










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Cardiologists have issued a stark warning about the dangers of e-cigarettes, particularly for young people, as results of new research show the damage they cause to the brain, heart, blood vessels and lungs.
The study, which is published in the European Heart Journal today, also identifies some of the mechanisms involved, for which there has been limited information up until now.
Professor Thomas Münzel, of the Department of Cardiology of the University Medical Centre Mainz in Mainz, Germany, who led the study, said e-cigarettes were so dangerous, as well as addictive, that countries should consider banning them, action that countries such as India, Brazil, Singapore, Mexico and Thailand have already taken.
“We need to focus on the youth because this is by far the largest market,” he said.
“According to the US Centers for Disease Control and Prevention, over 3.6 million children in the US use e-cigarettes, with a jump of 78%, from 11.7% to 20.8%, among US high school students reporting e-cigarette use from 2017 to 2018.
And in the UK, 1.6% of those aged 11-18 use e-cigarettes more than once a week, compared with 0.5% in 2015.
Vaping, which was actually intended as an aid to help smokers quit, developed into a trend among young people in the US, leading to nicotine addiction, even among those who had not smoked before.”
Prof Münzel said governments should prevent young people having access to tobacco products, tax them heavily, curb the marketing of tobacco products, educate teenagers and their families about the dangers of tobacco products and intensify research into the adverse health consequences of vaping.
“We cannot allow an entire generation to become addicted to nicotine,” he said.
Prof Münzel and his colleagues investigated the effect of e-cigarette vapour on blood flow in the brachial artery in the upper arm in 20 healthy smokers before they vaped an e-cigarette and then 15 minutes afterwards. They also measured how stiff the artery became.
In addition, they exposed 151 mice to cigarette vapour over one, three or five days for 20 minutes six times a day.
They found that just one vaping episode increased heart rates and caused the arteries to stiffen and the inner lining of the arteries, the endothelium, to stop working properly in the smokers.
The endothelium is responsible for maintaining the correct dilation and constriction of blood vessels, protects tissues from toxic substances and regulates inflammation and blood clotting processes.
Endothelial dysfunction is involved in the development of cardiovascular disease.
Results from the mice showed that an enzyme called NOX-2 was responsible for damage to blood vessels, including those in the lungs and the brain, as a result of e-cigarette vapour.
NOX-2 is involved in the body’s defences against bacteria and in a process called oxidative stress—an imbalance between free radicals and antioxidants in the body.
Mice that were not able to produce NOX-2 were protected from the damaging effects of vaping.
The researchers also found that mice that were treated with macitentan (a drug used for treating endothelial dysfunction, increased blood pressure in the vessels and lungs and oxidative stress) or bepridil (used for treating oxidative stress and cell death in cases of high blood pressure, angina or chest pain) did not show signs of endothelial dysfunction, oxidative stress or inflammation.
The beneficial effects of these drugs suggested a central role of a chemical in the body called endothelin 1, which is involved in narrowing of the arteries, and a protein called FOXO-3, which protects against oxidative stress.
