










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Breast cancer medicines may force some cancer cells into ‘sleeper mode’, allowing them to potentially come back to life years after initial treatment.
These are the early-stage findings from scientists at Imperial College London, who studied human breast cancer cells in the laboratory.
The team, who studied a group of breast cancer drugs called hormone treatments, say their research opens avenues for finding ways of keeping the cancer cells dormant for longer, or even potentially finding a way of awakening the cells so they can then be killed by the treatment.
Dr. Luca Magnani, lead author of the study from Imperial’s Department of Surgery and Cancer said:
“For a long time scientists have debated whether hormone therapies – which are a very effective treatment and save millions of lives – work by killing breast cancer cells or whether the drugs flip them into a dormant ‘sleeper’ state.
“This is an important question as hormone treatments are used on the majority of breast cancers.
Our findings suggest the drugs may actually kill some cells and switch others into this sleeper state.
If we can unlock the secrets of these dormant cells, we may be able to find a way of preventing cancer coming back, either by holding the cells in permanent sleep mode, or be waking them up and killing them.”
In the study, published in the journal Nature Communications and funded by Cancer Research UK and the NIHR Imperial Biomedical Research Centre, the team studied around 50,000 human breast cancer single cells in the lab, and found that treating them with hormone treatment exposed a small proportion of them as being in a dormant state.
The team say the ‘sleeper cells’ may also provide clues as to why some breast cancer cells become resistant to treatment, causing a patient’s drugs to stop working, and their cancer to return.
Hormone therapies are used to treat a type of breast cancer called oestrogen-receptor positive.
These make up over 70 per cent of all breast cancers, and are fuelled by the hormone oestrogen.
These cancers are usually treated with surgery to remove the tumour, followed by a course of targeted hormone therapy – usually either aromatase inhibitors or tamoxifen, which target oestrogen receptors.
However, around 30 per cent of breast cancer patients taking hormone therapies see their cancer eventually return – sometimes as long as 20 years after treatment.
This returning cancer is usually metastatic, meaning it has spread around the body, and the tumours are often now resistant to medication.
Previous work by the same team has investigated why breast cancer cells become resistant to hormone treatment, with findings suggesting cells can make their own ‘fuel’, allowing them to avoid being ‘starved’ by cancer treatment.
This new research provides another piece in the puzzle, explained Dr. Iros Barozzi, co-author of the study, also from the Department of Surgery and Cancer:
‘These sleeper cells seem to be an intermediate stage to the cells becoming resistant to the cancer drugs.
The findings also suggest the drugs actually trigger the cancer cells to enter this sleeper state.”
The research also revealed cells in this dormant sleeper state were more likely to spread around the body, explained Dr. Sung Pil Hong, study co-author from Imperial:
“Our experiments suggest these sleeper cells are more likely to travel around the body. They could then ‘awaken’ once in other organs of the body, and cause secondary cancers.
However, we still don’t know how these cells switch themselves into sleep mode—and what would cause them to wake up.
These are questions that need to be addressed with further research.”
The team added that hormone therapies remain one of the most effective treatments against breast cancer, and that further patient research will explore whether taking hormone therapies for longer after initial cancer treatment could prevent cancer cells from waking from their sleeping state.
Dr. Rachel Shaw from Cancer Research UK, said: “Although treatments for breast cancer are usually successful, cancer returns for some women, often bringing with it a poorer prognosis.
Figuring out why breast cancer sometimes comes back is essential to help us develop better treatments and prevent this from happening.
This study highlights a key route researchers can now explore to tackle ‘sleeping’ cancer cells that can wake up years after treatment, which could potentially save the lives of many more women with the disease.”
Breast cancer is a disease in which malignant (cancer) cells form in the tissues of the breast.
The breast is made up of lobes and ducts. Each breast has 15 to 20 sections called lobes. Each lobe has many smaller sections called lobules. Lobules end in dozens of tiny bulbs that can make milk. The lobes, lobules, and bulbs are linked by thin tubes called ducts.

Anatomy of the female breast. The nipple and areola are shown on the outside of the breast. The lymph nodes, lobes, lobules, ducts, and other parts of the inside of the breast are also shown.
Each breast also has blood vessels and lymph vessels.
The lymph vessels carry an almost colorless, watery fluid called lymph. Lymph vessels carry lymph between lymph nodes.
Lymph nodes are small, bean-shaped structures found throughout the body. They filter lymph and store white blood cells that help fight infectionand disease. Groups of lymph nodes are found near the breast in the axilla (under the arm), above thecollarbone, and in the chest.
The most common type of breast cancer is ductal carcinoma, which begins in the cells of the ducts.
Cancer that begins in the lobes or lobules is called lobular carcinoma and is more often found in both breasts than are other types of breast cancer.
Inflammatory breast cancer is an uncommon type of breast cancer in which the breast is warm, red, and swollen.
