










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



New research suggests that a baby’s age may offer clues to sudden unexplained infant death (SUID) – formerly known as SIDS.
The study identified two unique groups of babies who died from SUID – one who died within a week of birth, and another who died later on.
“SUID is a term that encompasses SIDS, unknown causes of death and accidental suffocation in bed.” explained study author Tatiana Anderson.
She said the new study found that, “deaths from [infant ages] 0 to 6 days were significantly different from deaths that occurred in the rest of the first year.”
Anderson is a neuroscience postdoctoral fellow at the Center for Integrative Brain Research at Seattle Children’s Research Institute.
She said a lot of the known risks for SIDS – young mothers, unmarried mothers, birth order and birth weight—didn’t seem to be factors for babies who died during the first week of life.
Even maternal smoking – a known SUID risk factor – didn’t seem to be one for babies who died suddenly in the first 48 hours, the study found.
Anderson said that doesn’t mean it’s OK to smoke in pregnancy, though.
“Smoking is still the biggest modifiable risk factor for SUID. [In a previous study, the researchers found that] 22% of SUID deaths could be attributed causally to smoking,” she said.
The researchers think their findings support the idea that SUIDs may have separate underlying causes, depending on an infant’s age.
The current study was a collaboration with Microsoft that relied on computer modeling. The model was developed from a database of all births in the United States from 2003 to 2013.
In all, the model included more than 41 million births, and nearly 38,000 sudden unexplained deaths.
“We didn’t go into the study predicting that the first week would be different, [that] these populations shouldn’t be lumped together under SUIDs,” Anderson said.
“There are different risk factors and likely different causes of death.”
The findings were published Dec. 9 in the journal Pediatrics.
Dr. Richard Goldstein, director of Robert’s Program in Sudden Unexpected Death in Pediatrics at Boston Children’s Hospital, wrote an editorial that accompanied the study.
“There are truths available in big datasets that maybe weren’t as available in the past,” he said.
But Goldstein cautioned against separating unexpected deaths into two groups just yet. He said it’s too soon to say that these are distinct groups with different causes. More research is needed.
Most experts in these sudden, unexplained deaths suspect that the deaths fall along a continuum by age, but that they likely have similar underlying causes or common vulnerabilities.
For example, it’s possible that these infants don’t have the proper autonomic system regulation that would wake them from sleep if they weren’t getting enough air. In one child, such a vulnerability might lead to stillbirth.
In another, it could cause sudden, unexpected death at 4 months of age.
Anderson said it’s too early to make any specific recommendations for parents based on this study.
Based on previous studies, she said it’s important for mothers not to smoke during pregnancy, and babies should sleep on their backs to reduce the risk of SUIDs.
Sudden death in a seemingly healthy infant during sleep is not a phenomenon of modern times, with cases being recorded throughout history for thousands of years. Indeed, one of the first cases is mentioned in the Bible (1 Kings 3:19).
However, these deaths have generally been attributed to overlaying, as it was common practice to sleep in the same bed as a child. Indeed, the death of an infant by “overlay” was considered such an issue that by the seventh century the event was a punishable offence (6), with the introduction of a “protective” wooden arcuccio for infants to sleep in during the 18th century in Europe with severe penalties if the infant died in a co-sleeping arrangement and the frame was not used (7).
By the 19th century the belief that the death of infants during sleep was due to overlaying was so entrenched that death was still attributed to this despite evidence suggesting otherwise (8), with calls for co-sleeping of parents and children to be illegal, especially if the parents were in an intoxicated state (9). This belief was maintained for the next 100 years (1).
While fewer deaths are attributed to overlaying in modern times, it is often impossible to exclude this possibility when death has occurred in a bed-sharing situation, which often leads to a diagnosis of “undetermined”.
As evidence built in the late 19th century that infants deaths were occurring without being associated with bed sharing (and thus overlaying), new theories of the factors mediating infant deaths began to arise.
In 1830, Kopp’s “thymic asthma” proposed that enlargement of the thymus in some infants resulted in a build-up of pressure leading to tracheal obstruction (10). Others suggested intrinsic asphyxial mechanisms (8), suffocation catarrh (11), superstition or the actions of witches and gods (12, 13) as the cause of sudden death. Although many theories have been discredited they have led to strong followings; the theory of status thymicolymphaticus, for example, was popular for over 30 years and resulted in over 800 publications, the most recent as late as 1959 (14). E
ven today, evidence is presented for numerous theories relating to the mechanisms mediating sudden death in infants (see below). Most recently a “wear and tear” hypothesis has been presented that suggests that “SIDS is the result of cumulative painful, stressful, or traumatic exposures that begin in utero and tax neonatal regulatory systems incompatible with allostasis” (15).
The authors argue that SIDS will be highest in winter-born premature male infants who are circumcised due to increased vulnerability to seasonal illness and stimulation of nocioreceptors during removal of the foreskin. However, like many contradictory theories in the past, this prediction lacks conclusive evidence.
While explanation for sudden death in certain infants remains incomplete, the term SIDS was only accepted as an official diagnosis on death certificates in 1971, with the term “sudden infant death” being allocated a separate code (coding number 798.0) in the World Health Organization’s International Classification of Diseases in 1979 (13).
Incidence
There has been a dramatic decrease in the incidence of SIDS since the introduction of safe sleep campaigns, with a 30-83% reduction in the SIDS rate (16–18). While, historically, rates have been recorded as high as 2-6 per 1,000 live births (19), they currently stand at 0.2-0.5 per 1,000 live births in most countries (18), although this rate can be heavily influenced by factors such as geographical location, climate, and ethnicity, as discussed below.