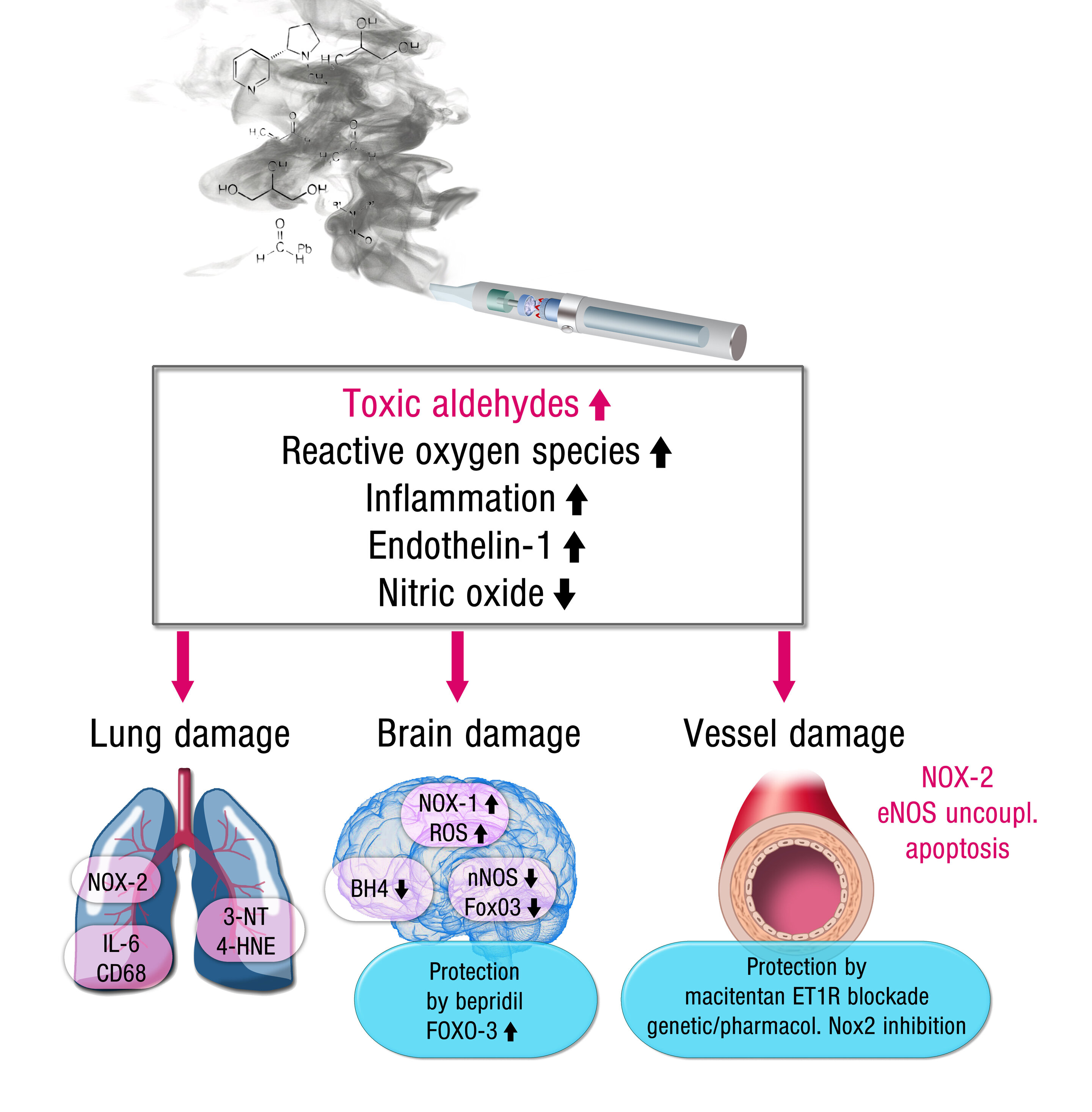
Prof Münzel said: “The results of the present studies identified several molecular mechanisms whereby e-cigarettes can cause damage to the blood vessels, lungs, heart and brain.
This is a consequence of toxic chemicals that are produced by the vaping process and may also be present at lower concentrations in the liquid itself.
Importantly, we identified an enzyme, NOX-2, that mediated all the effects of e-cigarettes on the brain and cardiovascular system, and we found that a toxic chemical called acrolein, which is produced when the liquid in e-cigarettes is vaporised, activated the damaging effects of NOX-2.
The beneficial effects of macitentan and bepridil indicate that e-cigarettes have the capacity to trigger constriction of blood vessels and to impair our cells’ antioxidant and survival systems.
“Our data may indicate that e-cigarettes are not a healthy alternative to traditional cigarettes, and their perceived ‘safety’ is not warranted.
In addition, we still have no experience about the health side effects of e-cigarettes arising from long-term use.
The e-cigarette epidemic in the US and Europe, in particular among our youth, is causing a huge generation of nicotine-addicted people who are being endangered by encouragement to switch from traditional cigarettes to e-cigarettes.
Research like ours should serve as a warning about their dangers, and aggressive steps should be taken to protect our children from health risks caused by e-cigarettes.”
A limitation of the study was that no healthy non-smokers were included. H
owever, the researchers point out that a strength is that they have received no funding from the e-cigarette industry.
