











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A set of 7 symptoms, considered together, can be used to maximize detection of COVID-19 in the community, according to a new paper published this week in PLOS Medicine by Marc Chadeau-Hyam and Paul Elliott of Imperial College London, UK, and colleagues.
The rapid detection of SARS-CoV-2 infection in the community is key to ensuring efficient control of transmission. When testing capacity is limited, it is important to use tests in the most efficient way possible, including using the most informative symptoms for test allocation.
In the new study, researchers obtained throat and nose swabs with valid SARS-CoV-2 PCR test results from 1,147,345 volunteers in England aged 5 years and above. The data were collected over 8 testing rounds conducted between June 2020 and January 2021 as part of the REal-time Assessment of Community Transmission-1 (REACT-1) study.
Participants were asked about symptoms they experienced in the week prior to testing.
A model was developed based on the data obtained during rounds 2 to 7, with 7 symptoms selected as jointly positively predictive of PCR positivity:
- loss or change of smell,
- loss or change of taste,
- fever,
- new persistent cough,
- chills,
- appetite loss,
- muscle aches.
The first 4 of those symptoms are currently used in the UK to determine eligibility for community PCR testing.
In round 8 of testing, the resulting model predicted PCR positivity with an area under the curve of 0.77, and testing people in the community with at least 1 of the 7 selected positively predictive symptoms gave sensitivity, specificity, and positive predictive values of 74%, 64%, and 9.7%, respectively.
Modeling suggested that the use of the 7 symptoms identified for PCR test allocation would result in 30% to 40% of symptomatic individuals in England being eligible for a test (versus 10% currently) and, if all those eligible were tested, would result in the detection of 70% to 75% of positive cases.
“In order to improve PCR positivity detection rates and consequently improve control of viral transmission via isolation measures, we would propose to extend the list of symptoms used for triage to all 7 symptoms we identified,” the authors say.
