











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



China expanded drastic travel restrictions Sunday to contain an epidemic that has killed 56 people and infected nearly 2,000, as the US, France and Japan prepared to evacuate their citizens from a quarantined city at the outbreak’s epicentre.
China has locked down the hard-hit province of Hubei in the country’s centre in an unprecedented operation affecting tens of millions of people in a bid to slow the spread of the respiratory virus.
Its ability to spread appears to be “getting stronger” though it is “not as powerful as SARS”, top Chinese health officials said at a press conference.
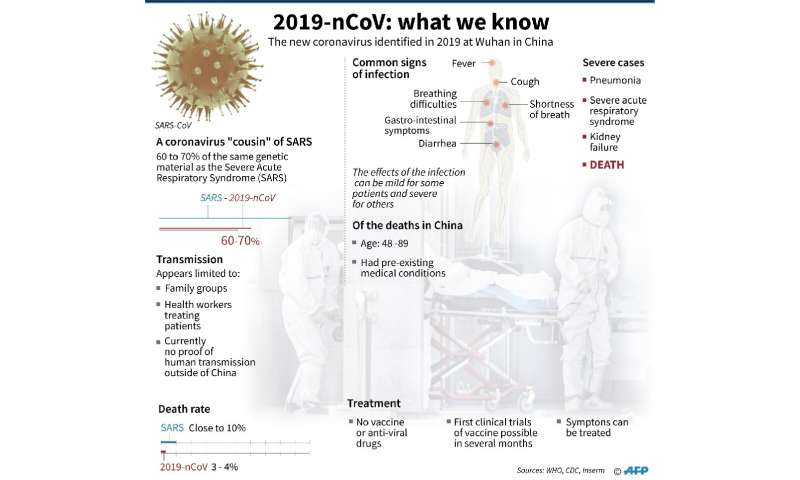
The previously unknown virus has caused global concern because of its similarity to the Severe Acute Respiratory Syndrome (SARS) pathogen, which killed hundreds across mainland China and Hong Kong in 2002-2003.
Outside the epicentre, Shandong province and four cities—Beijing, Shanghai, Xi’an and Tianjin—announced bans on long-distance buses entering or leaving, a move that will affect millions of people travelling over the Lunar New Year holiday.
The populous southern province of Guangdong, Jiangxi in the centre, and three cities made it mandatory for residents to wear face masks in public.
Originating in Hubei’s capital of Wuhan, the virus has spread throughout China and across the world – with cases confirmed in around a dozen countries including as far away as the United States.
The US State Department said Sunday it was arranging a flight from Wuhan to San Francisco for consulate staff and other Americans in the city.
France’s government and the French carmaker PSA also said they planned to evacuate staff and families, who will be quarantined in a city in a neighbouring province.
Japan is coordinating with Beijing to swiftly evacuate its citizens, Prime Minister Shinzo Abe said.
The complete annotated genome sequence of the novel coronavirus associated with the outbreak of pneumonia in Wuhan, China is now available from GenBank for free and easy access by the global biomedical community. Figure 1 shows the relationship of the Wuhan virus to selected coronaviruses.

Figure 1. Phylogenetic tree showing the relationship of Wuhan-Hu-1 (circled in red) to selected coronaviruses. Nucleotide alignment was done with MUSCLE 3.8. The phylogenetic tree was estimated with MrBayes 3.2.6 with parameters for GTR+g+i. The scale bar indicates estimated substitutions per site, and all branch support values are 99.3% or higher.
According to the CDC, as of January 11, Chinese health authorities say they’ve identified more than 40 human infections as part of this outbreak that was first reported on December 31.
The World Health Organization announced the preliminary identification of the novel coronavirus on January 9.
The GenBank record of Wuhan-Hu-1 includes sequence data, annotation and metadata from this virus isolated approximately two weeks ago from a patient believed to have contracted the disease in a Hubei province seafood market.
Rapid access to sequence data from public databases such as GenBank plays a vital role in helping countries develop specific diagnostic kits for disease outbreaks like this one.
Fear in Wuhan
Instead of New Year revelry, Wuhan has been seized by an eerie calm that deepened on Sunday as new restrictions banned most road traffic in the metropolis of 11 million.