While the rate of SIDS has decreased, it is also important to note that the use of the term SIDS is becoming increasingly controversial and there has been a diagnostic shift in recent years. This has resulted in a decrease in the application of the term as a diagnosis with many professionals classifying cases into other categories and employing terms such as “undetermined”, “unknown”, “unascertained” or “ill-defined” despite the fact that cases fulfil the criteria for SIDS (20). Thus it is possible that changes in terminology could be partially responsible for the reduction in SIDS rate, as opposed to there having been an actual reduction in the number of deaths.
Diagnosis
One issue when applying the term “SIDS” is that there are no diagnostic features that can be attributed to a SIDS death, and thus application of the term relies on a process of elimination. When no known cause of death or contributing factors can be determined, the term SIDS is utilised.
This leads the way to a large window of interpretation as to how the term can, and when it should, be used, especially considering that not all SIDS cases have the same characteristics. In the past, SIDS has been applied to cases even when the investigation does not fulfil the required definitions (21, 22) and an autopsy has not been performed (23).
Indeed, it is estimated that an alternative diagnosis could have been made in up to 25% of SIDS cases or more (24, 25). Thus it is highly recommended that investigators use the Sudden Unexplained Infant Death Investigation (SUIDI) reporting forms devised by the Centers for Disease Control (26) in order to standardise data collection, increase uniformity across different medical examiners offices, and thus make the classification of the cause of death more uniform.
As stated above, the current definition of SIDS typically refers to an infant younger than 1 year of age whose death remains unexplained after a thorough case investigation including a death scene investigation, complete autopsy, and review of medical and clinical history (2). This definition also provides subcategories (as outlined in Chapter 1), which were introduced in an attempt to assist with classification and diagnosis.
The initial investigation of the death scene should combine the expertise of both law enforcement and medical personnel and should include, at a minimum, documentation of the sleep environment, the position that the infant was placed to sleep in, and the position in which he or she was found.
This would preferably include photographic and video evidence and re-enactment using a doll of a similar size to the infant. In addition, information pertinent to understanding factors that may have contributed to the death — including (but not limited to) time and circumstances surrounding death, room temperature, details of household activities prior to the death, details regarding clothing and bedding, and any unusual features — should also be collected (27).
In combination with a full death scene investigation, a comprehensive autopsy utilising accepted protocols (25) such as the International Standardized Autopsy Protocol (ISAP) should be completed. Ideally, this would include full external and internal examinations, the latter complemented by radiology of internal structures, histological analysis for pathology of all major internal organs including the brain and liver, toxicology analysis, assessment for the presence of infectious agents, electrolyte and metabolic studies, and molecular/genetic studies. However, it should be noted that some facilities do not have access to all of these diagnostic techniques.
As part of a routine autopsy, and to complement the findings at autopsy, assessment of the infant’s medical history should also be undertaken. This will aid in determining whether the infant had a history of potentially lethal conditions that may have contributed to death.
This history should include details pertaining to the pregnancy and delivery (including type of delivery and any noted complications), method of feeding, and immunization status. Ideally, a full family history should also be reviewed to provide insight into parental illnesses and disorders, especially if a history of maternal drug use is present, including smoking habits, particularly of the mother during pregnancy.
This history should also provide details as to whether there is a history of illness in siblings of the infant, including any previous deaths, as these may provide information relative to the presence of lethal inherited diseases or potential homicide. Therefore, without rigorous and in-depth investigation, there is a high potential that the cause of death could be labeled as SIDS based on incomplete or poor evaluation of the death instead of being labeled as a true “unknown” cause. It is also important to note that, despite fulfilling the requirements for a SIDS definition, some deaths may be listed as undetermined or ill-defined.
Risk Factors for SIDS
The cause of sudden death in some infants has long been proposed to be multifactorial, involving interactions of a variety of factors (28); each factor alone is not sufficient to cause death, but may, when expressed or experienced in combination with one or more other factors, result in death.
This theory was first presented as the multiple contingency hypothesis in 1972 by Wedgwood, who believed SIDS was most likely to occur when three overlapping factors occurred simultaneously (29). This was shortly followed by Emery’s interrelated causal spheres of influence model and Rognum and Saugstad’s fatal triangle (30). While the emphasis varied, all placed the focus on a multifactorial cause of death.
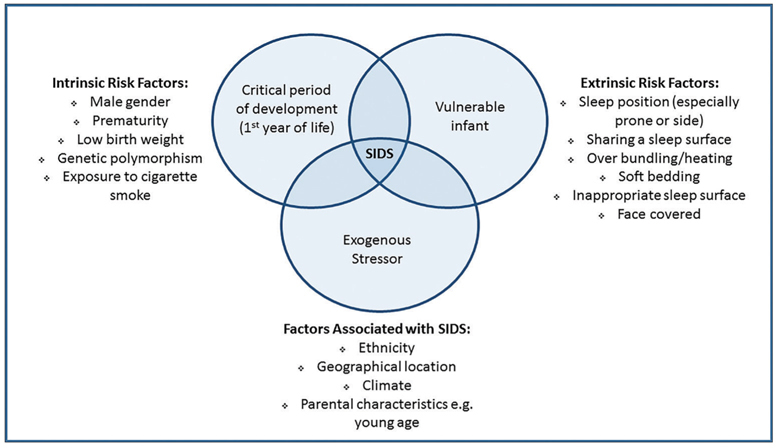
In 1994, Filiano and Kinney proposed the “Triple Risk Model” for SIDS (31), which today stands as one of the most accepted models in the field. As with the previous theories, the Triple Risk Model proposes that SIDS is not due to a single common pathway but that interrelated and overlapping factors combine to increase risk. Specifically, Filiano and Kinney posit that SIDS results from the simultaneous occurrence in an infant of a critical developmental period (i.e. the first year of life), the presence of an underlying vulnerability that increases susceptibility (i.e. unrecognised pathology), and exposure to an exogenous stressor (i.e. being placed in a prone position for sleep) (Figure 2.1).
