








 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The environmental pollutants we consume are probably the reason why some people develop type 1 diabetes. Even low concentrations of such pollutants can result in cells producing less insulin, reveals a new study from the University of Oslo (UiO).
Type 1 diabetes is an autoimmune disease characterize by a destruction of the beta cells of the pancreas that produce insulin. The body’s own defense system makes the mistake of believing that these insulin-producing cells are harmful alien cells that need destroying.
Researchers found more environmental pollutants in the blood of children with type 1 diabetes
In collaboration with the University of Tromsø and several research teams in the U.S., scientists at UiO have studied the environmental pollutants in blood samples from American children and adolescents who have been diagnosed with type 1 diabetes. These were compared with blood samples from a control group not suffering from type 1 diabetes.
“We found that a larger proportion of those with type 1 diabetes had such pollutants in their blood. On average, they also had a higher concentration of several types of environmental pollutants,” says Sophie E. Bresson, Ph.D. student at the Department of Molecular Medicine at the Institute of Basic Medical Sciences at the University of Oslo.
“We found that the beta cells then produced much less insulin, even after only two days and with very low concentrations of environmental pollutants. When the beta cells were exposed to the pollutants for a longer period of time, they died. We therefore believe that environmental pollutants play a role in triggering the onset of type 1 diabetes,” says Bresson.
Bresson, professor Jerome Ruzzin and the research team recently published their findings in an article in the journal Environment International.
Environmental pollutants are a global threat to mankind
Several of the environmental pollutants studied by the research team, such as PCBs and pesticides, were banned 20 years ago by the Stockholm Convention. But these substances are found in food, plastics, paints, building materials, soil and water and are only broken down naturally to a small degree. They may also have been trapped by ice, and when the ice melts due to global warming, the pollutants are released.
In addition, a number of countries that did not sign the Convention still continue to use these substances to prevent insects attacking crops.
“We consume most environmental pollutants via the food we eat. Once these pollutants enter the body, there is unfortunately nothing we can do to eradicate them,” says Bresson.
As part of the study, the researchers obtained blood samples from the US. Could the level of environmental pollutants there differ from that of Norway?
Eat less meat and more lean fish
90% of the environmental pollutants we consume via food come from fish, meat and dairy products, explains professor Jason Matthews at the Department of Nutrition at the University of Oslo.
The scientists point out that fatty fish such as herrings, mackerel, halibut, salmon and trout contain more dioxins and dl-PCB than lean fish filets. Examples of lean fish are coalfish, cod and haddock.
So what can we do to reduce the level of environmental pollutants in our food?
According to the World Health Organization (WHO), the number of people with diabetes worldwide increased from 108 million in 1980 to 422 million in 2014. The latest global estimate indicates that 40% of the 9 million patients diagnosed with T1D are under the age of 40. The prevalence is about 10 times higher in high-income countries compared to low-income countries. The dynamic increase in the number of cases found in children aged 0–4 years is also worrying [1].
The risk of developing the disease in the general population is 6%, while in family members of a person already suffering from it, the risk increases 15 times [2]. Despite many studies, the risk factors of type 1 diabetes in children and adolescents are not fully understood and remain a big challenge for researchers. Previous studies have shown that genetic and environmental factors have a significant impact on the risk of developing T1DM [3,4].
