









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A clinical review, published today for the BMJ, provides new interim advice for doctors and clinicians in prescribing cannabis-based products and cannabinoids to treat certain conditions.
Since a policy change in November 2018, specialist doctors registered with the General Medical Council (GMC), have been permitted to prescribe new medicines which derive from cannabis.
Yet, research into these products has, to date, been limited creating an ‘information vacuum’ about these medicines, their benefits or harms.
A new review authored by leading scientists and clinicians from the University of Bath and University College London (UCL) points to the array of different cannabis-based products and cannabinoids available, and a clear need to educate both patients and clinicians into what these different products do and how they might help.
In particular, it points to important differences between products containing THC (the main psychoactive and intoxicating constituent of cannabis) versus CBD (the non-intoxicating element).
Although in certain medicines CBD and THC are combined for clinical benefit, in others these components can work independently, playing different roles in improving certain symptoms.
For example, several studies have found that a combination of THC and CBD can alleviate symptoms of chronic pain, while CBD alone may be effective for treatment-resistant epilepsy.
By contrast THC alone may be effective for treating nausea and vomiting caused by chemotherapy. THC and CBD are both ‘cannabinoids‘ that act in different ways on the body’s endogenous cannabinoid system.
The cannabis plant produces over 144 different cannabinoids such as THC or CBD.
Some medicinal products contain THC and/or CBD derived from the cannabis plant, while others contain synthetically produced cannabinoids.
CBD is also available in non-medicinal products such as oils and tinctures.
Lead author, Dr. Tom Freeman of the University of Bath’s Addiction and Mental Health Group explains:
“In this complex and rapidly evolving field, there are several different cannabis-based and cannabinoid medicinal products.
These differ in their THC and CBD content, who can prescribe them, and the conditions they may be used to treat.
Here we provide an update for clinicians in advance of forthcoming NICE guidelines.
“A key message is that CBD products widely sold online and in health food shops lack quality standards and should not be treated as medicinal products.”
Research on cannabis was previously restricted because it was listed in Schedule 1, implying that it had no medical value.
Cannabis was recently moved to Schedule 2 in the UK.
The differences between the cannabinoids.
To begin, it’s important to know that when we talk about CBD, hemp oil, marijuana, and THC, we’re really talking about the cannabis plant and its derivates.
Because while there are important legal differences between hemp and marijuana, when it comes to the science, hemp and marijuana are actually just two versions of the cannabis plant.
This causes a lot of confusion (and it is, admittedly, confusing!), but it’s important to know that when we say cannabis, it applies to both marijuana and hemp.
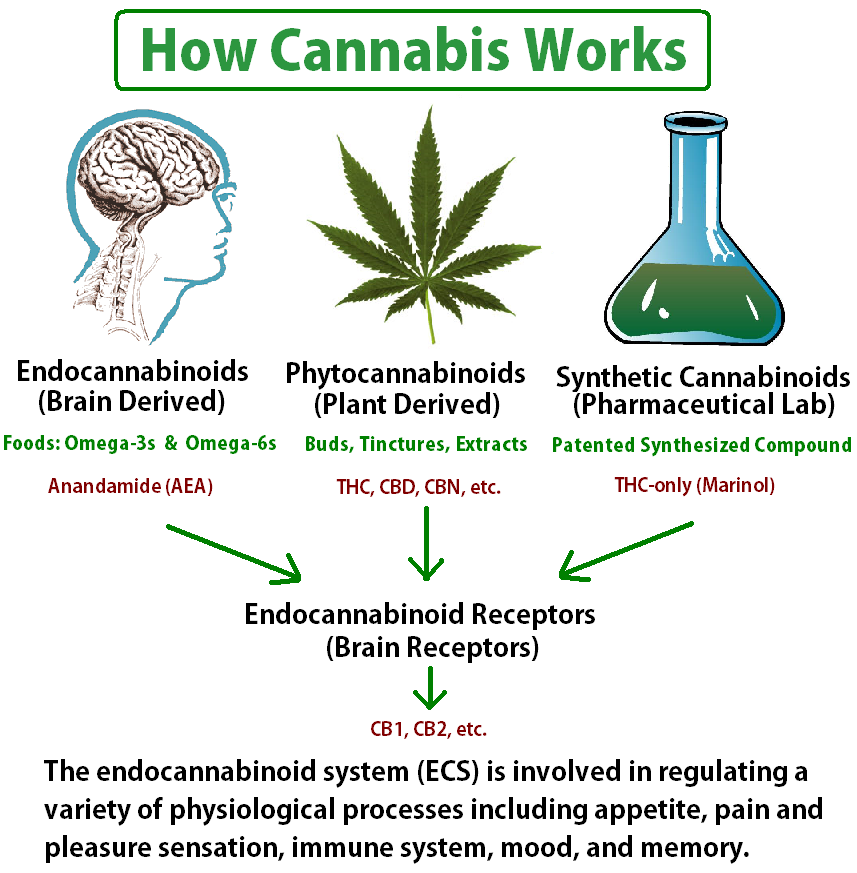
Cannabinoid is a name that describes a ground of similar compounds that are found in the body (called endocannabinoids), found naturally in plants (called phytocannabinoids), and even made in a lab (in this case they’re called synthetic cannabinoids).
Cannabinoids interact with a larger system in the body called the endocannabinoid system(ECS), which is often described as a major regulatory system.
The ECS is responsible for the side effects (good and bad) of using cannabis – whether that be in the form of hemp oil, CBD oil, or smoking marijuana.
The endocannabinoid system is composed of the endocannabinoids that the body produces naturally and also a family of receptors called cannabinoid receptors.
The two cannabinoid receptors to know about are CB1 and CB2, and they explain in large part why cannabis has so many healing properties and also why THC causes intoxication while CBD does not.

