










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Scientists have developed a new theory on the underlying cause of motor neurone disease, which could lead to more accurate diagnosis for patients and new treatments.
A team at the University of Exeter has found evidence that the condition is caused by an imbalance in cholesterol and other fat levels in the compartments of the body’s cells, triggered by a number of different gene mutations.
There are many different forms of motor neurone disease, which together affect around one in 2,500 people in the UK.
Due to their complex nature, motor neurone conditions may be difficult to diagnose, and currently no treatments are available to stop progression.
The degenerative condition can vary hugely in terms of specific symptoms, age of onset and rate of progression, even between members of the same family.
If confirmed, the new theory could lead to scientists to use blood samples to predict the course and severity of motor neurone disease in an individual, and to monitor the effect of potential new drugs to treat these disorders.
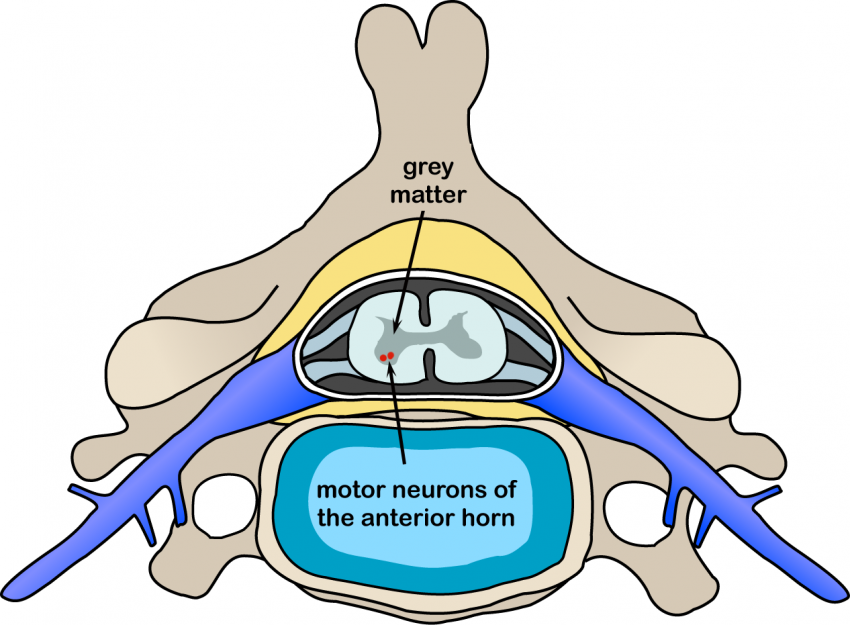
The finding particularly relates to the large group of motor neurone conditions called the “spastic paraplegias,” due to malfunction in how motor neurons in the upper part of the spinal cord communicate with muscle fibers.
This leads to symptoms including muscle stiffness, weakness and wasting.
Professor Andrew Crosby, of the University of Exeter Medical School, is lead author of the paper outlining the theory, published today in Brain.
He said: “For years, we have known that a large number of genes are involved in motor neurone disease, but so far it hasn’t been clear if there’s a common underlying pathway that connects them.
Our group’s previous research has identified 13 genes which if altered may cause the condition, and some of these discoveries have proven crucial as the genes we identified are directly involved in the cholesterol processing pathway.
That led to a Eureka moment, that cholesterol and other fat processing pathways in cells, are in fact the common link.”
Dr. Emma Baple, of the University of Exeter Medical School, said: “Currently, there are no treatments available that can reverse or prevent progression of this group of disorders. Patients who are at high risk of motor neurone disease really want to know how their disease may progress and the age at which symptoms may develop, but that’s very difficult to predict.
This paper should guide further research in this area, and we’re confident it could lead to more effective diagnostic tools and treatment strategies for a group of diseases that have a huge impact on people’s lives.”
Hereditary spastic paraplegia (HSP) encompasses a group of neurodegenerative conditions that result in lower limb spasticity and weakness. Despite causing significant disability, there is no available cure for this progressive condition (1).
The underlying pathophysiology of HSP remains poorly understood and it is likely that this varies according to genotype (2). There are >64 HSP associated genes and 13 HSP associated loci identified to date and this number will continue to grow with the advent of next generation sequencing (3, 4).