See the following PDQ summaries for more information about breast cancer:
- Breast Cancer Prevention
- Breast Cancer Screening
- Breast Cancer Treatment During Pregnancy
- Male Breast Cancer Treatment
- Unusual Cancers of Childhood Treatment (for information about breast cancer in childhood)
A family history of breast cancer and other factors increase the risk of breast cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk to your doctor if you think you may be at risk for breast cancer.
Risk factors for breast cancer include the following:
- A personal history of invasive breast cancer, ductal carcinoma in situ (DCIS), or lobular carcinoma in situ (LCIS).
- A personal history of benign (noncancer) breast disease.
- A family history of breast cancer in a first-degree relative (mother, daughter, or sister).
- Inherited changes in the BRCA1 or BRCA2 genes or in other genes that increase the risk of breast cancer.
- Breast tissue that is dense on a mammogram.
- Exposure of breast tissue to estrogen made by the body. This may be caused by:
- Menstruating at an early age.
- Older age at first birth or never having given birth.
- Starting menopause at a later age.
- Taking hormones such as estrogen combined with progestin for symptoms of menopause.
- Treatment with radiation therapy to the breast/chest.
- Drinking alcohol.
- Obesity.
Older age is the main risk factor for most cancers. The chance of getting cancer increases as you get older.
NCI’s Breast Cancer Risk Assessment Tool uses a woman’s risk factors to estimate her risk for breast cancer during the next five years and up to age 90. This online tool is meant to be used by a health care provider. For more information on breast cancer risk, call 1-800-4-CANCER.
Breast cancer is sometimes caused by inherited gene mutations (changes).
The genes in cells carry the hereditary information that is received from a person’s parents. Hereditary breast cancer makes up about 5% to 10% of all breast cancer. Some mutated genes related to breast cancer are more common in certain ethnic groups.
Women who have certain gene mutations, such as a BRCA1 or BRCA2 mutation, have an increased risk of breast cancer.
These women also have an increased risk of ovarian cancer, and may have an increased risk of other cancers. Men who have a mutated gene related to breast cancer also have an increased risk of breast cancer. For more information, see the PDQ summary on Male Breast Cancer Treatment.
There are tests that can detect (find) mutated genes. These genetic tests are sometimes done for members of families with a high risk of cancer. See the PDQ summary on Genetics of Breast and Gynecologic Cancersfor more information.
The use of certain medicines and other factors decrease the risk of breast cancer.
Anything that decreases your chance of getting a disease is called a protective factor.
Protective factors for breast cancer include the following:
- Taking any of the following:-Estrogen-only hormone therapy after a hysterectomy.-Selective estrogen receptor modulators (SERMs).-Aromatase inhibitors.
- Less exposure of breast tissue to estrogen made by the body. This can be a result of:-Early pregnancy.-Breastfeeding.
- Getting enough exercise.
- Having any of the following procedures:-Mastectomy to reduce the risk of cancer.-Oophorectomy to reduce the risk of cancer.-Ovarian ablation.
Signs of breast cancer include a lump or change in the breast.
These and other signs may be caused by breast cancer or by other conditions. Check with your doctor if you have any of the following:
- A lump or thickening in or near the breast or in the underarm area.
- A change in the size or shape of the breast.
- A dimple or puckering in the skin of the breast.
- A nipple turned inward into the breast.
- Fluid, other than breast milk, from the nipple, especially if it’s bloody.
- Scaly, red, or swollen skin on the breast, nipple, or areola (the dark area of skin around the nipple).
- Dimples in the breast that look like the skin of an orange, called peau d’orange.
Tests that examine the breasts are used to detect (find) and diagnose breast cancer.
Check with your doctor if you notice any changes in your breasts. The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Clinical breast exam (CBE): An exam of the breast by a doctor or other health professional. The doctor will carefully feel the breasts and under the arms for lumps or anything else that seems unusual.
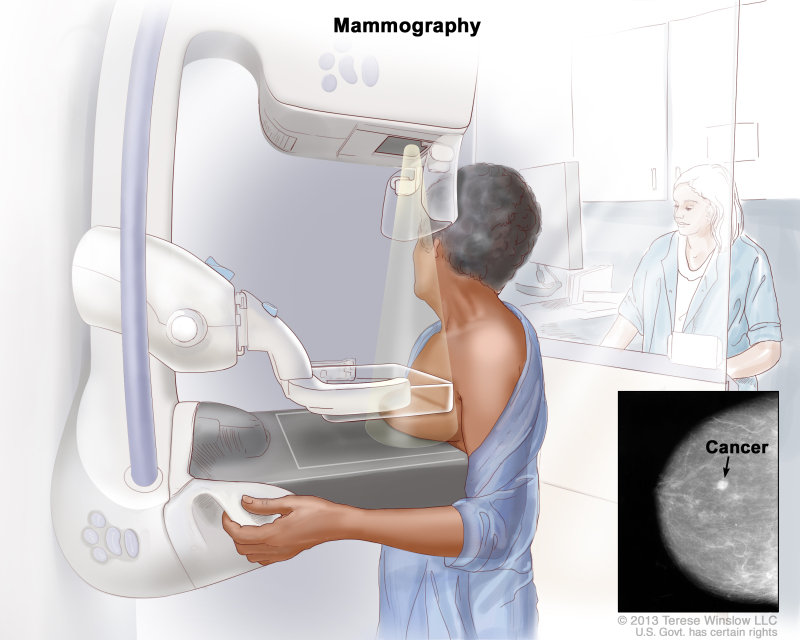
- Mammogram: An x-ray of the breast.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of both breasts. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. If a lump in the breast is found, a biopsy may be done.There are four types of biopsy used to check for breast cancer:-Excisional biopsy: The removal of an entire lump of tissue.-Incisional biopsy: The removal of part of a lump or a sample of tissue.-Core biopsy: The removal of tissue using a wide needle.-Fine-needle aspiration (FNA) biopsy: The removal of tissue or fluid, using a thin needle.