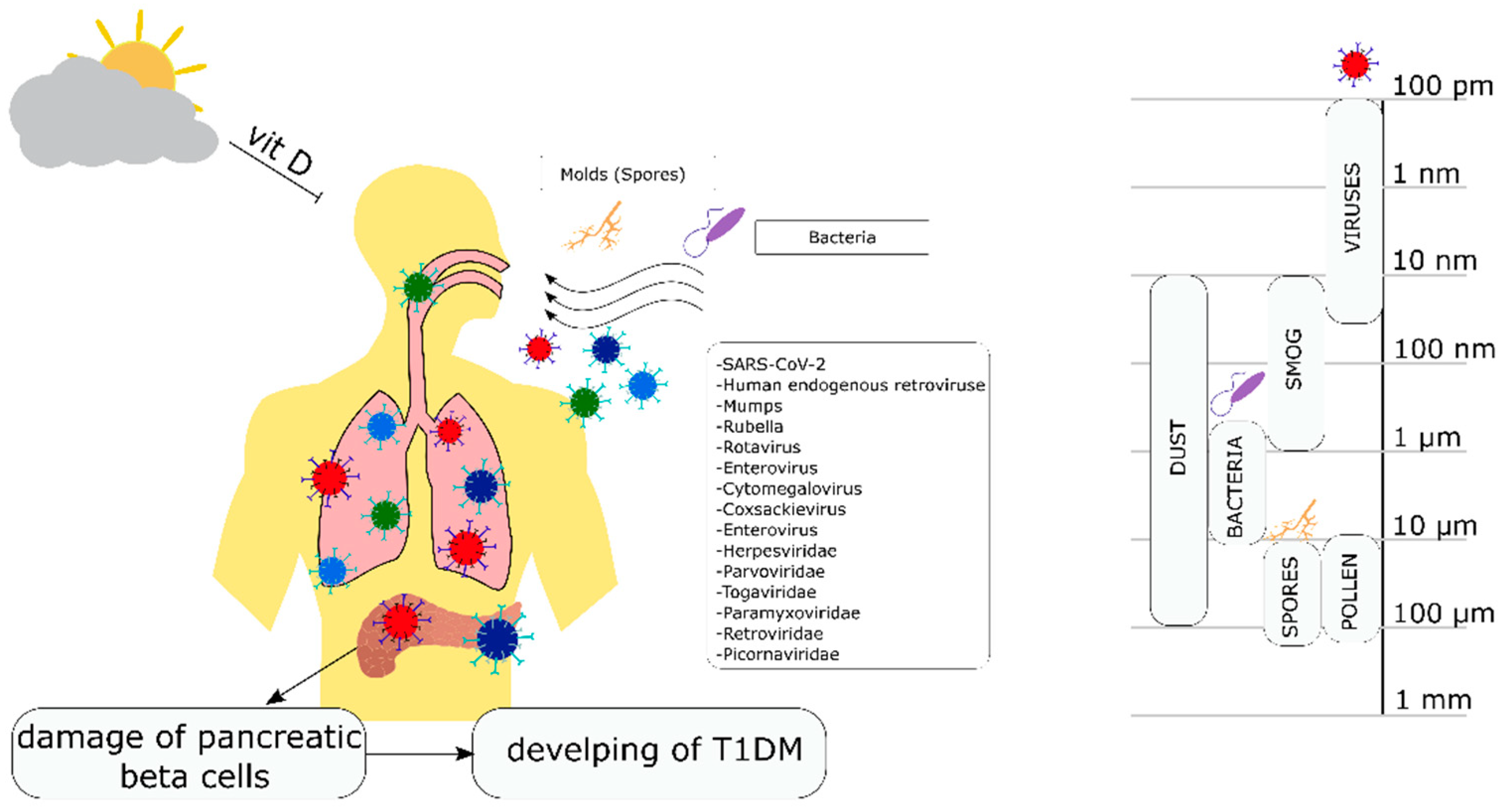
However, in the last few years, new factors have emerged that were not previously considered possible risk factors for the development of T1DM, such as particulate matter (PM) contamination, the microbiome, or SARS-CoV-2 virus infection [5,6,7]. Therefore, an extensive online search for scientific research on factors related to diabetes has been performed for the identification of new factors of unexplained etiology. Three databases were searched: PubMed, Cochrane, and Embase.
The following ‘methodological filter’ was applied when surveying the literature. Firstly, a comprehensive search of peer-reviewed journals, excluding conference papers, was completed based on a wide range of key terms, including the following keywords: type 1 Diabetes Mellitus, T1DM, infection, viral infection, bacterial infection, fungal infection, microbiome, mold, environment, and environmental. Latin names of each of the pathogens found by the use of the previous keywords were also searched.
Secondly, the reference section for each article found was also searched to find additional manuscripts. The search results were limited to the past 11 years of research and discovered 143 manuscripts published between 2011 and 2022. Additionally, 21 manuscripts from between 2000 and 2010 and 3 manuscripts from 1974 to 2000 were referenced for historical reference, as first studies showcasing a certain phenomenon or mechanism.
Eligibility criteria chosen for the study were studies published in the English language between 2000 and 2022 focused on children, adolescents, or pregnant women (due to the T1DM manifesting itself in the first years of life). Exclusion criteria included: primary focus on type 2 diabetes with only a reference to type 1, short reports/conference articles without methodology or results section, studies published in a language other than English. Animal studies and cell-culture studies were only referenced to explain the mechanism behind a particular relation seen in human studies.