Recent research using stem cell models to study HSP disease pathogenesis, including SPG4 (HSP-SPAST), SPG3A (HSP-atlastin-1), and SPG11 (HSP-spatacsin) (5–7), have revealed several potential treatment options targeting the underlying disease mechanisms (8).
There is a paucity of clinical trials for HSP drug treatment options, the most recent trials targeting SPG5 (HSP-CYP7B1) showed improvement of biological markers but no discernible clinical improvement (1, 9, 10).
Biomarkers of disease severity and progression are vital components of establishing a clinical trial for therapeutic agents in HSP. Although several different biomarkers have been used in the small number of clinical trials published to date, a standardized biomarker for use across all clinical trials has not been defined (9–11).
Promising biomarkers for disease severity in HSP include the Spastic Paraplegia Rating Scale (SPRS) (10), gait analysis (12), motor evoked potentials (MEPs) (13), diffusion tensor imaging (DTI) (14), and genotype-specific biochemical markers, such as 27-hydroxycholesterol in SPG5 (9, 10).
Ideally, a disease biomarker for HSP should be easily accessible, able to be standardized across different institutions, affordable and minimally invasive. Challenges to developing a standardized biomarker include heterogeneity of HSP genotypes, broad spectrum of associated features and the typically slow progression of HSP.
Motor evoked potentials (MEPs) elicited through transcranial magnetic or electric stimulation have been proposed as a biomarker for disease severity in HSP (13). Prolongation of the central motor conduction time (CMCT) is used as a marker for upper motor neuron abnormalities causing slowing of conduction (15).
There are clear guidelines for measurement of MEPs allowing standardization across multiple centers, a useful feature for a disease biomarker (16). In order to evaluate the utility of MEPs as a biomarker for HSP, we performed a systematic review on the measurement of MEPs in HSP patient cohorts. Our aim was to evaluate CMCT as a diagnostic tool and as a biomarker for disease severity in HSP.
Discussion
This systematic review showed that prolonged or absent lower limb CMCT is a potential diagnostic biomarker for HSP. However, only one study showed a weak correlation between upper and lower limb CMCT and clinical disease severity. Hence, the utility of CMCT as a prognostic biomarker in HSP remains uncertain.
CMCT as a Diagnostic Biomarker for HSP
Most (96%) of studies reported prolongation of CMCT or absence of MEPs in the lower limbs with 78% of patients studied demonstrating lower limb CMCT abnormalities, whilst only 59% of studies reported abnormalities in the upper limbs.
The gold standard for the diagnosis of HSP was considered to be appropriate findings on clinical exam, appropriate exclusion of other disorders, and genetic testing. Compared to this standard, this review found that prolongation of lower limb CMCT had a sensitivity of 0.8.
The underlying disease pathophysiology of HSP is length-dependent axonal degeneration (2). CMCT measured from MEPs are thought to reflect neuronal integrity and are therefore a potential surrogate marker of disease severity. In this systematic review, CMCT was more likely to be abnormal in the lower limb (78%) vs. the upper limb (26%) consistent with more neuronal damage in the longer motor tracts to the lower limbs.
This was also seen when HSP was compared to other motor neuron diseases such as hereditary motor and sensory neuropathy (HMSN) types 1 and 2, amyotrophic lateral sclerosis (ALS) and primary lateral sclerosis (PLS), where CMCT to the upper limbs were more likely to be normal in HSP compared to these other conditions (30, 41, 42).
This finding was also confirmed in a study using the triple stimulation technique, thought to be the most accurate neurophysiological measure of upper motor neuron integrity, which found normal central motor conduction to the upper limbs in 15 patients with pure HSP (13 had SPG4 HSP) (51).
However, there was a significant proportion of patients with normal CMCT to the upper and lower limbs despite severe signs of spasticity. In fact, most studies did not find any correlation of CMCT abnormalities with disease severity, disease duration or age of onset (23, 27–29, 32, 34, 35, 45).
There are several possible explanations for this finding. One could be that although not significantly prolonged compared to controls, the CMCT of affected patients may be prolonged compared to their baseline before developing symptoms.