CBD versus THC.
Speaking of CBD and THC, it’s important to know the difference between these two distinct compounds that interact with the body in very different ways.
THC directly binds to CB1 receptors in the body, which are mainly found in the brain and nervous system.
Once you know this, it’s no big surprise to learn that this CB1 receptor activation is responsible for the “high” from smoking cannabis and that CBD does not directly bind with that receptor.
Instead, CBD interacts with other receptors and pathways in the body that explain many of its specific health benefits.
CBD and THC have been described as “sister molecules” and one of the most interesting aspects of cannabinoid science is the “entourage effect,” which says that cannabinoids are more effective together than they are alone in isolated preparations.
This is part of the reason why when you’re looking for cannabis products, experts recommend full-spectrum products (which include some of the other cannabinoids and terpenes of the plant) and to steer clear of isolates, which only contain the single compound and are generally less effective and more difficult to dose.
CBN, THCA, CBDA, and other cannabinoids.
CBD and THC get a lot of the fame, but there are actually a bunch of cannabinoids worth learning about.
Cannabinol (CBN), which was actually the first cannabinoid to be discovered, is often used specifically for sleep.
In addition, two compounds called tetrahydrocannabinolic acid (THCA) cannabidiolic acid (CBDA) – known as the “parent” molecules of CBD and THC – seem to have their own set of healing properties and are both non-psychoactive.
Other cannabinoids include cannabigerol (CBG), cannabichromene (CBC), and tetrahydrocannabivarin (THCV), which are all of interest to doctors and researchers for their specific health benefits.
Unfortunately, many of these cannabinoids have barely been studied.
The benefits of cannabinoids.
Cannabinoids have a wide range of health benefits, ranging from THC’s pain-relieving qualities to CBD’s anti-anxiety properties.
Other areas of research include cannabinoid therapy for PTSD, seizures, depression and anxiety, cancer and cancer-treatment-related symptoms, pain, and addiction (especially to opioids).
Most of these areas of research are in the preliminary stages, although a CBD-derived pharmaceutical drug was just approved by the FDA for seizure disorders, and THC-based drugs have been available for pain and a few other conditions for quite some time.
As research continues, we’ll better understand cannabis and the health benefits of specific cannabinoids.
Unfortunately, though, the way current laws are set up, it’s extremely difficult to get approval to study cannabis and even more difficult and time-intensive to get high-quality plant materials to use in research.
Hopefully, as more patients ask their doctors about cannabis-based therapies and more states approve recreational and medicinal marijuana, that will change.
CBD oil versus hemp oil.

The difference between CBD oil and hemp oil (not to be confused with hemp seed oil, which is made from the sterilized seeds of the plant and doesn’t have significant cannabinoid content) can also be a source of confusion.
Essentially, hemp oil is an extract from the whole plant and will contain a variety of cannabinoids – including CBD.
In fact, many products that are marketed as CBD oil are actually CBD-rich hemp oils. CBD is available on its own (in a form commonly referred to as a CBD isolate), but hemp and cannabis experts don’t typically recommend CBD isolates, as you miss out on the beneficial entourage effect.
Dr. Freeman adds: “Research on unlicensed cannabis products has been limited to date.
The rescheduling of cannabis and allocation of dedicated UK research funding will improve the evidence we have to guide clinical decision-making.”
Co-author, Dr. Michael Bloomfield Head of Translational Psychiatry at University College London (UCL) added:
“There have been leaps and bounds in our scientific knowledge in recent years, which combined with confusing claims about the medicinal uses of these drugs can be potentially perplexing for doctors and patients.
We hope that our new guidance is helpful to doctors and patients worldwide. Much more research is needed into this new class of medicine.”
Co-author Dr. Chandni Hindocha of the Clinical Psychopharmacology Unit at UCL added:
“Resources must be made available to update and educate clinicians about cannabis and cannabinoid based medicines.
We would like to encourage doctors to maintain a compassionate and evidence-based approach when engaging with their patients in this rapidly developing field, in order to provide the best standard of care.”
More information: Tom P Freeman et al, Medicinal use of cannabis based products and cannabinoids, BMJ (2019). DOI: 10.1136/bmj.l1141
Journal information:British Medical Journal (BMJ)Provided by University of Bath



{kind=link}