“These findings suggest many people with COVID-19 won’t be getting tested – and therefore won’t be self-isolating – because their symptoms don’t match those used in current public health guidance to help identify infected people,” Elliott adds.
“We understand that there is a need for clear testing criteria, and that including lots of symptoms which are commonly found in other illnesses like seasonal flu could risk people self-isolating unnecessarily.
I hope that our findings on the most informative symptoms mean that the testing program can take advantage of the available evidence, helping to optimize the detection of infected people.”
Discussion
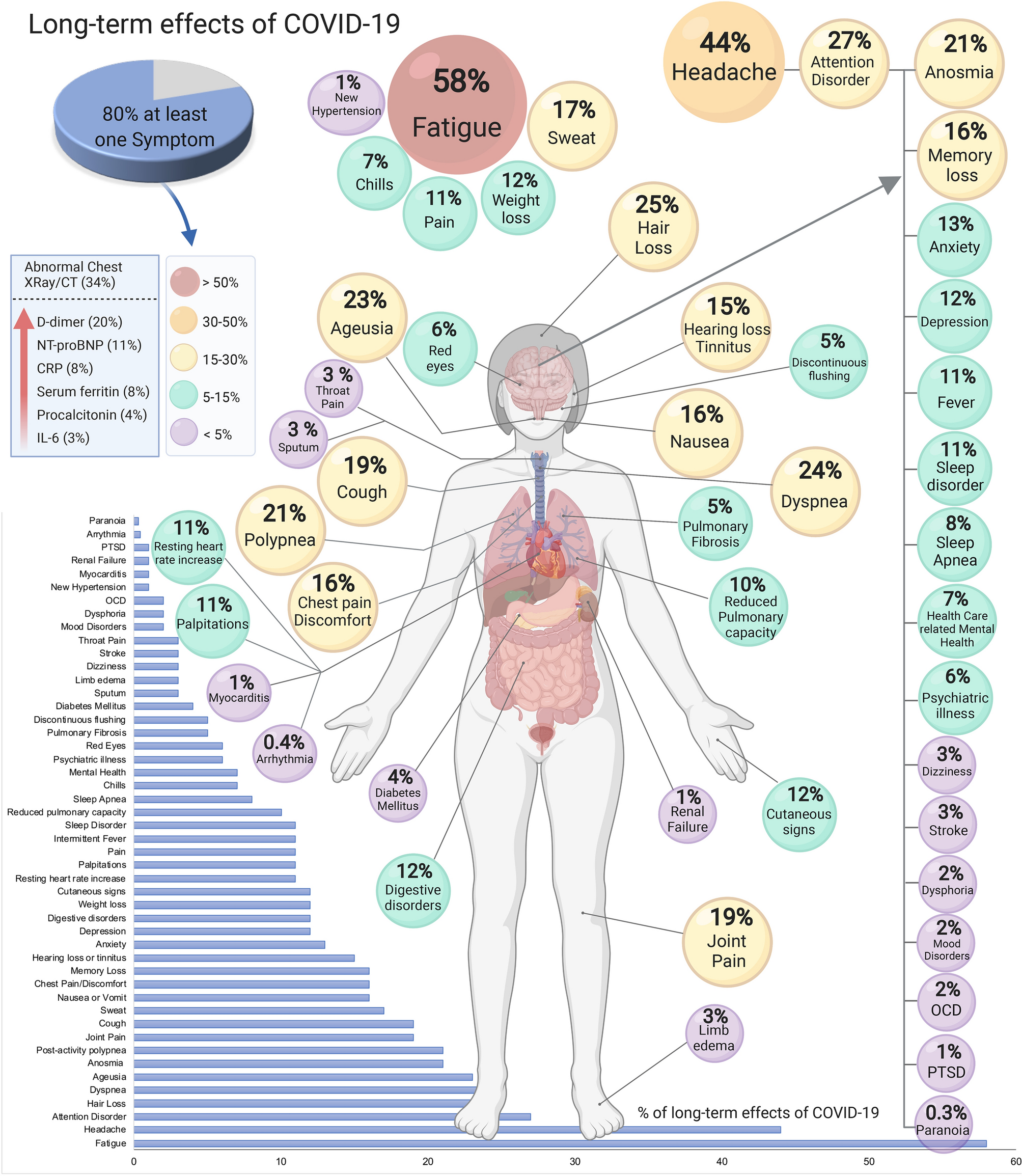
This systematic review and meta-analysis shows that 80% (95% CI 65–92) of individuals with a confirmed COVID-19 diagnosis continue to have at least one overall effect beyond 2 weeks following acute infection. In total, 55 effects, including symptoms, signs, and laboratory parameters, were identified, with fatigue, anosmia, lung dysfunction, abnormal chest X-ray/CT, and neurological disorders being the most common (Table 1, Fig. 2).
Most of the symptoms were similar to the symptomatology developed during the acute phase of COVID-19. However, given that all of the surveys were predefined, there is a possibility that other effects have not yet been identified. In the following paragraphs, we will discuss the most common symptoms to illustrate how complex each one can be. However, further studies are needed to understand each symptom separately and in conjunction with the other symptoms.
The five most common effects were fatigue (58%), headache (44%), attention disorder (27%), hair loss (25%), and dyspnea (24%). The recovery from COVID-19 should be more developed than checking for hospital discharge or testing negative for SARS-CoV-2 or positive for antibodies25.
Fatigue (58%) is the most common symptom of long and acute COVID-1923. It is present even after 100 days of the first symptom of acute COVID-194,23. In addition, there are syndromes such as acute respiratory distress syndrome (ARDS), in which it has been observed that after a year, more than two-thirds of patients reported clinically significant fatigue symptoms26.