Loudspeakers broke the silence by offering tips slathered with bravado.
“Do not believe in rumours. Do not spread rumours. If you feel unwell, go to the hospital in time,” the message said.
“Wuhan is a city that dares to face difficulties and keeps overcoming them,” the female voice added, mentioning the deadly 2002-03 SARS epidemic and 1998 Yangtze River flooding.
The health emergency has overwhelmed Wuhan’s hospitals with patients, prompting authorities to send hundreds of medical reinforcements, including military doctors, and start construction on two field hospitals.
The number of confirmed cases in the city could rise by 1,000, Wuhan’s mayor Zhou Xianwang predicted Sunday, based on the number currently undergoing observation in hospital.
He also said around five million people had left the city during the new year travel rush.
Speaking at a press conference and wearing a face mask, Zhou said the city’s medical staff were “very strained and tired”.
With non-essential vehicles banned from the road, volunteers stepped up to drive sick fellow citizens to hospitals.
“There has to be someone who does this,” Zhang Lin, 48, told AFP journalists as he waited for a patient to emerge from a clinic for the drive back home in nearly deserted streets.
Some foreigners in Wuhan expressed deep concern, saying they feared going outside.
“We want to be evacuated as soon as possible, because either the virus, the hunger or the fear will kill us,” Mashal Jamalzai, a political science student from Afghanistan at Central China Normal University, told AFP.
The outbreak is suspected to have originated in a Wuhan market where animals including rats, snakes and hedgehogs were reportedly sold.
China said Sunday it was banning all trade in wildlife until the emergency is over, but conservationists complain that China has previously failed to deliver on pledges to get tough.
Animal rights groups called for the ban to be made permanent, saying it could end the possibility of future outbreaks.

Another Disneyland closes
Health officials said the virus has since become transmissible between humans.
“From what we see now, this disease is indeed… not as powerful as SARS,” said Gao Fu, head of China’s Centre for Disease Control and Prevention, at a press briefing in Beijing.
However, it also appears that the “spreading ability of the virus is getting stronger,” said Ma Xiaowei, head of China’s national health commission.
The government says most deaths involved the elderly or people with existing ailments.
Fearing a repeat of SARS, China has dramatically scaled back celebrations and travel associated with the New Year holiday, which began Friday, while tourist sites like Beijing’s Forbidden City and a section of the Great Wall have closed.
In Hong Kong, Disneyland announced Sunday it had closed as a precaution after the city declared an emergency to combat the crisis. Shanghai’s Disneyland park had already closed Saturday.
Also in Hong Kong, protesters opposed to government plans to use a newly built public housing facility as a quarantine centre threw petrol bombs at the building, showing how fearful people are of the virus.
A new working group to tackle the epidemic, chaired by Chinese Premier Li Keqiang, called for local authorities to consider “extending the Spring Festival holiday”, in order to prevent the movement of people.
Several cities responded, with new school terms delayed in Beijing, Shanghai and the city of Suzhou in eastern Jiangsu province—which also ordered companies to extend the end of the holiday until February 9.
Research in contextEvidence before this study
We searched PubMed on Jan 13, 2020, with no starting date limitations, using the terms “family”, “pneumonia”, “Wuhan”, “coronavirus”, and “novel” for articles in English. Our search did not reveal any reports of novel coronavirus pneumonia in Wuhan before 2020. We only noted family clusters of pneumonia due to the novel severe acute respiratory syndrome (SARS) coronavirus in 2003, and Middle East respiratory syndrome coronavirus in 2012.
Added value of this study
The epidemiological, clinical, laboratory, radiological, and microbiological findings of unexplained pneumonia in a Shenzhen family cluster connected to a Wuhan hospital were presented. The diagnostic tests from relevant clinical samples confirmed the presence of a novel coronavirus in five of six patients with radiological changes of viral pneumonia. The phylogenetic analysis of this novel coronavirus suggested its linkage to a possible animal source.