When these factors align, the risk for SIDS is believed to be the greatest. The group further went on to propose that the risks for SIDS could be considered as either intrinsic or extrinsic, where intrinsic factors affect susceptibility and extrinsic factors represent physical stressors experienced around the time of death (see below) (32). While SIDS is not exclusive to infants with intrinsic or extrinsic risk factors, the importance of their role is demonstrated by the fact that at least one risk factor (and sometimes more) is present in approximately 90% of all SIDS cases, with very few SIDS cases reported where no extrinsic risk factors are present (32).
Developmental period
By definition, for a death to be classified as SIDS it must occur in an infant some time before their first birthday. Sudden and unexpected death can occur after the age of 1, though these deaths would be classified as sudden and unexplained death in childhood (SUDC), which has a much lower incidence (currently 1.4 to 1.8 deaths per 100,000 children) (33, 34). While death can occur at any time during the first year, approximately 90% of cases happen in the first six months of life, and there is an increased incidence between 2 and 4 months of age, a period when the infant brain is undergoing dramatic neurodevelopmental changes, especially to systems controlling homeostatic control (5).
Intrinsic risk factors
As mentioned above, intrinsic risk factors affect the vulnerability of the infant, increasing susceptibility to the influence of extrinsic risks. These factors include male sex, prematurity, low birth weight, genetic polymorphisms, and prenatal exposure to drugs, particularly nicotine (from cigarettes) and alcohol. Intrinsic risk factors are normally not modifiable, with the exception of exposure to maternal cigarette smoking or alcohol consumption during pregnancy. Although these could also be considered extrinsic risk factors (such as would occur via exposure to second-hand smoke after birth), as maternal exposure during pregnancy causes the highest risk for SIDS it will be presented in this section.
Sex, prematurity, and low birth weight
There is clear evidence that the incidence of SIDS is higher in males than females (35), with a ratio of 60 to 40 respectively (5). While some suggest male vulnerability is influenced by sex differences in genetic and biological makeup, it is not clear why the incidence of SIDS is higher in males, and this may simply be a reflection of the fact that male infants are more vulnerable to illness and disease than females, with males having a generally greater mortality rate overall (36). Prematurity and low birth weight also increase the risk for SIDS fourfold (37, 38), the most likely reason being the associated increased vulnerability in these infants due to immature autonomic systems.
Genetic polymorphisms
Unlike conditions such as Down Syndrome, where the presence of a third copy of chromosome 21 results in the phenotype, to date there has been no one gene identified in the etiology of SIDS. However, this does not exclude the possibility that some infants may carry unidentified genetic mutations or polymorphisms that interact with environmental or endogenous factors in complex ways, thus increasing their susceptibility to SIDS. A recent sequencing study of 161 SIDS infants by Neubauer et al. in 2017 identified potentially causative gene variants in 20% of their SIDS cases. These were associated with ion channelopathies (9%), cardiomyopathies (7%), and metabolic diseases (1%) (39). While it should be noted that the authors of this study focused specifically on genes associated with cardiovascular and metabolic diseases, mutations in cardiac ion channels, for example, could contribute to lethal arrhythmia and may explain sudden death in some infants. Others have reported differences in the expression of up to 17 genes in SIDS infants compared to controls, including three genes involved in mediating inflammatory responses (40). There have also been reports of polymorphisms in the promoter region of the serotonin transporter gene, which could result in altered serotonin uptake and regulation, supporting pathological and neurochemical studies reporting serotonergic dysfunction in SIDS (41, 42). Both Narita et al. (43) and Weese-Mayer et al. (44) reported an increase in the “L” allele in SIDS cases across different ethnic groups. The L allele is responsible for increasing the effectiveness of the promoter region of the serotonin transporter gene and thus an increased expression should lead to reduced serotonin concentrations. However, these findings have not been replicated in all studies (45, 46). In addition, findings of genetic abnormalities in SIDS vary across groups, with polymorphisms also being reported in genes for sodium channels, complement C4 and interleukin 10 (involved in immunity), and genes involved in the development of the autonomic nervous system, such as paired-like homeobox 2a and rearranged during transfection factor (RET) (47).
Two issues remain when trying to interpret the significance of gene mutations in SIDS. First, the rarity of multiple SIDS death in a family limits our ability to study the contribution of familial or inherited genetic abnormalities (see below). Second, many screening studies investigating genetic mutations in SIDS cases often identify several differences between groups in genes that have non-specific or heterogeneous functions; thus understanding the resultant consequences of changes to one or several genes becomes difficult.
Prenatal exposure to drugs including maternal cigarette smoking
Maternal cigarette smoking increases the relative risk for SIDS up to fivefold, with additional risks from postnatal exposure (48, 49). Despite evidence that smoking during pregnancy can be harmful, approximately 13% of women continue to smoke during this period (50). These numbers may be as high as 75% in some high-risk and Indigenous populations (51). Furthermore, the prevalence of maternal smoking during pregnancy in SIDS mothers has increased from 50% to 80% (49), such that in the wake of reductions in prone sleeping, exposure to cigarette smoke is now considered the dominate modifiable risk factor for SIDS (49). In addition, exposure to second-hand cigarette smoke both prior to, and after, birth also impacts on infant wellbeing (52), so that recommendations now state that mothers should not smoke during pregnancy, and infants should be in a smoke-free environment in order to reduce the risk of SIDS.