Two studies showed borderline or mild prolongation in CMCT in patients with HSP compared to controls although these were reported as normal as the prolongation was not significant (30, 34).
A longitudinal study of MEPs in patients with HSP, ideally from presymptomatic to symptomatic stage might shed light on the theory that increasing CMCT occurs in the presymptomatic stage and may not change once the patients is symptomatic, indicative of a ceiling effect of the test (see later).
Another explanation is that although symptoms are associated with neuronal damage, there may be enough residual nerve fibers that are intact to conduct the action potentials induced with transcranial magnetic stimulation or transcranial electrical stimulation.
There are limited neuropathological studies in HSP as it typically does not reduce life span. One study looked at cervical and lumbar spinal cord sections from two patients with HSP and found axonal swellings in the long descending corticospinal (CST) axons, more prevalent in the dorsal column (52).
Another looked at post-mortem tissue from six HSP patients and showed a significant reduction in axonal density and number of axons of CST and sensory tracts compared to controls (53).
The latter study demonstrated a reduction of both larger and smaller diameter fibers equally within the CST, however the integrity of the remaining neurons was not described and these could be enough to maintain central motor conduction without sufficiently demonstrating slow conduction in a grouped axon test.
It is also likely that clinical motor impairment in HSP is due to more global cerebral impairment than just the motor tracts. A study using magnetoencephalography to assess the connectivity of brain networks found changes that suggested global network rearrangement due to changes beyond motor impairment (54). One study looking at 118 patients with SPG4 HSP found 10% had psychiatric comorbidities and 3.5% had memory impairment, possible reflecting more global cerebral impairment (55).
There are several limitations of MEPs as a clinical biomarker. A recent paper investigating the use of MEP measures in movement disorders, specifically Parkinson’s disease, dystonia, Tourette syndrome, Huntington Disease and essential tremor, found discrepancies between studies reporting “canonical” MEP findings for these conditions (56). Similar to our findings, the authors found inconsistencies in methodology, diagnostic criteria for inclusion, study participants’ disease stages, and small sample sizes contributed to weaker evidence for the use of MEPs for diagnosis and differential diagnosis in movement disorders. See below for limitations of MEPs as a biomarker in HSP.
Limitations of MEPs as a biomarker in HSP
- Limitations of MEPs
- HSP-related factors
- ∘ Slow progression of disease
- ∘ Low prevalence
- ∘ Clinically and genetically heterogenous
- ∘ No previously known biomarker
- Limitations of reviewed studies
- ∘ Variability in study methodology
- ∘ Small sample size of patient cohorts studied
- ∘ Clinically and genetically heterogeneous patient samples
In studies where HSP was investigated along with other neurodegenerative conditions, CMCT changes in HSP were found to be milder than in multiple sclerosis, myelopathy, stroke and motor neuron disease (20, 21, 24). Therefore, characteristic changes of prolonged or absent LL CMCT with normal or mildly prolonged UL CMCT are more likely to suggest a diagnosis of HSP, whilst patients with grossly abnormal UL and LL CMCT are more likely to be seen in other types of motor neuron disease. However, it is important to note that these changes are not specific to HSP and can be seen in other motor neuron conditions (20).
In summary, although useful in diagnosis of HSP, CMCT is best used to confirm the clinical examination findings or the results of genetic testing.
CMCT as a Measure of Treatment Response for HSP
Only 30% of studies that investigated correlation between CMCT and other clinical variables reported a mild correlation with disease severity. One study only included two patients whilst the other only showed a correlation in patients with disease onset before 20 years old (32, 41). It is difficult to draw conclusions from these results, but the current evidence does not support a strong correlation with disease severity.
MEPs have not been studied longitudinally in HSP and therefore, the ability to assess changes in disease severity over time remains to be established. It is possible that individual patients may show changes from their baseline MEPs over time although some may not be in the abnormal range, whilst in others, their MEPs may become absent before their CMCT is in the abnormal range.
Patients may exhibit a “ceiling” effect where after a certain degree of motor neuron damage, CMCT measurements remain unchanged or absent. Studies investigating the change in MEP parameters longitudinally in HSP patients across different disease stages will help clarify the ability of MEPs to reflect disease progression.