The symptoms observed in post-COVID-19 patients, resemble in part the chronic fatigue syndrome (CFS), which includes the presence of severe incapacitating fatigue, pain, neurocognitive disability, compromised sleep, symptoms suggestive of autonomic dysfunction, and worsening of global symptoms following minor increases in physical and/or cognitive activity27,28,29,30,31. Myalgic encephalomyelitis (ME) or CFS is a c
omplex and controversial clinical condition without established causative factors, and 90% of ME/CFS has not been diagnosed32. Possible causes of CFS include viruses, immune dysfunction, endocrine-metabolic dysfunction, and neuropsychiatric factors. The infectious agents related to CFS have been Epstein-Barr virus, cytomegalovirus, enterovirus, and herpesvirus33. It is tempting to speculate that SARS-CoV-2 can be added to the viral agents’ list causing ME/CFS.
Several neuropsychiatric symptoms have been reported, headache (44%), attention disorder (27%), and anosmia (21%). Other symptoms were reported, which were not included in the publications, including brain fog and neuropathy34,35.
The etiology of neuropsychiatric symptoms in COVID-19 patients is complex and multifactorial.
They could be related to the direct effect of the infection, cerebrovascular disease (including hypercoagulation)36, physiological compromise (hypoxia), side effects of medications, and social aspects of having a potentially fatal illness37.
Adults have a double risk of being newly diagnosed with a psychiatric disorder after the COVID-19 diagnosis37, and the most common psychiatric conditions presented were anxiety disorders, insomnia, and dementia. Sleep disturbances might contribute to the presentation of psychiatric disorders38. Prompt diagnosis and intervention of any neuropsychiatric care is recommended for all patients recovering from COVID-19.
An increase in mental health attention models in hospitals and communities is needed during and after the COVID-19 pandemic. Hair loss after COVID-19 could be considered as telogen effluvium, defined by diffuse hair loss after an important systemic stressor or infection.
Premature follicular transitions cause it from the active growth phase (anagen) to the resting phase (telogen). It is a self-limiting condition that lasts approximately 3 months, but it could cause emotional distress39.
Dyspnea and cough were found in 24% and 19% of patients, respectively (Table 2, Fig. 2). In addition, abnormalities in CT lung scans persisted in 35% of patients even after 60–100 days from the initial presentation. In a follow-up study conducted in China among non-critical cases of hospitalized patients with COVID-19, radiographic changes persisted in nearly two-thirds of patients 90 days after discharge40.
Although most of the available studies do not include baseline pulmonary dysfunction or radiographic abnormalities, findings indicate improvement or resolution of abnormal CT findings. Previous data from recovered patients with other viral pneumonia41,42, also found residual radiographic changes. Abnormalities in pulmonary function, such as decreased diffusion capacity for carbon monoxide, were present among 10% of patients in this meta-analysis.
Although these findings are not as high as compared to other available studies of survivors with COVID-19 or SARS, where the estimate of lung dysfunction is 53% and 28% respectively43,44, the reasons behind these differences could be distinct follow-up periods, definitions of pulmonary dysfunction, or characteristics of the patient population. Nevertheless, residual radiographic findings or lung function abnormalities require additional investigation on their clinical relevance and long-term consequences.
The immune-mediated tissue damage in COVID-19 involves cellular and humoral responses, but the immunity to SARS-CoV-2 and the protection to reinfection or a final viral40,45 clearance is unknown. Also, the reason why some patients experience long-term symptoms after COVID-19 is uncertain.
This could be partially explained by host-controlled factors that influence the outcome of the viral infection, including genetic susceptibility, age of the host when infected, dose and route of infection, induction of anti-inflammatory cells and proteins, presence of concurrent infections, past exposure to cross-reactive agents, etc. Whether SARS-CoV-2 can cause substantial tissue damage leading to a chronic form of the disease such as the chronic lesions in convalescence observed in other viruses such as human immunodeficiency virus (HIV), hepatitis C virus (HCV), hepatitis B virus (HBV), and some herpesviruses is still unknown.
One study was excluded because it did not provide a denominator, and therefore it was not possible to estimate the prevalence46. In such a study, the authors performed a survey in a Facebook group of patients who previously had COVID-19 and compared the symptoms of those hospitalized with mild to moderate symptoms. They concluded that both groups had symptoms after 3 months of having COVID-19.