While the exact mechanism of how maternal smoking increases SIDS risk is still to be fully elucidated, it has been hypothesised that nicotine (the major neurotoxic component in cigarette smoke) is able to cross the placenta into the fetal circulation where it binds to endogenous neuronal nicotinic acetylcholine receptors present in the fetal brain (53). These receptors are widely expressed in the fetal brain from as early as 4-5 weeks’ gestation (54). Exogenous nicotine may bind to and inappropriately stimulate the function of these receptors. Indeed, there are several studies highlighting the impacts of prenatal cigarette smoking on fetal physiology including impaired arousability (55), changes to the apneic index for obstructive events during sleep (56), and altered parasympathetic control of heart rate (57) to name just a few. The processes by which this occurs are hypothesized to include the ability of nicotine (or other active ingredients in cigarette smoke) to control cell survival, affect neurite outgrowth, and regulate transmitter release (due to co-expression of these receptors on non-cholinergic neurons) (53) and synapse formation (see (58)). It has also been suggested that exposure to cigarette smoke in utero reduces lung capacity, thus resulting in chronic hypoxia after birth, or alternatively increases the risk of respiratory tract infection, both increasing infant vulnerability.
While the literature suggests that drug use, including cocaine and alcohol consumption, is associated with an increased risk for SIDS (59, 60), a direct relationship is often harder to determine due to the confounds of poly-drug use and environmental factors such as socioeconomic status. We do know that drug use, including cocaine and cigarettes, during pregnancy increases the risk of prematurity and low birth weight (61), themselves both associated with an increased risk for SIDS. Furthermore, infants born to mothers with a history of drug use are known to have altered physiology, including altered heart rate and fetal movements (62).
Extrinsic risk factors
Extrinsic risk factors represent physical stressors experienced around the time of death and often relate to the environment that the infant faces. These factors include sleep position (especially prone sleep position), sharing a sleep surface, over-bundling/over-heating, soft bedding, inappropriate sleep surfaces, and having the infant’s face covered.
Sleep position
The majority of SIDS deaths occur in association with a sleep period, with infants most often found dead in their cots (63). However, there is no association with any particular sleep period, with deaths attributed to SIDS occurring at any time of the day (64). Thus it is not surprising that sleep position, especially prone sleep position, which places additional physiological stress on cardiorespiratory systems, is the most significant environmental or “extrinsic” risk factor for SIDS. Indeed, prone sleeping (whether the infant is placed in this position or they move into this position during their sleep period) is estimated to increase the risk of SIDS by up to 14-fold (65).
The mechanism of death attributed to prone sleeping is often suffocation, and while suffocation is a valid possibility in some cases, it does not account for all deaths. Therefore, there are numerous theories relating to the factors that contribute to death while an infant is in the prone position. These include, but are not limited to, the face-down position resulting in oxygen deprivation leading to hypoxia, rebreathing of carbon dioxide leading to hypercarbia, reduced arousal responses and increased waking thresholds (especially to exogenous stimuli), compromised cerebral blood flow, airway obstruction, splinting of the diaphragm, altered cardiovascular capacity, and increased body temperature (66–68).
Despite no clear mechanisms being identified, the recognition that prone sleeping position plays a role in infant death was first reported in 1944 (69), and in SIDS deaths some 20 years later. However, the recommendation to place infants on their stomachs to sleep continued until the late 1980s. It is estimated that during this period prone sleep recommendations may have contributed to the unnecessary deaths of an estimated 60,000 infants (70). Publications highlighting the association between prone sleep position and sudden death in infants saw a decrease in the number of infants being placed prone to sleep and this was closely mirrored by a fall in SIDS deaths, confirming the strong association (71). In the late 1980s and early 1990s this led to the initiation of “Reducing the Risk” and “Back to Sleep” campaigns, which saw a dramatic decrease in the number of SIDS deaths (72); in some countries this was as high as a 73-83% reduction in the average number of deaths per year (16, 17).
While the numbers of SIDS infants found prone has gone down by nearly 50% since safe sleep campaigns were introduced, there has been little decline in the incidence of SIDS since 2006, suggesting that other extrinsic factors may be present. Thus it is also not surprising that the number of deaths associated with other known risk factors such as prematurity and bed sharing have increased 18% and 9% respectively (32) since this time. It is also important to note that, even with the success of safe sleep messaging, some health workers continue to use non-supine positioning and promote incorrect sleep positions to parents (73). In the study by Patton et al., “fear of aspiration” during sleep was the primary reason given for not choosing supine positioning (73), despite the fact that the incidence of deaths associated with the aspiration of gastric contents has not changed since the recommendation of supine sleep position (74).
Side sleeping position also increases the risk for SIDS, some studies reporting this risk to be similar to that of the prone position (75). This is often attributed to the ease with which infants can roll onto their stomachs, as many SIDS infants who were placed on their side to sleep were subsequently found prone at the time of death. In addition, the risk for SIDS is increased by changing an infant’s sleep position to one that they are not accustomed to, especially sleeping prone for the first time when an infant would normally sleep supine (76).
Sharing a sleep surface
Evidence from over 20 years in the United Kingdom indicates a significant increase from 12% to 50% in the number of SIDS/unexpected deaths associated with a shared sleep environment (77). These data support the argument that sharing a sleep surface, primarily beds and couches/sofas, increases the risk for infant death (78) due to the proposed potential for overlaying, suffocation, or overheating. This risk increases more when there is a history of prematurity or low birth weight, when more than one adult is present on the sleep surface, or when additional factors are present such as obesity, sedation, intoxication, or cigarette smoking (especially maternal smoking during pregnancy) in the person sharing the sleeping space with the infant (79, 80), or when the infant shares the sleep space for the entire night, or is younger than 11 weeks of age (81). However, sharing sleep surfaces with an infant is not a phenomenon specific to modern times and remains a common practice in many communities worldwide, without an associated increase in SIDS/infant deaths (82). Thus it could be argued that contemporary practices — in particular, the use of soft bedding — make sharing a sleep surface dangerous. Furthermore, sharing a sleep surface facilitates breastfeeding (83), which is thought to reduce the risk of SIDS (84). Therefore, further studies in this area are needed in order to fully understand why these differences exist. While bed sharing increases the risk for SIDS/infant deaths, safe sleep recommendations advocate infants sleeping near their parents or caregivers, as this decreases risks (85). There is no increase in the risk for SIDS for sleeping infants held in bed with an awake caregiver.
