










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The discovery could lead to new methods for classifying and treating patients with this disease.
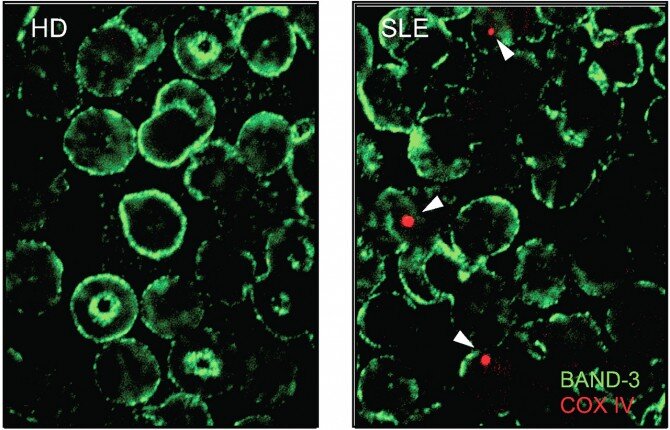
The researchers, who published their findings Aug. 11 in Cell, found that in a number of lupus patients, maturing red blood cells fail to get rid of their mitochondria – tiny molecular reactors that help convert oxygen into chemical energy in most cell types, but are normally excluded from red blood cells.
“Our findings support that red blood cells can play a really important role in driving inflammation in a subgroup of lupus patients,” said senior author Dr. Virginia Pascual, the Drukier Director of the Gale and Ira Drukier Institute for Children’s Health and the Ronay Menschel Professor of Pediatrics at Weill Cornell Medicine. “So this adds a new piece to the lupus puzzle, and could now open the door to new possibilities for therapeutic interventions.”
The lead author of the study was Dr. Simone Caielli, assistant professor of immunology research at the Drukier Institute and the Department of Pediatrics at Weill Cornell Medicine.
Lupus, also known as systemic lupus erythematosus, is a chronic disorder that features intermittent and sometimes debilitating attacks by the immune system on the body’s own healthy tissues, including skin, joints, hair follicles, heart and kidneys. A common underlying factor is the abnormally elevated production of immune-activating proteins called type I interferons.
Treatments, which often are taken long-term and have side effects, aim to suppress immune activity, including interferon-driven inflammation. There is no cure for lupus, and how it arises is still largely mysterious. It is estimated to affect roughly 200,000 people in the United States, the vast majority of whom are female.
Caielli then studied how human red blood cells normally rid themselves of mitochondria as they mature, as prior studies had mainly examined this in mice, and why this process could be defective in lupus patients.
Further experiments revealed how these abnormal red blood cells cause inflammation. In general, as red blood cells age or display signs of damage they are removed by scavenger immune cells called macrophages. Antibodies that bind red blood cells also facilitate their removal.
Once ingested by macrophages, the red blood cells’ mitochondrial DNA stimulates a powerful inflammatory pathway called the cGAS/STING pathway, which in turn drives type I interferon production.
Underlining the relevance of these findings, “those lupus patients with mitochondria-containing red blood cells and evidence of circulating anti-RBC antibodies had higher interferon signatures compared to those who didn’t,” Caielli said.
Systemic lupus erythematosus (SLE) is a multisystem autoimmune connective tissue disorder with a broad spectrum of clinical presentations. The peak age of onset among young women is between the late teens and early 40s with a female to male ratio of 9:1. Those with African or Asian ancestry are more at higher risk of developing the disease and it may be associated with severe organ affection compared to Caucasian patients. SLE may be a life-threatening condition when major organs are affected but more commonly results in chronic debilitating illness.
The cause for SLE has not been identified though environmental factors such as sunlight, hormones, and drugs may precipitate the condition and there is a complex genetic basis [1]. Lupus activity can be measured by many laboratory markers as aberrant production and imbalance of T-helper (Th1/Th2) cell cytokines which have been implicated in the pathogenesis of autoimmunity as IL-18 and IL-10 concentrations are usually significantly elevated in SLE patients and correlated with the SLEDAI score [2].
Red blood cell distribution width (RDW) is a parameter in complete blood counts that is routinely tested to describe the heterogeneity of red blood cells. During the last years, it has been identified as a valuable index to differentiate between thalassemia, megaloblastic anemia and iron deficiency anemia [3].
The researchers have found that RDW is positively correlated with DAS-28, a widely used disease activity tool for rheumatoid arthritis (RA). Increased RDW in RA patients was reported to be associated with risk of cardiovascular diseases. It has been found that increased rate of RDW, as well as RDW changes in the first year after diagnosis, is correlated with a high risk of cardiovascular accident (heart failure, ischemic heart disease, or cerebrovascular accident), and the significant correlation remained after adjusting for sex and age [4].
Lymphopenia has been reported in most of lupus patients throughout the disease course in a previous adult series [5]. SLE activity is not the only cause of lymphopenia; other factors include infections and medications such as corticosteroids and cytotoxic agents which are frequently included in the treatment of SLE. The pathophysiological mechanisms of lymphopenia are complex, including antibodies against CD8+ T lymphocytes, uncontrolled apoptosis, and increased complement mediated cytolysis of T cells, as well as impaired lymphopoiesis and lymphocyte sequestration [6].
Several reports support the notion that abnormal neutrophil subsets and enhanced neutrophil extracellular trap (NET) formation in SLE may play important roles in promoting innate and adaptive aberrant autoimmunity and tissue damage in SLE [7].
Autoimmune diseases as SLE usually consist of inflammatory components. The chronic inflammation, which begins and is triggered by auto-antigen and maintained by both environmental and genetic risk factors, is a common characteristic for all autoimmune diseases [8].
Therefore, inflammatory parameters, such as CRP and ESR, actually useful to assess and follow up the activity of autoimmune diseases; a novel index for inflammation, RDW, may be also useful to assess the activity of autoimmune diseases. Previous studies have shown that RDW was associated with the increased severity of inflammatory bowel disease (IBD), SLE [9, 10], RA [11], and psoriatic arthritis [12, 13]. Another recent study has also concluded that RDW was increased in patients with SLE [14].
A recent Egyptian study had shown that there was a statistically higher RDW in lupus patients with very high activity than those with high activity [15].
In 2013, Vayá et al. [14] firstly reported that SLE patients have higher RDW than healthy controls. Although some of the SLE patients (26/105) had anemia, the SLE patients without anemia also showed higher RDW than healthy controls, indicating that increased RDW in SLE patients is not completely attributed to anemia [14]. Subsequent two studies also revealed that RDW is positively correlated with ESR [16, 17]. Besides, these two studies also it was found that RDW is positively correlated with SLEDAI and anti-dsDNA antibody [14, 16]. RDW also correlates with therapeutic outcome in patients with SLE. Compared to patients with normal RDW, patients with higher RDW have lower response to first line therapy, as well as higher rate of flare during one year follow up [17].
reference link : https://erar.springeropen.com/articles/10.1186/s43166-020-00037-y
More information: Simone Caielli et al, Erythroid mitochondrial retention triggers myeloid-dependent type I interferon in human SLE, Cell (2021). DOI: 10.1016/j.cell.2021.07.021



{kind=link}