Symptoms that were not mentioned in any of the articles we studied include sudden loss of body weight, ear pain, eye problems, sneezing, cold nose, burning feeling in the trachea, dizziness, heart palpitations, pain/burning feeling in the lungs, pain between the shoulder blades, Sicca syndrome, vertigo, body aches, and confusion3,12.
The results assessed in the present study are in line with the current scientific knowledge on other coronaviruses, such as those producing SARS and MERS, both clinical sharing characteristics with COVID-19, including post symptoms. For example, studies on SARS survivors have shown lung abnormalities months after infection.
After a 1-year follow-up, a study showed that 28% of the survivors presented decreased lung function and pulmonary fibrosis signs44,47,48. In addition, MERS survivors showed pulmonary fibrosis (33%)49. Regarding psychiatric symptoms, a study reported high levels of depression, anxiety, and post-traumatic stress disorder (PTSD)37 in the long term in patients previously infected with other coronaviruses.
To assure that future healthcare providers, researchers, and educators recognize the effects of long-term COVID19 that are sex- and age-specific related, it is essential to classify the groups according to such variables to make better decisions about prevention diagnosis and disease management.
Limitations of this systematic review and meta-analyses include the small sample size for some outcomes, making it difficult to generalize these results to the general population. The variation in the definition of some outcomes and markers and the possibility of bias. For example, several studies that used a self-reported questionnaire could result in reporting bias.
In addition, the studies were very heterogeneous, mainly due to the follow-up time references and the mixture of patients who had moderate and severe COVID-19. All of the studies assessed had performed their internal pre-definition of symptoms, and therefore there is the possibility that essential outcomes were not reported.
Another limitation is that, given that COVID-19 is a new disease, it is impossible to determine how long these effects will last. To decrease heterogeneity and better understand the long-term effects of COVID-19, there is a need for studies to stratify by age, previous comorbidities, the severity of COVID-19 (including asymptomatic), and the duration of each symptom.
To determine whether these long-term effects either complicate previous diseases or continue COVID-19, there is a need for prospective cohort studies. The baseline characteristics should be well established. To obtain more accurate meta-analyses, there is an urgent need to have a standard definition of long-COVID-19. Currently, post-COVID-19 symptoms that develop during or after COVID-19 are defined if they continue for ≥ 12 weeks (“long-COVID-19”), and not explained by an alternative diagnosis2,6,50.
There is a need to standardize biological measures such as peripheral blood markers of genetic, inflammatory, immune, and metabolic function to compare studies. Besides studying pre-defined symptoms and characteristics, an open question should be included. Proper documentation in medical charts by health care providers and the flexibility and collaboration from the patients to report their symptoms are of equal importance.