Implications of all the available evidence
Although this novel coronavirus might have first originated from animals and now jumped into humans, the possibility of person-to-person transmission could not be excluded, as seen in this family cluster with no known history of exposure to markets or animals, and rapid intercity spread might be possible by air travel. Vigilant epidemiological control in the community and health-care facilities is important to prevent another SARS-like epidemic.
Results
The family cluster of six patients (patients 1–6) flew from Shenzhen to Wuhan on Dec 29, 2019, and flew back to Shenzhen on Jan 4, 2020 (figure 1). This travel period overlapped with the time period after the announcement of the first case of Wuhan pneumonia (symptom onset on Dec 12, 2019) according to the Chinese health authority.2 They had no history of contact with animals, visits to markets including the Huanan seafood wholesale market in Wuhan, or eating game meat in restaurants. T
he family stayed in the same hotel throughout their travel. Patients 1 and 2 stayed in one room and patients 3–6 stayed in another room. After patient 4 developed fever and diarrhoea on Jan 1, 2020, patients 5 and 6 stayed in the same room as patients 1 and 2, and patient 3 stayed with patient 4. Patients 1–6 had met with their relatives (relatives 2–5: one female cousin and three aunts of patient 3) every day during their stay in Wuhan for meals.
Relative 4 made frequent visits to the wet market but not the Huanan seafood wholesale market, which had been implicated by the health authority to be the epidemic centre.
Relatives 2–5 have developed fever, cough, and weakness since Jan 4, 2020. Patients 1 and 3 had visited relative 1, aged 1 year, and the son of relative 2, on Dec 29, 2019, in a Wuhan hospital, who had been treated in hospital for febrile pneumonia (relative 2 accompanied relative 1 in the hospital overnight; relative 1 later recovered and was discharged home on Dec 31, 2019).
Patient 3, but not patient 1, had worn a surgical mask during the hospital visit. The incubation period was estimated to be between 3 and 6 days. Patients 1–4 were symptomatic, and they only presented to our hospital (The University of Hong Kong-Shenzhen Hospital, Shenzhen) 6–10 days after symptom onset. For the two asymptomatic children (patients 5 and 6), patient 5 had ground-glass lung opacities identified by CT scan.
Unlike patient 5, who was aged 10 years and non-compliant to parental guidance, patient 6, who was aged 7 years and reported by her mother to wear a surgical mask for most of the time during the period in Wuhan, was not found to be infected by virological or radiological investigations. The blood tests and CT scan of patient 6 were normal.
After they returned to Shenzhen on Jan 4, 2020, patients 3–6 stayed in the same household of patient 7 (mother of patient 4) until Jan 11, 2020. Patient 7, who did not go to Wuhan or visit Shenzhen markets in the preceding 14 days, developed back pain and generalised weakness and attended the outpatient clinic at another local hospital on Jan 8, 2020. She was given cefaclor for 3 days with no improvement.
She developed fever and dry cough and attended the same outpatient clinic and was treated with intravenous cefazolin (two doses) on Jan 12, 2020. She was admitted to our hospital on Jan 15, 2020, due to persistent symptoms.

Of the six patients with pulmonary infiltrates (patients 1–5 and patient 7) on CT scans, three were male and three were female, with ages ranging 10–66 years (table 1). Four had chronic comorbidities and five had history of fever. The three older patients (aged >60 years: patients 1, 2, and 7) had dry cough and generalised weakness.
Patient 4 had productive cough. Patients 3 and 4 were younger adults and had diarrhoea and upper respiratory tract symptoms including sore throat, nasal congestion, and rhinorrhoea. Patient 3 also had pleuritic chest pain.
Except for patient 4, all six had normal or lower than average total white blood cell counts. The three older patients (patients 1, 2, and 7) all had substantially increased C-reactive protein, fibrinogen, and lactate dehydrogenase levels. Patients 1 and 2 also had lymphopenia, mild thrombocytopenia, and extended activated thromboplastin time.
All six patients showed multifocal patchy ground-glass opacities, especially around the peripheral parts of the lungs on CT scans, which were compatible with changes seen in viral pneumonia (figure 2).