1.1. Type 1 Diabetes Mellitus (T1DM)—Etiopathogenesis
During the initiation of the development of type 1 diabetes, under the influence of genetic and environmental factors, a cellular and humoral response is triggered against the β cells of the islets of Langerhans. Their slow destruction is the preclinical stage of diabetes, so-called “prediabetes”.
The first clinical symptoms of the disease appear when 80–90% of pancreatic β-cells are destroyed. They appear suddenly and mainly include pollakiuria and polyuria as well as strongly increased thirst [8]. The symptoms of type 1 diabetes are accompanied by weight loss, fatigue, and weakness of the body.
Ketone bodies may appear in the body as a result of a number of metabolic processes, leading to the development of diabetic ketoacidosis or keto coma, cerebral edema, and in extreme cases, death [8,9].The clinical symptoms of type 1 diabetes mellitus are preceded by a long period of “prediabetes”, characterized by the presence of anti-islanding antibodies and impaired insulin and C-peptide secretion.
During the “prediabetes” period, those antibodies detected in the blood serum are one of the markers for “predicting” the development of T1DM. These include antibodies against islet cells (ICA), insulin (IAA), and/or glutamic acid decarboxylase (GAD; an enzyme present in pancreatic β cells, participating in insulin secretion), against protein tyrosine phosphatase (anti-IA-2) and zinc transporting protein (ZnP8) [10].
Clinical symptoms of T1DM are preceded by disturbances in insulin and C-peptide secretion [10]. What is more, in patients with freshly diagnosed T1DM, autoreactive T lymphocytes directed against specific autoantigens, which are considered a cell-damaging factor, may appear in addition to serum antibodies [11]. In the course of viral infections or due to other environmental factors, autoreactive T cells can be activated and damage the β-cells of the pancreas [11,12]. β-cells are destroyed by apoptosis (programmed cell death) and necrosis.
Both processes may involve cellular immunity, including lymphocyte T subpopulations (Th1 and Th2 helper and CD8 + cytotoxic cells), NK cells, monocytes/macrophages, cytokines, and other inflammatory factors [13,14]. According to the current knowledge, it is assumed that specifically activated Th1 lymphocytes, which recognize pancreatic autoantigens, induce migration of specific as well as non-specific mononuclear cells through cytokine secretion.
These cells also produce pro-inflammatory cytokines that intensify the course of the reaction and, at the same time, affect β cells by stimulating the release of free radicals and nitric oxide [12]. The period in which the pancreatic islets are infiltrated by mononuclear cells, e.g., macrophages, T lymphocytes, and Natural Keller (NK) cells, is called perinsulitis [15].
Mononuclear cells and the release of inflammatory agents damage the β-cells of the pancreas by triggering the apoptosis process and by the infiltration of inflammatory cells called insulitis [16,17]. In the pathogenesis of T1DM, attention is also paid to the imbalance between the activity of the Th1 and Th2 lymphocyte subpopulations.
Th1 lymphocytes present with features of autoreactive cells—they have the ability to secrete pro-inflammatory cytokines, e.g., IL-1, IL-6, IL-12, or TNFα, as well as activate macrophages, cytotoxic CD8 + lymphocytes and NK cells [18,19]. On the other hand, Th2 lymphocytes also act as regulatory cells—they can inhibit Th1 lymphocytes and induce a humoral response.
In prediabetes patients, as well as in patients with newly diagnosed diabetes, there is an increased concentration of pro-inflammatory cytokines—the Th1 profile [20]. Studies on anti-inflammatory cytokines—Th2 profile of IL-4, IL-10, IL-13 have shown that the ability to secrete these cytokines may correlate with a reduced risk of developing diabetes [10,16,20]. On the other hand, under the influence of pro-inflammatory factors (IL-1, TNF-α, and IFN-γ), the production of NO intensifies, which in turn may lead to apoptosis of pancreatic β-cells [21,22].
1.2. Genetic Predisposition as an Etiological Factor of T1DM
T1DM is a multifactorial disease. Susceptibility to T1DM is hereditary, and the mode of inheritance is complex and still not fully understood [9]. The risk of developing T1DM under the age of 20 is 1:300 in families without genetic burden, 1:50 in the case of a child whose mother has T1DM, and 1:15 in the case of T1DM in the child’s father.