Table 2 Long-term effects in PASC patients.
| Studies | Cases | Sample size | Prevalence % (95% CI) | |
|---|---|---|---|---|
| Clinical manifestations | ||||
| 1 or > symptoms | 7 | 1403 | 1915 | 80 (65–92) |
| Fatigue | 7 | 1042 | 1892 | 58 (42–73) |
| Headache | 2 | 261 | 579 | 44 (13–78) |
| Attention disorder | 1 | 32 | 120 | 27 (19–36) |
| Hair loss | 2 | 178 | 658 | 25 (17–34) |
| Dyspnea | 9 | 584 | 2130 | 24 (14–36) |
| Ageusia | 4 | 108 | 466 | 23 (14–33) |
| Anosmia | 6 | 210 | 1110 | 21 (12–32) |
| Post-activity polypnea | 1 | 115 | 538 | 21 (18–25) |
| Joint pain | 4 | 191 | 1098 | 19 (7–34) |
| Cough | 7 | 465 | 2108 | 19 (7–34) |
| Sweat | 2 | 144 | 638 | 17 (6–30) |
| Nausea or vomit | 1 | 22 | 141 | 16 (10–23) |
| Chest pain/discomfort | 6 | 264 | 1706 | 16 (10–22) |
| Memory loss | 3 | 320 | 45,186 | 16 (0–55) |
| Hearing loss or tinnitus | 2 | 64 | 425 | 15 (10–20) |
| Anxiety | 4 | 2288 | 45,896 | 13 (3–26) |
| Depression | 4 | 182 | 1501 | 12 (3–23) |
| Digestive disorders | 1 | 15 | 130 | 12 (7–18) |
| Weight loss | 1 | 15 | 130 | 12 (7–18) |
| Cutaneous signs | 1 | 15 | 130 | 12 (7–18) |
| Resting heart rate increase | 1 | 60 | 538 | 11 (9–14) |
| Palpitations | 1 | 14 | 130 | 11 (6–17) |
| General pain | 1 | 17 | 145 | 11 (7–18) |
| Intermittent fever | 1 | 32 | 287 | 11 (8–15) |
| Sleep disorder | 5 | 1036 | 46,070 | 11 (3–24) |
| Reduced pulmonary diffusing capacity | 1 | 14 | 145 | 10 (6–16) |
| Sleep apnea | 1 | 34 | 404 | 8 (6–12) |
| Chills | 2 | 44 | 679 | 7 (1–18) |
| Health care related mental health | 1 | 28 | 404 | 7 (5–10) |
| Psychiatric illness | 1 | 2597 | 44,779 | 6 (6–6) |
| Red eyes | 1 | 8 | 141 | 6 (3–11) |
| Pulmonary fibrosis | 1 | 14 | 287 | 5 (3–8) |
| Discontinuous flushing | 1 | 26 | 538 | 5 (3–7) |
| Diabetes mellitus | 1 | 12 | 287 | 4 (2–7) |
| Sputum | 1 | 16 | 538 | 3 (2–5) |
| Limb edema | 1 | 14 | 538 | 3 (1–4) |
| Dizziness | 1 | 14 | 538 | 3 (1–4) |
| Stroke | 1 | 8 | 287 | 3 (1–5) |
| Throat pain | 1 | 17 | 538 | 3 (2–5) |
| Mood disorders | 1 | 896 | 44,779 | 2 (2–2) |
| Dysphoria | 1 | 9 | 538 | 2 (1–3) |
| Obsessive compulsive disorder (OCD) | 2 | 15 | 579 | 2 (0–8) |
| New hypertension | 1 | 7 | 538 | 1 (1–3) |
| Myocarditis | 1 | 4 | 287 | 1 (0–4) |
| Renal failure | 1 | 4 | 287 | 1 (0–4) |
| Post-traumatic stress disorder (PTSD) | 1 | 2 | 292 | 1 (0–2) |
| Arrythmia | 1 | 1 | 287 | 0.4 (0–2) |
| Paranoia | 1 | 1 | 292 | 0.3 (0–2) |
| Lab tests and other examinations | ||||
| Abnormal chest X-ray/CT | 2 | 188 | 529 | 34 (27–42) |
| Elevated D-dimer | 2 | 134 | 529 | 20 (6–39) |
| Elevated NT-proBNP | 1 | 16 | 145 | 11 (6–17) |
| Elevated C-reactive protein | 2 | 44 | 529 | 8 (5–12) |
| Elevated serum ferritin | 1 | 12 | 145 | 8 (4–14) |
| Elevated procalcitonin | 1 | 6 | 145 | 4 (2–9) |
| Elevated IL-6 | 1 | 4 | 145 | 3 (1–7) |
- Random effects weighted by quality effects model MetaXL for 2 or more studiesC-reactive protein (CRP), Interleukin-6 (IL-6), D-dimer, NT-proBNP, serum ferritin, N-terminal (NT)-pro hormone BNP (NT-proBNP).
Figure 2
reference link: https://www.nature.com/articles/s41598-021-95565-8
More information: Elliott J, Whitaker M, Bodinier B, Eales O, Riley S, Ward H, et al. (2021) Predictive symptoms for COVID-19 in the community: REACT-1 study of over 1 million people. PLoS Med 18(9): e1003777. doi.org/10.1371/journal.pmed.1003777



{kind=link}