Soft bedding and inappropriate sleep surfaces
Sleep surfaces, and in particular soft bedding, also contribute to the risk of SIDS/unexpected infant death independent of sleep position; however, the risk is substantially higher again should the infant be placed prone (86). Soft surfaces, such as mattress and sheepskins, are thought to result in a potential “trough” when the surface depresses under the weight of the infant (87). In this situation, the infant may not be able to extricate themself, resulting in the potential for suffocation, asphyxia, or overheating. Blankets and pillows may also constitute soft sleep surfaces, and may, in addition to the above, increase the risk of face covering (81). Importantly, the risk of infant death is greatly increased if infants are left to sleep on a couch or sofa, with an odds ratio as high as 66.9, especially if this occurs in association with sharing this surface with an adult (more so than bed sharing) (78).
Overheating, over-bundling and covering of the face
A study by Kleemann et al. found that profuse sweating was present at the time of death in 36% of SIDS cases (88), suggesting that hyperthermia plays a role in some SIDS deaths. This has been attributed to endogenous factors including infections, immature central thermoregulatory centers, or increased amounts of brown adipose fat (89); it suggests an additional intrinsic risk in these infants. However, overheating due to over-bundling, increased ambient room temperature, or covering of the face or head is most likely to be attributed to exogenous factors, thus serving as an extrinsic risk factor (88). These extrinsic risks have the highest incidence when ambient temperatures fall and there is overcompensation. Indeed, over-bundling and thus presumably overheating during a sleep period is considered an independent risk factor for SIDS (90). Understandably, covering of the face may not only increase the risk for overheating but may also contribute to the risk for SIDS due to the increased chance of suffocation, asphyxia, decreased respiratory function, hypoxia, and hypercapnia.
Additional characteristics of SIDS cases
The above-mentioned risk factors are well documented to contribute to SIDS deaths; however, there are several additional factors that have also been shown to have an impact upon SIDS rates. Therefore, it is presumed that these factors influence the vulnerability of certain infants and could themselves be considered risks, though the means by which they impact on SIDS cases is not always evident. These factors include geographical location, climate, ethnicity, and certain parental characteristics. It is also worth discussing here the potential of altered sleep patterns in SIDS infants, and instances where there are multiple deaths of siblings in a single family, suggesting that the vulnerability may be inherited.
Geographic location and climate
Geographical location has a considerable influence on the number of infant deaths, with SIDS rates varying considerably across the globe (27). SIDS is also more common in colder climates than in warmer climates; likewise, it is more common during winter months than at other, warmer times of the year (91, 92). This is not a reflection of age, as the month (and thus season) in which an infant is born per se has no effect on the rate of SIDS (91). It is possible that the same factors that cause an increase in numbers of cases in winter months will also act for a longer time in colder climates. However, it should also be noted that the incidence of SIDS during colder months has decreased since the introduction of risk campaigns; in some geographical locations, such as Alaska and Sweden, where winter temperatures are extremely low, there was no evidence of a winter peak even prior to the era of safe sleep campaigns (93). It is also possible that the influence of geographical location and climate is driven more by different childcare practices or diagnostic protocols than actual location, which should be considered when comparing rates across countries.
Ethnicity
Ethnicity has been shown to be associated with the incidence of SIDS (94). The incidence of SIDS is lower in individuals with an Asian heritage (95), with a higher incidence reported in African-American (37) and Indigenous populations (96). For example, Native Americans of the Aberdeen Area of the Northern Plains have a rate of 3.5/1,000 live births, almost 7 times greater than the overall United States rate (96). However, these findings have not always been validated once socioeconomic factors, maternal history, and the presence of risk factors have been controlled for (97). In addition, the potential effects of ethnicity may be impacted by geographical location. For example, Californian infants with an Asian heritage have a higher rate of SIDS compared to Asian infants living in their country of ethnic origin (95). Again, consideration of different childcare practices should be made when interpreting the incidence of SIDS across different ethnic groups and assigning a potential genetic predisposition (98).
Parental characteristics
Young paternal age (<20 years) is considered to increase the risk for SIDS, despite the fact that SIDS infants in younger parents are less likely to be the firstborn child (35). Single maternal marital status (99), complications during pregnancy, fewer prenatal examinations (35), multiple births (38), and admission for psychiatric treatment of either parent, especially drug-related disorders (100), have also been implicated in the etiology of SIDS.
Sleep patterns
There is evidence to suggest that infants dying of SIDS have altered sleep patterns and altered responses to stressors while asleep. For example, in 1992 Schechtman and colleagues showed that SIDS infants have decreased waking time and therefore more sleep during the early morning period with more rapid eye movement (REM) periods throughout the night compared to controls (101). Abnormalities have also been noted in the organization, structure, and level of maturation of sleep in a group of “near-miss” SIDS infants (102). Furthermore, functions such as autoresuscitation and arousals during sleep are also altered in SIDS (101); these functions are especially vulnerable to the influence of maternal cigarette smoking during pregnancy (103). Thus it is possible that altered sleep states impact an infant’s ability to respond to stressors, potentially increasing their vulnerability during sleep.