“Recent studies indicate that e-cigarette industry funding is more likely to lead to results that indicate that e-cigarettes are harmless,” write the researchers in their paper.
Electronic nicotine delivery systems (ENDS) are commonly known as electronic cigarettes or e-cigarettes and vape pens. These devices are meant to deliver nicotine by heating up a vape liquid into an inhalable aerosol.
The vape liquid is a solution containing nicotine, flavoring agents, and solvents such as propylene glycol or glycerin [1]. The e-cigarette was first invented by Herbert A Gilbert in 1963, but the subsequent commercially viable design was patented by Hon Lik of China [2].
E-cigarettes entered the US market in 2007 [3] and have gained tremendous popularity since, especially among youth.
E-cigarettes were marketed as a safer alternative to conventional combustible cigarettes and therefore were promoted as harm reduction substitutes for current smokers.
However, there are contrasting claims associated with e-cigarettes being considered as a safer alternative to conventional cigarettes. The bottom-line according to the Centers for Disease Control and Prevention remains that e-cigarettes are possibly a less harmful alternative for current smokers addicted to combustible cigarettes [4••].
E-cigarettes are not for people who have never smoked in their life, and even establishing their efficacy as a smoking cessation tool needs thorough and long-term research [5]. The dangers of e-cigarette vaping include damage to the developing brain from nicotine [6–8] and exposure to toxic substances such as heavy metals, volatile organic compounds, and ultrafine particles [9, 10•].
Public Health Consequences
The adverse health consequences of e-cigarette use for both primary smokers and those exposed to secondhand smoke arises from the inhalation of the e-cigarette aerosol and levels of nicotine delivered into the system [11, 12].
Nicotine is known to be acutely toxic at high doses, and cases of nicotine poisonings due to vape liquids have seen a rise in recent years [13]. Nicotine is also a pharmacologically active biomolecule that sustains addiction, changes the way one’s brain functions [14], and is known to have particularly harmful consequences on the growing fetus if exposed to it during pregnancy [15, 16].
The e-cigarette aerosol contains a vast array of chemicals including any number of approximately 7000 flavorings [17], humectants such as Propylene Glycol and Vegetable Glycerin and contaminants such as metals, formaldehyde, acrolein, and tobacco-specific nitrosamines [1, 18] all with the potential to cause a wide variety of negative health effects. A list of these compounds and their physiologic effects are outlined below (Table (Table11).
Table 1
Constituents of ENDS Aerosol [19]
| Serial number | Aerosol component | Health risk | Reference |
|---|---|---|---|
| 1. | Ultrafine particles | Asthma, vasoconstriction leading to cardiovascular problems | [20, 21] |
| 2. | Benzene, formaldehyde, acetaldehyde, toluene, cadmium, lead, and nickel | Carcinogen, reproductive toxin | [22, 23] |
| 3. | Propylene glycol | Irritant of the eyes, throat and airways, long-term exposure leads to asthma | [24, 25] |
| 4. | Propylene oxide | Carcinogen | [26] |
| 5. | Diethylene glycol | renal and neurologic toxicity | [27] |
| 6. | Diacetyl and acetyl propionyl (sweet flavorings) | bronchiolitis obliterans | [28, 29] |
| 7. | Carbonyls | Cardiovascular toxicity | [30] |
| 8. | Copper nanoparticles | DNA fragmentation, mitochondrial stress | [31] |
Need for Regulation
In the years before the advent of ENDS technology, various public health measures made significant progress in tobacco control yielding a 6.9% reduction in smoking across the US population from 2005 to 2017 [32–35].
Keeping in mind the economic and social burden exacted by smoking-related diseases, the Federal Government had enacted various laws to make the sale of conventional tobacco products more difficult especially for the younger generation. However, rapid and unchecked increase in e-cigarette use [10•, 36] has once again threatened to endanger the health of our youth through nicotine addiction and vaping related disease [6, 37].
The National Youth Tobacco Survey held jointly by the FDA and the Centers for Disease Control and Prevention shows that around 3.6 million students (both middle and high school) were using e-cigarettes in 2018, up from 2.1 million in 2017 [38, 39]. There is emerging evidence that e-cigarettes can spur future tobacco product use in teens, whereas, on the other hand, banning tobacco products diminishes the smoking risk. Socio-economic background is another factor that also plays a major role in smoking initiation [40–42].
