











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Idiopathic hypereosinophilic syndrome (HES) is a rare and potentially lethal disorder characterized by persistently elevated eosinophil counts without any underlying causes.
Hypereosinophilic syndrome happens when eosinophilia accelerates, speeding up eosinophil production and increasing the number of eosinophils. This eosinophil overload can damage the organs, including the heart, lungs, skin and nervous system. Left untreated, hypereosinophilic syndrome can be life-threatening. Fortunately, prompt diagnosis and treatment mean more than 80% of those diagnosed with hypereosinophilic syndrome are alive five years after diagnosis.
https://jmedicalcasereports.biomedcentral.com/articles/10.1186/s13256-022-03543-z
Case presentation
A 48-year-old Japanese woman with a recent history of COVID-19 presented with fatigue, palpitation, back pain, and abdominal discomfort, and loss of appetite 3 days after the quarantine period. She had a positive polymerase chain reaction (PCR) test for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) 5 weeks before her visit, which was detected because she was in close contact with her husband who had COVID-19. She remained asymptomatic for 10 days during the COVID-19 isolation period; however, she began to feel general fatigue and back pain 3 days later. She complained of bilateral upper back pain without irradiation.
This condition was moderate in severity and was not relieved by rest. Her appetite was hindered owing to abdominal bloating, frequent belching, and constipation. She lost 4 kg of weight in 3 weeks and was admitted to the hospital. She had a history of bronchial asthma, allergic rhinitis, and oral allergy syndrome to melon and watermelon with eosinophilia. Absolute eosinophil count was 1645/µL, 26% of white blood cell count, on the laboratory data 1 year before.
Although she had been experiencing numbness in her bilateral hands for 3 months, she did not take it seriously, assuming it was due to her daily manual labor. A month before, she had been diagnosed with carpal tunnel syndrome at another clinic. She was given a budesonide/formoterol inhaler, montelukast, theophylline, mirogabalin, and methyl-cobalamin, which is conventionally prescribed for peripheral neuropathy in Japan.
Her blood pressure was 142/115 mmHg, pulse rate was 113 beats per minute, body temperature was 36.3 °C, respiratory rate was 18 breaths per minute, and oxygen saturation was 99% on ambient air. Physical examination revealed slight inspiratory fine crackles on the left chest but no wheezing. Cardiac auscultation revealed no gallops or murmurs, and cervical inspection showed no jugular venous distention. A pale rash was observed, which changed to palpable erythema on the entire back (Fig. 1) in a week.
No eruptions were observed on the chest, abdomen, and extremities. She presented with sensory disturbances in the bilateral median nerve territories, as well as a positive Phalen test and Tinel sign. Lower limb hypoesthesia and weakness of the left tibialis anterior muscle were observed. Generalized hyperreflexia was also observed, but it was not accompanied by pathological reflexes. The eyes, nose, thyroid gland, abdomen, and superficial lymph nodes showed no abnormalities.