Sibling deaths
The association of SIDS deaths amongst siblings is still debated. There have been reports of an increase in the incidence of SIDS of between two and ten times in infants who have had a sibling or twin death, including an increase risk based on the presence of SIDS in second- and third-degree relatives (104, 105). However, some of these outcomes have been explained once environmental and maternal factors have been controlled for and these families may only represent a small subgroup of individuals with increased vulnerability. There have also been reports of simultaneous sudden death in siblings supporting a genetic basis (106), although the importance of environmental factors should be taken into consideration under these circumstances. In addition, a report by Diamond et. al. indicated five consecutive sibling deaths in the same family (107), However, the authors feel that multiple deaths within the same family should raise concerns about other possible inherited conditions such as prolonged QT interval or metabolic disorders, homicide or potentially misclassified deaths of known cause. Thus, while multiple SIDS deaths in the one family may represent a genetic component in the etiology of SIDS, for 92% of families the risk of recurrence is considered small (105).
Mechanisms Underlying SIDS Deaths
Based on the fact that the definition of SIDS is dependent on the elimination of known causes of death, it is not surprising that there are no identifiable mechanisms underlying these deaths. This has led to a vast number of theories on the mechanisms responsible for SIDS. Chapters throughout this book will provide in-depth discussions on the proposed causation of SIDS, but below is a short summary of some of the current theories, all of which, obviously, have yet to be fully substantiated. It is also worth noting that in many studies there is a lack of comparative “normal controls”, which complicates our ability to interpret whether entities present in SIDS infants represent a primary cause of death or act as a secondary, or even an unrelated, phenomenon. Indeed, the authors of this chapter, along with others, are of the opinion that infant deaths attributed to SIDS are likely to represent a mixed population with various etiologies and disease entities contributing to one common endpoint (i.e. death) rather than all deaths being attributed to one single cause (108).
Respiration and respiratory function
Respiratory failure has long been thought to contribute to sudden and unexpected infant deaths (109), especially considering that sleep heightens the possibility of airway obstruction and apparent life-threatening events such as apneas. Furthermore, SIDS infants are hypothesized to have defects in respiratory control resulting in altered respiratory function, prolonged periods of “breath holding”, a failure of autoresuscitation, and defective arousal mechanisms (specifically, a failure to arouse to altered oxygen or carbon dioxide levels) (110–113). While some studies have reported mixed and obstructive respiratory events (114) or altered ventilatory control (115) prior to death in infants who subsequently died of SIDS, others have shown no difference in breathing patterns or respiratory rates (at least during regular breathing) (116), thus making integration of respiratory-related issues for SIDS difficult.
In SIDS cases there have been a number of anatomical abnormalities reported that are similar to those reported in obstructive sleep apnea/hypopnea syndromes (117), and thus it could be argued that these contribute to the respiratory issues hypothesised to exist in SIDS infants. These include retrognathic facial abnormalities such as retroposition of the maxilla, narrowing of the nasal passages, shallow temporomandibular joints, and enlargement of the tongue (117, 118). However, these abnormalities are not present in all cases and are not sufficient to enable a SIDS diagnosis to be made.
Siren recently postulated that SIDS occurs due to critical failure of the diaphragm (SIDS-critical diaphragm failure hypothesis) as a result of the increased respiratory workload following exposure to exogenous stressors leading to cessation of breathing and death (119). Others have suggested that abnormalities in peripheral airway stretch receptors, changes to peripheral sensory chemoreceptors including the carotid body, or dysfunction or immaturity in centrally located brainstem networks controlling upper airway functions could also contribute to respiratory issues, by increasing the risk for events such as apneas, or by reducing autonomic responses to airway obstruction during sleep (113).
Suggestions of respiratory-related mechanisms in SIDS have led to theories regarding an apparent protective effect of dummies/pacifiers, as supported by a recent meta-analysis by Alm and colleagues (120). It is thought that their use increases arousability, maintains airway patency and increases airway tone, and alters heart rate variability, thus improving autonomic tone (121). However, it should also be noted that there is contradictory evidence as to whether dummy or pacifier use interferes with the establishment of breastfeeding (itself thought to reduce the risk of SIDS) (122), and therefore caution should be given to the initiation of their use.
Hypoxia and hypoventilation
Due to evidence of repetitive apneas and hypoxic gasping prior to death in some SIDS cases (123), it has long been proposed that SIDS infants succumb to death due to repeated episodes of hypoxic/ischemic injury. In support of this theory, studies have reported subtle morphological changes in the liver, adipose tissue, and heart and circulatory system, which could be attributed to a chronic hypoxic state (27), though the findings remain inconclusive. In contrast, others have not reported changes to markers that would be expected to be altered following chronic hypoventilation — such as serum erythropoietin levels, for example (124), and, with the exception of some reports, brainstem gliosis (125). There is also a lack of significant evidence at autopsy of hypoxic-related changes (126). Furthermore, our own studies have illustrated differences in neurochemical and enzymatic levels in the brainstem between infants who had chronic hypoxia-ischemia and those classified as SIDS (41), suggesting an alternative mechanism (or mechanisms) related to death other than impaired oxygenation.
Cardiovascular function
It has been suggested that arrhythmia and cardiovascular changes are responsible for death in SIDS infants (127). This is driven by evidence proposing altered heart rate and heart rate variability; defects in centrally mediated cardiac control, primarily brainstem centers; autonomic imbalances and abnormal conduction pathways, including a left-handed His bundle (27, 128, 129); prolongation of the QT interval (the time from ventricular depolarization to repolarization) early in life (130); and severe bradycardia (with and without apnea) (131). While entities with known abnormalities of cardiac conduction are associated with sudden death, as with the issues around respiratory function mentioned above, there are considerable difficulties in proving a cardiac cause for SIDS, with some studies failing to report any differences in cardiovascular function (116). Furthermore, anatomical abnormalities related to cardiovascular function, if present, often exclude a diagnosis of SIDS, and in such cases, though they may be present, do not contribute to the cause of death (132).