No other clinical or radiological changes of lung congestion, fibrosis, or cancer to explain these ground-glass lung changes, or any concomitant radiological changes of dense consolidation, pleural effusion, lymphadenopathy, or pneumomediastinum were seen.Table 1Summary of clinical features and laboratory results of the family cluster infected with 2019 novel coronavirus, at presentation
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 7 | ||
|---|---|---|---|---|---|---|---|
| Relationship | Mother of patient 3 | Father of patient 3 | Daughter of patients 1 and 2 | Son-in-law of patients 1 and 2 | Grandson of patients 1 and 2 | Mother of patient 4 in Shenzhen | |
| Age (years) | 65 | 66 | 37 | 36 | 10 | 63 | |
| Sex | Female | Male | Female | Male | Male | Female | |
| Occupation | Retired | Retired | Office worker | Architect | Student | Retired | |
| Chronic medical illness | Hypertension; benign intracranial tumour treated by gamma knife | Hypertension | None | Chronic sinusitis | None | Diabetes | |
| Interval between symptom onset and arrival at Wuhan (days) | 5 (hospital exposure) | 6 | 4 (hospital exposure) | 3 | NA | NA | |
| Interval between admission to hospital and symptom onset (days) | 7 | 6 | 9 | 10 | NA | 7 | |
| Presenting symptoms and signs | .. | .. | .. | .. | .. | .. | |
| Fever | + | + | + | + | − | + | |
| Cough | + (dry) | + (dry) | − | + (productive) | − | + (dry) | |
| Generalised weakness | + | + | − | − | − | + | |
| Nasal congestion | − | − | + | − | − | − | |
| Rhinorrhoea | − | − | − | + | − | − | |
| Sneezing | − | − | − | + | − | − | |
| Sore throat | − | − | + | − | − | − | |
| Pleuritic chest pain | − | − | + | − | − | − | |
| Diarrhoea | − | − | + (3 days, 5–6 times per day) | + (4 days, 7–8 times per day) | − | − | |
| Body temperature (°C) | 39·0 | 39·0 | 36·2 | 36·5 | 36·5 | 39·0 | |
| Oximetry saturation (%) | 94% | 96% | NA | NA | NA | NA | |
| Haemoglobin (g/dL); (male normal range 13·3–17·1; female normal range 11·5–14·8) | 13·1 | 15·6 | 15·0 | 15·2 | 14·6 | 13·0 | |
| White blood cell count (× 109 cells per L); (normal range 3·9–9·9) | 4·8 | 4·2 | 5·6 | 11·4 (↑) | 6·5 | 4·3 | |
| Neutrophil count (× 109 cells per L); (normal range 2·0–7·4) | 4·0 | 3·2 | 3·1 | 8·1 (↑) | 3·2 | 2·7 | |
| Lymphocyte count (× 109 cells per L); (normal range 1·1–3·6) | 0·6 (↓) | 0·7 (↓) | 2·2 | 2·7 | 2·8 | 1·2 | |
| Platelet count (× 109 cells per L); (normal range 162–341) | 157 (↓) | 118 (↓) | 224 | 196 | 197 | 205 | |
| Prothrombin time (s); (normal range 11·0–14·5) | 12·6 | 12·5 | 13·0 | 13·0 | 13·1 | 12·9 | |
| International normalised ratio | 1·0 | 1·0 | 1·0 | 1·0 | 1·0 | 1·0 | |
| Activated partial thromboplastin time (s); (normal range 26·0–40·0) | 45·4 (↑) | 45·3 (↑) | 36·0 | 31·4 | 34·0 | 35·8 | |
| D-dimer (μg/mL); (normal range 0·0–0·5) | 0·6 (↑) | 0·3 | NA | NA | NA | 0·6 (↑) | |
| Fibrinogen (g/dL); (normal range 2·0–4·0) | 6·2 (↑) | 5·1 (↑) | 3·8 | 3·8 | 2·9 | 4·5 (↑) | |
| C-reactive protein (mg/L); (normal range 0·0–5·0) | 55·6 (↑) | 34·2 (↑) | 0·5 | 4·9 | 0·2 | 44·9 (↑) | |
| Albumin (g/L); (normal range 35·0–52·0) | 39·4 | 38·5 | 50·4 | 48·1 | 49·1 | 41·2 | |
| Bilirubin (μmol/L); (normal range 0·0–21·0) | 6·9 | 5·9 | 9·3 | 8·9 | 3·6 | 10·4 | |