Laboratory results revealed hypereosinophilia with an absolute eosinophil count of 11,956/µL, as well as elevated immunoglobulin E (IgE) level, positive rheumatoid factor, and negative anti-neutrophil cytoplasmic antibody (ANCA). Liver and kidney function tests were normal, and urinalysis revealed no proteinuria, hematuria, or cast. Table 1 summarizes the major laboratory data.
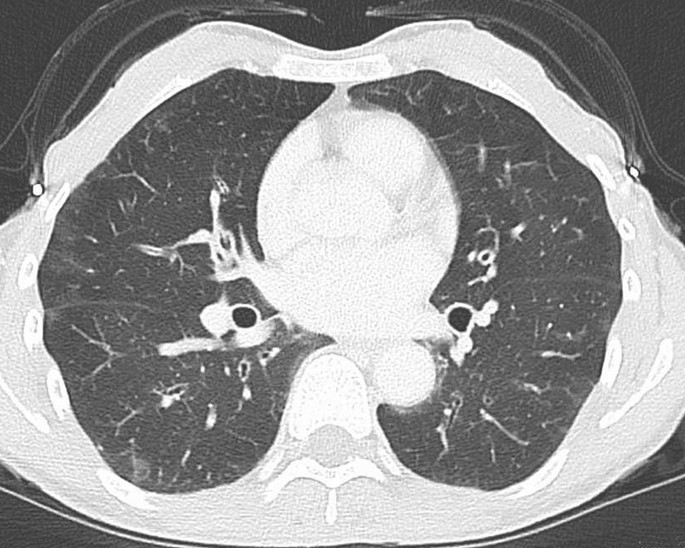
Electrocardiography revealed sinus tachycardia. Left ventricular ejection fraction was normal, and there was no evidence of ventricular hypertrophy, dilation including the right ventricle, valvular abnormality, or pericardial effusion on echocardiography. Bilateral patchy ground-glass opacity areas were observed on chest computed tomography (CT), which were indistinguishable from the residual COVID-19 lesion (Fig. 2). There was no evidence of pulmonary embolism, or abnormal findings of abdomen on the contrast-enhanced CT.
A nerve conduction study revealed signs of axonal injury, namely reduced amplitudes of sensory nerve action potentials and normal sensory nerve conduction velocities in the bilateral median nerve and the right-sided ulnar and sural nerves. Normal distal latencies on the bilateral median nerves ruled out carpal tunnel syndrome.
The physical examination findings, including anterior tibialis muscle weakness, indicated a mononeuritis multiplex pattern. Bone marrow aspiration demonstrated normal cellularity with increased eosinophil count of 65.2% without dysplasia, and FIP1L1–PDGFRA fusion gene was negative on fluorescence in situ hybridization.
A biopsy of the skin lesion showed perivascular and perineural eosinophilic infiltration and degranulation. There was no evidence of necrotizing small-vessel vasculitis or extravascular granulomas. Although the patient presented abdominal discomfort, there were no abnormal findings in gastrointestinal investigations with upper endoscopy and
As helminthic infection is rare in this region, these findings could be explained by either idiopathic HES or ANCA-negative, nonvasculitic EGPA. We decided to treat the patient with glucocorticoids, which is the common first-line drug for both diseases and evaluated the diagnosis from the therapeutic course because we could not distinguish these two at this point.
Prednisolone at 1 mg/kg was started, which significantly improved the systemic symptoms. Back pain, tachycardia, abdominal discomfort, and appetite loss subsided within a few days, and the absolute eosinophilic count dropped to 50/µL. In 3 weeks, the erythema on the back faded and completely disappeared. Prednisolone was tapered from weekly to biweekly, with outpatient evaluation for her symptoms and eosinophil count.
Follow-up echocardiographic findings were normal, and weakness of the left tibialis anterior muscle improved to normal strength in 3 months. The numbness in the hands improved but fluctuated in a low grade through the course. After 8 months of tapering and discontinuing prednisolone, asthmatic symptoms recurred with mild eosinophilia despite continued use of budesonide/formoterol inhalation, montelukast, and theophylline. After resumption of 30 mg of prednisolone for 5 days, nighttime cough and wheezing disappeared, and absolute eosinophil count was normalized. Since the patient responded well to maintenance dose of prednisolone 5 mg/day thereafter, tapering rate was slowed down by monitoring symptoms and eosinophil count.
. . . .
It should be noted that a few past studies have suggested that COVID-19 may trigger the development of some autoimmune and/or autoinflammatory dysregulation in genetically predisposed patients.
https://pubmed.ncbi.nlm.nih.gov/33080459/
https://pubmed.ncbi.nlm.nih.gov/32220633/
https://pubmed.ncbi.nlm.nih.gov/33842894/
https://pubmed.ncbi.nlm.nih.gov/33640999/
There have been three other documented cases of eosinophilic granulomatosis with polyangiitis (EGPA) and hypereosinophilic syndrome (HES) following the occurrence of COVID-19.
https://pubmed.ncbi.nlm.nih.gov/33506754/
https://pubmed.ncbi.nlm.nih.gov/33106869/
https://pubmed.ncbi.nlm.nih.gov/34160722/



{kind=link}