Gastrointestinal function
While aspiration of gastric contents into the lungs or airways has been proposed as a possible cause of sudden death, it does not appear to be a valid marker for SIDS and can often be explained as a secondary event that has occurred after death (133). It has been proposed that reflux of gastric contents into the upper aerodigestive tract without aspiration may contribute to SIDS, as infants who suffer gastroesophageal reflux also manifest respiratory issues (134, 135). Besides the potential of airway obstruction, it has been suggested that reflux may also result in stimulation of peripheral esophageal receptors resulting in vagally mediated fatal apnea or bradycardia (136), or that some infants may have altered laryngeal receptor function upon stimulation (137). However, signs of reflux have not been consistently observed in SIDS cases (138) and are common in early infancy.
Nervous system abnormalities
There is a large body of literature suggesting that nervous system dysfunction plays a role in SIDS, especially in particular brainstem regions (41, 139, 140). These changes have been attributed to either abnormal development or to maturational delay, and are hypothesised to play a key role in SIDS due to their direct influence over homeostatic processes including cardiorespiratory control, sleep regulation, and arousal (41, 139–141).
Furthermore, marked changes in neural control (including within brainstem regions) overlap the peak period for SIDS, i.e. 2 to 4 months of age (53). However, our ability to fully understand changes to nervous system processes in SIDS is often limited due to contradictory findings in the literature and our ability to apply histological and molecular techniques to examine post-mortem specimens (due to rapid deterioration of tissues after death).
Central nervous system
Abnormalities in the brains of infants who have been classified as SIDS have been reported, including increased brain weight (142), and this is not attributed to simple edema or to cerebral anomalies. At the cellular level, studies have demonstrated focal granule cell bilamination in the dentate gyrus of the hippocampus (143), arcuate nucleus hypoplasia in the ventral medulla (144), altered development of the hypoglossal nucleus (145), altered neuronal cell number (140), changes to dendritic spines (141), and increased cerebral β-amyloid precursor protein (β-APP) expression (146).
The latter study also showed that the expression of β-APP in SIDS cases was related to sleep environment, with a higher expression in infants sleeping alone compared to those bed sharing, possibly suggesting different mechanisms relating to death in these two populations. Periventricular and subcortical white matter changes (147) and brainstem gliosis in the nucleus of the solitary tract and inferior olive (141, 148) have also been reported.
These changes have been attributed to ischemic damage, with ischemic necrosis also noted in these regions (149); however, many pathological findings overlap with observations from controls (150) and thus appear to have little diagnostic utility. Furthermore, while all of these abnormalities have the potential to alter brain function, it should be noted that the majority of these studies report findings in a subset of SIDS infants only (ranging from 20% to 94% across four publications alone) (141, 143, 146, 147), demonstrating that these changes are not present in all cases.
Neurotransmitter abnormalities
There are variable reports of altered neurotransmitter levels and changes to receptor systems in SIDS infants, with the majority of these focusing on brainstem regions. These have included changes to growth factors; cytokines; neuropeptides; and the catecholaminergic; cholinergic; and serotonergic systems (see (151) for an in-depth review). For example, Denoroy and colleagues reported a decrease in dopamine-β-hydroxylase and phenylethanolamine-N-methyltransferase in the medulla in SIDS infants, suggesting changes in the activity of central catecholaminergic neurons (152); however, Duncan and colleagues saw no difference in dopamine levels in the medulla (41).
There have also been reports of increased levels of substance-P in the medulla (153), reduced gamma-aminobutyric acid (A) receptor binding and subunit protein expression (154), and subunit specific changes to nicotinic acetylcholine receptors (155). However, the reported differences in neurotransmitter or receptor expression between SIDS cases and control cases can further be influenced by factors such as maternal cigarette smoking during pregnancy (155), highlighting the importance of accounting for these factors when trying to interpret neurochemical changes.
There have also been reports of a number of differences in markers of the serotonergic system, suggesting that serotonergic abnormalities in the medullary network may play a key role in SIDS due to the fact that serotonergic pathways in this region impact on virtually all homeostatic processes (41, 140). These findings have been validated across four independent cohorts, which reported a reduction in the levels of serotonin 1A receptors in medullary nuclei containing serotonergic neurons and their projection sites in the same cases (140).
These studies have also shown that SIDS infants have an increase in the number of serotonergic neurons in this region, though these neurons displayed an immature neuronal morphology (140) which may aid in the explanation of the observed reduction in the levels of serotonin in the raphe nucleus in these infants (41). SIDS infants also have reduced tryptophan hydroxylase2 (the key biosynthetic enzyme required for serotonin production) in the raphe obscurus, suggesting that SIDS infants may not be able to produce adequate serotonin levels (41); however the factors mediating reduced tryptophan hydroxylase2 levels remain undetermined.
While the literature on the central nervous system to date is heavily focused on the brainstem, more recent studies have reported changes to regions of the brain beyond the brainstem. Hunt and colleagues have shown a decrease in the immunoreactivity for orexin neurons, not only in the pons, but also in regions of the hypothalamus (156). Orexin plays a key role in the regulation of arousal and wakefulness, and thus changes to the levels of orexin are arguably well positioned to aid in the explanation of impaired arousal in SIDS.
Thus while limitations do exist with assessing changes in post-mortem tissues and the examples above are by no means all-inclusive, and numerous other pathological and neurochemical changes have been implicated in SIDS, they are suggestive of central nervous system abnormalities (particularly to brainstem regions) contributing to death in at least a subset of SIDS cases. However, due to the interrelated nature of central nervous system pathways, it is unlikely that changes to neurotransmitters system occur in isolation.