None of the studies reviewed included presymptomatic patients with confirmed genetic diagnoses. MEP studies in this specific group of patients will help shed light on the utility of CMCT to predict future motor impairment. MEPs may be more sensitive to changes early in the disease process, before significant motor neuron damage limits variation in MEP measures.
Overall, longitudinal studies of MEPs in patients with HSP, including presymptomatic and various stages of the disease, are required to establish the utility of CMCT as a prognostic biomarker. Similarly, information from such studies will reveal the natural history of upper motor neuron damage in HSP.
Impact of HSP Genotype on MEP Findings
Fifty two percent of studies reviewed included patients from a single genotype, however, most of these were case reports or case series.
The largest studies of MEP in HSP included a heterogeneous cohort of patients with multiple genotypes and unknown genotypes (13, 23). In addition, these studies did not clearly delineate MEP changes according to each genotype, with the exception of the study by Karle and colleagues which performed subgroup analysis on SPG4 patients as well as providing values for other genotypes tested (13). Therefore, it is difficult to draw conclusions on MEP findings specific to each genotype although some patterns do emerge.
The largest cohorts that studied genotypically confirmed SPG4 patients noted that SPG4 patients had normal or only mildly prolonged MEPs (13, 34). These papers hypothesized that a very prolonged CMCT makes an SPG4 genotype unlikely, and may indicate SPG5, 6, 7, or 11. A study by Schulte et al. suggested that MEPs were a useful way of differentiating SPG4 from non-SPG4 HSP (47). Orlacchio et al. provides a caveat to this: all males in the SPG4 family studied had very prolonged CMCTs, whereas the women did not (36). This finding has not been replicated and the mechanism underlying this observation is uncertain.
For the other genotypes, the study numbers were too small to draw any firm conclusions. Though a significantly prolonged CMCT may point to certain HSP genotypes, patients will still need to undergo genetic testing to identify the mutation.
Future Recommendations
Further studies of MEPs in HSP with standardized methodology, strict inclusion criteria, adequate sample sizes and standardized assessment of clinical disease severity will clarify the role of MEP measures in HSP diagnosis and monitoring of disease severity. Our systematic review does not strongly support the use of MEPs as a sole biomarker in HSP although it remains useful when combined with other biomarkers, including clinical rating scales and diffusion tensor imaging.
There remains a need for a biomarker for use in future HSP clinical therapeutic trials. An ideal biomarker will be able to measure small changes in disease severity seen in HSP to account for the relatively short duration of clinical trials (1–2 years). Future studies of other potential biomarkers, such as neuroimaging and biological fluid-based biomarkers, are needed.Go to:
Conclusion
In summary, MEPs are not superior to clinical examination and genetic testing for diagnosis for HSP. However, MEP findings may help confirm a clinical diagnosis in suspected patients. Prospective longitudinal studies in presymptomatic and symptomatic patients with known genotypes are needed to clarify the utility of MEPs as a prognostic biomarker for HSP.
Overall, this systematic review has revealed variation in MEP findings in patients in HSP with the most consistent finding being prolonged lower limb CMCT over upper limb abnormalities. In fact, the presence of greater lower limb involvement may be more likely to signify the presence of HSP when compared to other upper motor neuron disorders.
Study quality assessment has shown inconsistencies in study methodology and reporting of results, perhaps contributing to the variation in results and preventing meta-analysis of available data.
Current studies are insufficient to establish the validity of MEPs as a prognostic marker or a measure of disease severity as most were not designed for this purpose. Nevertheless, no clear correlation was found between MEP abnormalities and disease severity or duration, but there was some tendency for certain subtypes (e.g., SPG4) to be less affected.
Future longitudinal studies in HSP patients with known genotypes, investigating the correlation of MEP parameters with standardized measures of clinical disease severity will help clarify the use of MEPs as a surrogate marker for disease severity for use in future clinical drug trials.
More information: Olivia J Rickman et al. Lipid metabolic pathways converge in motor neuron degenerative diseases, Brain (2019). DOI: 10.1093/brain/awz382



{kind=link}