If cancer is found, tests are done to study the cancer cells.
Decisions about the best treatment are based on the results of these tests. The tests give information about:
- how quickly the cancer may grow.
- how likely it is that the cancer will spread through the body.
- how well certain treatments might work.
- how likely the cancer is to recur (come back).
Tests include the following:
- Estrogen and progesterone receptor test: A test to measure the amount of estrogen and progesterone (hormones) receptors in cancer tissue. If there are more estrogen and progesterone receptors than normal, the cancer is called estrogen and/or progesterone receptor positive. This type of breast cancer may grow more quickly. The test results show whether treatment to block estrogen and progesterone may stop the cancer from growing.
- Human epidermal growth factor type 2 receptor (HER2/neu) test: A laboratory test to measure how many HER2/neu genes there are and how much HER2/neu protein is made in a sample of tissue. If there are more HER2/neu genes or higher levels of HER2/neu protein than normal, the cancer is called HER2/neu positive. This type of breast cancer may grow more quickly and is more likely to spread to other parts of the body. The cancer may be treated with drugs that target the HER2/neu protein, such as trastuzumab and pertuzumab.
- Multigene tests: Tests in which samples of tissue are studied to look at the activity of many genes at the same time. These tests may help predict whether cancer will spread to other parts of the body or recur (come back).There are many types of multigene tests. The following multigene tests have been studied in clinical trials:-Oncotype DX: This test helps predict whether early-stage breast cancer that is estrogen receptor positive and node negative will spread to other parts of the body. If the risk that the cancer will spread is high, chemotherapy may be given to lower the risk.-MammaPrint: This test helps predict whether early-stage breast cancer will spread to other parts of the body. If the risk that the cancer will spread is high, chemotherapy may be given to lower the risk.
Based on these tests, breast cancer is described as one of the following types:
- Hormone receptor positive (estrogen and/or progesterone receptor positive) or hormone receptor negative (estrogen and/or progesterone receptor negative).
- HER2/neu positive or HER2/neu negative.
- Triple negative (estrogen receptor, progesterone receptor, and HER2/neu negative).
This information helps the doctor decide which treatments will work best for your cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer (the size of the tumor and whether it is in the breast only or has spread to lymph nodes or other places in the body).
- The type of breast cancer.
- Estrogen receptor and progesterone receptor levels in the tumor tissue.
- Human epidermal growth factor type 2 receptor (HER2/neu) levels in the tumor tissue.
- Whether the tumor tissue is triple negative (cells that do not have estrogen receptors, progesterone receptors, or high levels of HER2/neu).
- How fast the tumor is growing.
- How likely the tumor is to recur (come back).
- A woman’s age, general health, and menopausal status (whether a woman is still having menstrual periods).
- Whether the cancer has just been diagnosed or has recurred (come back).
Stages of Breast Cancer
Key Points for This Section
- After breast cancer has been diagnosed, tests are done to find out if cancer cells have spread within the breast or to other parts of the body.
- There are three ways that cancer spreads in the body.
- Cancer may spread from where it began to other parts of the body.
- In breast cancer, stage is based on the size and location of the primary tumor, the spread of cancer to nearby lymph nodes or other parts of the body, tumor grade, and whether certain biomarkers are present.
- The TNM system is used to describe the size of the primary tumor and the spread of cancer to nearby lymph nodes or other parts of the body.
- The grading system is used to describe how quickly a breast tumor is likely to grow and spread.
- Biomarker testing is used to find out whether breast cancer cells have certain receptors.
- The TNM system, the grading system, and biomarker status are combined to find out the breast cancer stage.
- Talk to your doctor to find out what your breast cancer stage is and how it is used to plan the best treatment for you.
- The treatment of breast cancer depends partly on the stage of the disease.
“Single-cell Transcriptomics reveals multi-step adaptations to endocrine therapy” is published in the journal Nature Communications.
Journal information: Nature Communications
Provided by Imperial College London



{kind=link}
{kind=link}