Peripheral nervous system
It is also possible that changes to peripheral nervous systems may impact on SIDS. Studies have reported histological changes such as a prominence of the dark variant of chief cells in the carotid bodies in SIDS cases (157). Changes such as this may suggest exposure to sustained hypoxemia and have the potential to impact the ability of chemoreceptors to respond adequately to changes in oxygen levels. However, interpretation of the role that changes to chemoreceptors play in SIDS is difficult, as conflicting outcomes regarding carotid body size, histological changes, and the number of neurosecretory granules and transmitter levels have been reported (157–159). As peripheral and central networks are highly integrated, it is likely that a change in one system may subsequently affect the other, and thus that both processes contribute to nervous system dysfunction in SIDS.
Immune responses and infectious agents
Anecdotal evidence of “a mild cold” or upper respiratory infection (32) close to the time of death, the presence of markers of infection and inflammation, and a peak incidence in winter months in many SIDS infants has led to the hypothesis that SIDS infants are immunologically incompetent and that stimulation of the immune system may contribute to death (160). Indeed, increased levels of immunoglobulins (including IgG, IgM and IgA) have been reported in SIDS victims (161), while others have reported changes to the number of IgM positive cell numbers in the wall of the trachea compared to controls (162).
This study concluded that the mucosal immune system is activated in SIDS; however, this was not to the same degree as infants where infection was known to contribute to, or cause, death. Others have suggested that SIDS infants have hypersensitive immune responses resulting in inappropriate allergic responses (163), though there is also evidence to support that this is not the case (11).
The argument for immune-mediated responses in the pathology of SIDS has been further strengthened by reports of the presence of viruses (164–166) including rhinovirus, cytomegalovirus, respiratory syncytial virus, Bordetella pertussis, enterovirus, and parvovirus, and also of the presence of bacteria including Staphylococcus aureus, Clostridium difficile, and Escherichia coli in the pathology of SIDS (167, 168). However, many of these are also present in control cases, suggesting that their presence may be more co-incidental than causative (167, 169).
The hypothesis of immune-mediated mechanisms contributing to SIDS deaths was further fuelled when four infants died of SIDS in 1979 within 24 hours of receiving a diphtheria-tetanus-polio (DTP) vaccine (170). Although occasional studies today still suggest an association between vaccination and sudden infant death (171), no causal associations have been found (38, 172, 173); in fact, some studies suggest that immunization may actually reduce the incidence of SIDS (174).
Thus, while it is possible that the presence of one, or a combination of, infectious agents may increase the vulnerability of some infants to sudden death, especially should they be faced with additional stressors, there appears to be no conclusive evidence of a single infectious agent being responsible for death in SIDS infants. Indeed, the presence of infectious agents in some SIDS infants may represent no more than a mere coincidence. In addition, immune-based systems in infants within the peak age range for SIDS (i.e. 2 to 4 months) are often considered normal (175). Furthermore, SIDS cases display little evidence of sepsis (176), which, if present, would exclude the use of a SIDS diagnosis.
Endocrine, metabolic and biochemical issues
Based on the pivotal role that the endocrine and metabolic systems play in regulating homeostatic functions, it is not surprising that abnormalities in these systems have been proposed to contribute to SIDS (177). Researchers have reported that SIDS infants have increased levels of tri-iodothyronine, which is released from the thyroid gland and affects nearly every physiological process in the body (178). Despite suggested changes to pancreatic (179) and pituitary gland pathology (180) or changes to cortisol and growth hormone levels (181), there is not sufficient evidence of endocrine system dysfunction.
There has been some suggestion of pathological findings in the liver, spleen, and skeletal muscle, attributed to metabolic defects at autopsy (182, 183). However, the role of metabolic issues is hard to determine, as inherited metabolic disease can easily be missed if access to specialised units is not available. The identification of inborn errors of metabolism sufficient to result in sudden death would preclude a SIDS diagnosis.
Biochemical differences have also been reported, with significant differences in the concentration of vitreous levels of potassium, calcium, phosphorus, creatinine phosphokinase, and lactate dehydrogenase (among others) in SIDS infants (184); however, findings from this study have not being replicated (185).
Thus, while it is possible that unrecognised metabolic and biochemical defects are present in some SIDS cases, there is no conclusive evidence. Furthermore, the most common metabolic abnormality, a deficiency of medium-chain acyl-coenzyme A dehydrogenase, has not consistently been reported to contribute to death in SIDS infants (186). Thus it would appear that the contribution these factors make to the number of SIDS cases is minimal.
Nutrition and toxins
It is obvious that adequate nutrition is needed for development, both in utero and after birth. While breastfeeding is believed to reduce the risk of SIDS (120), there is no direct evidence that maternal diet can impact on SIDS, though inadequate or unbalanced diets may led to fetal compromise that does increase the SIDS risk, such as intrauterine growth restriction (37).
Others have suggested that low levels of tryptophan, which is critical for serotonin production, as a result of either maternal diet or inefficient absorption from this diet, could result in lower brainstem serotonin levels and altered cardiorespiratory function in the offspring, as demonstrated using rodent studies (187).
Changes to the levels of the trace metal magnesium have also been shown in SIDS infants (188), but these have not been substantiated, and there is no conclusive evidence to support an association between SIDS and vitamin (189) or thiamine (190) deficiencies.
Thus the role of diet and nutrients remains to be determined. The same can be said for the possibility of accumulated toxins contributing to SIDS where there have been mixed findings on the levels of lead (191), cadmium, or chlorohydrocarbons (192). Furthermore, theories relating to sudden death due to inhalation of highly toxic trihydride gases from mattresses have never been proven (193, 194). SIDS infants show no evidence of poisoning by toxic gas, and the practice of wrapping mattresses, in an attempt to reduce the proposed toxic gas levels, has not affected the rate of SIDS deaths (195).
More information: Learn what’s known about preventing SIDS/SUIDS from the American SIDS Institute.



{kind=link}