Another area of concern is the public health consequences of secondhand e-cigarette smoke on bystanders. Though the country has made significant progress in enacting clean air laws in public places including workplaces and indoors, a lot still remains to be done.
The use of e-cigarettes in public areas poses a serious health risk considering the various toxic constituents that have been shown to affect both the primary smoker and victims of passive smoking. It is pertinent to note that smoke-free laws in the USA were passed before ENDS entered the market and do not specifically mention the prohibition of e-cigarette smoking in many places. As such, this non-clarity may lead to non-compliance or exploitation of smoke-free rules [43, 44].
Existing Regulation
Federal Regulations
The FDA has been regulating tobacco products since June 2009; a timeline of the most important regulations is furnished in Table Table22.
Table 2
Timeline of policies/rules/regulations enforced at the federal level
| No. | Date | Name of agency | Regulation particulars | Implication |
|---|---|---|---|---|
| 1. | June, 2009 | Food and Drug Administration (FDA) of the Department of Health and Human Services. | Family Smoking Prevention and Tobacco Control Act. [45] | Authorizing FDA to regulate tobacco products including e-cigarettes. It led to the creation of center for tobacco products. |
| 2. | April, 2014 | Food and Drug Administration (FDA) of the Department of Health and Human Services. | Proposed Deeming Regulations [46] | Authorized the FDA to put heavy restrictions on most of the existing unregulated e-cigarette manufacturing industry and required premarket tobacco applications (PMTA’s) for new manufacturers |
On May 10, 2016, the U.S. Food and Drug Administration (FDA) passed a new rule effective August 08, 2016, deeming that all tobacco products be brought under the purview of Federal Food, Drug, and Cosmetic Act thus authorizing the FDA to regulate all tobacco products including ENDS [46].Apart from banning the sale of e-cigarettes to those below 18 years of age, the rule also stipulates several manufacturing standards and marketing limitations. The rule focuses on preventing a younger generation from becoming addicted to nicotine through e-cigarettes while taking into account the harm reduction potential of e-cigarettes for existing smokers addicted to nicotine.
More recently, in light of the 2018 National Youth Tobacco Survey, the FDA and Federal Trade Commission (FTC) issued warnings to four e-cigarette manufacturing companies around youth-focused advertisement, sale and distribution of ENDS products, especially on social media platforms [47].
State Regulations of e-Cigarettes
The US state and local governments have played a proactive role in enacting several laws at their level to protect against the misuse of e-cigarettes. In June 2019, San Francisco, California, became the first city in the USA to ban the retail and online sale of e-cigarettes.
This move is especially significant as Juul Labs, Inc., the makers of the Juul e-cigarettes variety, which has captured 70% of ENDS market share in recent years, is based out of San Francisco. Another trend is the implementation of Tobacco 21 laws in several states, increasing the minimum age of sale of tobacco products from 18 to 21.
As of June 2019, 16 states, Arkansas, California, Connecticut, Delaware, Hawaii, Illinois, Maine, Maryland, Massachusetts, New Jersey, Oregon, Texas, Utah, Vermont, Virginia, and Washington, the District of Columbia and 470 localities had implemented tobacco 21 laws [48].
As of April 2019, 13 states, 2 territories, and 841 municipalities have banned the use of e-cigarettes in 100% smoke-free public places [43]. In addition, regulations defining e-cigarettes, taxation, packaging, access to youth, and licensure of e-cigarette sales have been put into place across several states (Table (Table33).
