity treatment guidelines recommend a comprehensive lifestyle intervention consisting of on-site, high-intensity (≥14 sessions in 6 months) behavioral support provided in individual or group sessions by a trained interventionist [4], none of the studies we reviewed provided behavioral support for IMF meeting these criteria. The duration of the interventions ranged from only 8 to 26 weeks, so the efficacy of IMF over a longer duration, or during weight loss maintenance, has not been well-evaluated.
Finally, none of these studies evaluated the effects of IMF or TRF on appetite (appetite-related hormones or hypothalamic expression of orexigenic peptides), physical activity, or exercise, nor have they assessed sex differences. Clearly, well-designed and longer-term randomized trials are needed to evaluate the effectiveness of IMF compared to the current dietary approach to weight loss (CER), when these approaches are delivered in a real-world setting with guideline-based behavioral support.
While it is well-recognized that adherence to weight loss interventions is the greatest predictor of weight loss success [11], data regarding adherence and acceptability of the IMF and TRF interventions in these studies are limited and variable. In addition, studies present adherence data in variable ways (i.e., percentage vs. absolute number of days adherent to energy restriction, vs. absolute percent energy restriction), which makes direct comparisons across studies difficult. Two studies provided no data regarding adherence to the prescribed diets [42,47]. Most of the IMF studies used seven-day diet records [40,41,44,46,48,49] or diet checklists [43] to assess adherence, with the exception of Catenacci et al. [25] and Hutchison et al. [49], which provided food and assessed adherence via food return.
In a subset of participants, Trepanowski et al. [48] assessed dietary adherence using doubly-labeled water and reported no statistically significant difference in the percent energy restriction between the ADMF and CER by month 6 of the intervention. In other studies, self-reported adherence to the fast days was variable, with the percent of potential restricted days ranging from 43% in Harvie et al. [40] to 97% in Carter et al. [43] at 3 months. Studies with longer-term follow up data showed that self-reported adherence to the fast days dropped to between 21% [44] and 44% [43] at one year.
Two studies provided no data regarding acceptability of the IMF intervention [47,49], but most studies assessed acceptability of the intervention via data on major adverse events and drop-out rates, which were generally found not to differ between groups [25,40,41,42,43,45].
However, Trepanowski et al. [50] reported a higher dropout rate in the ADMF group (38%) vs. CER (29%), with more participants in the ADMF group reporting dissatisfaction with the diet as a reason for withdrawal. Harvie et al. [40] reported that fewer participants in the 2DW IMF group planned to continue the diet at the end of the study compared to the CER group (58% vs. 85%). Sundfør et al. [46] found that participants in the 2DW IMF group reported more hunger, more adverse events, less favorable changes in diet nutritional composition and eating behavior [64], and greater measured weight regain than participants in the CER group.
In the TRF studies, self-reported adherence (number of days adherent to the eating window based on diet diaries) was 62.5% and 80% in studies by Antoni et al. [61] and Gabel et al. [60], respectively. However, in the study by Gill and Panda [32], it was reported that all participants reduced their eating duration (as measured with app-based photographic food records).
However, no data were presented regarding the number or percentage of days that participants adhered to their eating windows. While Gill and Panda [32] reported that all participants expressed an interest in continuing the TRF regimen after the conclusion of the study, participants in the Antoni et al. [61] study rated the regimen with an average difficulty score of 7/10 (10 = extremely difficult to stick to the regimen every day), and 57% felt that they could not have maintained the TRF protocol beyond the 10 week intervention. Therefore, more rigorous, objective methods to assess the adherence and acceptability of IMF and TRF as long-term weight loss regimens are needed, as well as efficacy analyses that take adherence into account.
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6836017/
More information: I. Templeman el al., “A randomized controlled trial to isolate the effects of fasting and energy restriction on weight loss and metabolic health in lean,” Science Translational Medicine (2021). stm.sciencemag.org/lookup/doi/ … scitranslmed.abd8034



{kind=link}