A family history of diabetes is an important indicator of the risk of the disease in children because it shows the coexistence of pro-diabetogenic factors, both genetic and environmental [23,24]. The main genes predisposing to the development of T1DM are located within the genes of the HLA system on chromosome 6, although other genes may also be involved [25,26].
The genetic factor plays a significant role in the development of T1DM, which has been proven by studies on twins. In identical twins, the risk of diabetes is 50% compared to fraternal twins, where the risk ranges from 5 to 13% [27,28]. A study by Siewko et al. showed that autoimmune markers were detected in the serum in more than 30% of first-degree relatives of diabetic patients.
It was also revealed that these people, despite normal glucose tolerance, significantly decreased beta-cell secretory reserve and decreased insulin sensitivity [29].The genetic predisposition to develop T1DM is associated with the HLA gene complex located in chromosome 6p21 (IDDM1), which has been known since the 1970s. [30]. The associated HLA DR3 and DR4 haplotypes cause severe susceptibility [31,32]. In 90% of the Caucasian population, diabetes is strongly associated with DR3 antigens (DRB1 * 03: 01-DQB1 * 02: 01) and DR4 (DRB1 * 04: 01-DQB1 * 03: 02).
In contrast, in Japan and most other East Asian populations, TDM1 diabetes is associated with DR4 haplotypes (DRB1 * 04: haplotypes 05-DQB1 * 04: 01) and DR9 (DRB1 * 09: 01-DQB1 * 03: 03) [33]. In Brazil, the most common haplotype is HLA-DRB1 * 03: 01 ~ DQA1 * 05: 01 g ~ DQB1 * 02: 01 [32].Analysis of the human genome by a mapping technique also identified other loci attributed to the presence of T1DM. One such site is the region associated with the insulin gene, which is located on the short arm of chromosome 11 (11p15.5) and is responsible for 10% inheritance of T1DM [34]. So far, the risk of T1DM has been associated with nearly 30 different gene loci. However, few of the loci studied have been linked to specific genes [34]. Research on the connection of genes with a genetic predisposition is still ongoing. Despite many years of research, the actual role of most of these genes in the pathogenesis of T1DM remains unclear [35,36,37]. On the other hand, more and more studies indicate the role of environmental factors in the development and/or progression of T1DM [6,38,39,40,41,42].
1.3. The Accelerator Hypothesis, the β-Cell “Overload” and the Risk of Developing Diabetes
Genetic inheritance is linked to various hypotheses with environmental factors and is associated with multiple mechanisms [43,44,45,46,47,48]. One of these hypotheses is the “Accelerator Hypothesis”, which points to the role of adipose tissue metabolism in the process of autoimmunity. Proposed by Kibirige et al. and based on epidemic logical data, the hypothesis suggests that excess body fat and insulin resistance may be accelerators, i.e., they may accelerate the destruction of β-cells (by the primary or secondary effect on their apoptosis) and, consequently, initiate the autoimmune process in genetically predisposed people [49].
Moreover, it was shown that low physical activity had been shown to initiate insulin resistance leading to excessive β-cell function [50]. The increasingly ‘obesogenic’ environment which promotes insulin resistance could account for the rising incidence of type 1 diabetes [51].The second known hypothesis is the so-called “overload of the β cell” theory formulated by Dahquist G., which is a complement to the accelerator hypothesis [52].
It assumes the influence of several environmental factors on the increase of β-cells susceptibility to necrosis and/or apoptosis, including factors such as overfeeding the fetus and children. Interestingly, recent research has shown that excessive weight gain in the first years of life causes growth and the accumulation of both fat and muscle cells [53]. On the other hand, recent research does not corroborate an increase in type 1 incidence in the pediatric population being associated with younger age of diagnosis and higher BMI-SDS [54]. The data does not support the ‘accelerator hypothesis’. There was no sign of excessive weight gain before the manifestation of type 1 diabetes. The authors suggest that discrepant results from other studies could be due to non-age-adjusted controls [55].
reference link: https://www.mdpi.com/2079-7737/11/4/608/htm
reference link : More information: Sophie E. Bresson et al, Associations between persistent organic pollutants and type 1 diabetes in youth, Environment International (2022). DOI: 10.1016/j.envint.2022.107175



{kind=link}