Table 3
Law(s) in effect across all States & the District of Columbia in the USA (March 15, 2019) [49]
| State | Law(s) that define e-cigarettes | Law(s) taxing e-cigarettes | Law(s) on product packaging of e-cigarettes | Law(s) restricting youth access to e-cigarettes | Law(s) requiring licenses for retail sales of e-cigarettes | |
|---|---|---|---|---|---|---|
| 1 | Alabama | Yes | ||||
| 2 | Alaska | Yes | Yes | |||
| 3 | Arizona | Yes | ||||
| 4 | Arkansas | Yes | Yes | Yes | ||
| 5 | California | Yes | Yes | Yes | Yes | Yes |
| 6 | Colorado | Yes | Yes | |||
| 7 | Connecticut | Yes | Yes | |||
| 8 | Delaware | Yes | Yes | Yes | Yes (vape liquid) | |
| 9 | District of Columbia | Yes | Yes | Yes | Yes | |
| 10 | Florida | Yes | ||||
| 11 | Georgia | Yes | ||||
| 12 | Hawaii | Yes | Yes | Yes | ||
| 13 | Idaho | Yes | ||||
| 14 | Illinois | Yes | Yes | |||
| 15 | Indiana | Yes | Yes | Yes | Yes | |
| 16 | Iowa | Yes | Yes | |||
| 17 | Kansas | Yes | Yes | Yes | ||
| 18 | Kentucky | Yes | ||||
| 19 | Louisiana | Yes | Yes | Yes | ||
| 20 | Maine | Yes | Yes | Yes | Yes | |
| 21 | Maryland | Yes | Yes | |||
| 22 | Massachusetts | Yes | Yes | Yes | ||
| 23 | Michigan | |||||
| 24 | Minnesota | Yes | Yes | Yes | Yes | Yes |
| 25 | Mississippi | Yes | ||||
| 26 | Missouri | Yes | Yes | Yes | ||
| 27 | Montana | Yes | Yes | |||
| 28 | Nebraska | Yes | ||||
| 29 | Nevada | Yes | ||||
| 30 | New Hampshire | Yes | Yes | |||
| 31 | New Jersey | Yes | Yes | Yes | Yes | |
| 32 | New Mexico | Yes | Yes | |||
| 33 | New York | Yes | Yes | |||
| 34 | North Carolina | Yes | Yes | Yes | Yes | Yes (non-local manufacturers) |
| 35 | North Dakota | Yes | Yes | |||
| 36 | Ohio | Yes | Yes | |||
| 37 | Oklahoma | Yes | ||||
| 38 | Oregon | Yes | Yes | |||
| 39 | Pennsylvania | Yes | Yes | Yes | Yes | |
| 40 | Rhode Island | Yes | Yes | Yes | ||
| 41 | South Carolina | Yes | ||||
| 42 | South Dakota | Yes | Yes | Yes | ||
| 43 | Tennessee | Yes | Yes | |||
| 44 | Texas | Yes | Yes | Yes | ||
| 45 | Utah | Yes | Yes | Yes | Yes | |
| 46 | Vermont | Yes | Yes | Yes | ||
| 47 | Virginia | Yes | Yes | |||
| 48 | Washington | Yes | Yes | Yes | ||
| 49 | West Virginia | Yes | Yes | Yes | ||
| 50 | Wisconsin | Yes | ||||
| 51 | Wyoming | Yes | Yes | Yes |
Challenges and Recommendations
A review of the scientific literature shows largely incomplete data around the health effects of e-cigarettes. This translates to policy indecision among the regulatory authorities leading to confusion among the general public. This also causes problems for health care professionals in counseling current smokers looking to switch to e-cigarettes [50–52]. A long-term comprehensive study involving all major stakeholders is required to address this problem.
A bi-pronged approach could be key in balancing the regulatory aspects of e-cigarettes. It should consist of a prevention strategy in case of youth and a control strategy for current smokers who are looking at reduced harm alternatives for their nicotine fixation [53].
The prevention aspect can include laws that prohibit sale to minors, prevent youth-targeted advertisement campaigns [54, 55] and flavors, child-safe packaging, and campaigns addressing awareness and education. On the other hand, the control aspect can include better manufacturing measures, licensing laws for retail and online sale, selective taxation, and supervised subsidy for verified current smokers.
More information: Marin Kuntic et al, Short-term e-cigarette vapour exposure causes vascular oxidative stress and dysfunction: evidence for a close connection to brain damage and a key role of the phagocytic NADPH oxidase (NOX-2), European Heart Journal (2019). DOI: 10.1093/eurheartj/ehz772
Journal information: European Heart Journal
Provided by European Society of Cardiology



{kind=link}