| Alkaline phosphatase (U/L); (normal range 35–105) | 68 | 56 | 56 | 48 | 211 (↑) | 66 | |
| Alanine aminotransferase (U/L); (normal range 0·0–33·0) | 14·2 | 13·9 | 25·9 | 20·2 | 23·9 | 17·3 | |
| Aspartate aminotransferase (U/L); (normal range 0·0–32·0) | 20·5 | 23·3 | 27·4 | 18·1 | 28·2 | 27·6 | |
| Urea (mmol/L); (normal range 2·8–8·1) | 3·5 | 5·7 | 3·1 | 5·2 | 5·6 | 4·9 | |
| Creatinine (μmol/L); (normal range 44–80) | 53 | 93 (↑) | 67 | 87 (↑) | 51 | 55 | |
| Sodium (mmol/L); (normal range 136–145) | 136 | 133 (↓) | 142 | 141 | 141 | 139 | |
| Potassium (mmol/L); (normal range 3·5–5·1) | 3·2 (↓) | 3·7 | 3·7 | 3·7 | 3·9 | 3·8 | |
| Creatine kinase (U/L); (normal range 0–170) | 42 | 109 | 50 | 137 | 78 | 143 | |
| Lactate dehydrogenase (U/L); (normal range 135–214) | 286 (↑) | 232 (↑) | 192 | 176 | 194 | 252 (↑) | |
| Amylase (U/L); (normal range 28–100) | NA | NA | 70 | 61 | 61 | NA |
NA=not available. +=positive. –=negative. ↑=above normal range. ↓=below normal range.

All respiratory samples were negative on two point-of-care multiplex PCR systems for 18 respiratory viral and four bacterial targets. The two faecal samples from patients 3 and 4 who had preceding diarrhoea were negative on a multiplex PCR assay for common diarrhoeal viruses, bacteria, and parasites (table 2).
The respiratory samples of patients 1, 2, 4, 5, and 7 were positive for both RdRp and S genes by conventional RT-PCR, and for the S gene by real-time RT-PCR, which were confirmed by Sanger sequencing of all amplicons (appendix pp 3–5). Although the respiratory samples of patient 3 were negative for both RdRp and S gene (collected 9 days after symptom onset), she was still regarded as an infected case because she was strongly epidemiologically linked to the Wuhan hospital exposure and radiologically showing multifocal ground-glass lung opacities. Only the serum sample of patient 2 was positive and all other patients’ serum, urine, and faecal samples were negative for this novel coronavirus.
Phylogenetic analysis of the PCR products showed that the amplicon sequences of both RdRp and S genes from these five patients were novel (figure 3) and different from other known human or animal coronaviruses, including the SARS and bat SARS-related coronaviruses.Table 2Microbiological findings from clinical specimens collected from the family cluter infected with 2019 novel coronavirus, at presentation
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 7 | |||
|---|---|---|---|---|---|---|---|---|
| Interval between sample collection and symptom onset (days) | 7 | 6 | 9 | 10 | NA | 7 | ||
| Conventional RT-PCR | .. | .. | .. | .. | .. | .. | ||
| Nasopharyngeal swab | .. | .. | .. | .. | .. | .. | ||
| RdRp | + | + | ND | + | ND | + | ||
| Spike | + | + | ND | + | + | + | ||
| Throat swab | .. | .. | .. | .. | .. | .. | ||
| RdRp | NA | NA | ND | ND | ND | + | ||
| Spike | NA | NA | ND | + | + | + | ||
| Serum | .. | .. | .. | .. | .. | .. | ||
| RdRp | ND | ND | NA | NA | NA | NA | ||
| Spike | ND | + | NA | NA | NA | NA | ||
| Plasma | .. | .. | .. | .. | .. | .. | ||
| RdRp | NA | NA | ND | ND | ND | NA | ||
| Spike | NA | NA | ND | ND | ND | NA | ||
| Urine | .. | .. | .. | .. | .. | .. | ||
| RdRp | ND | ND | ND | ND | ND | NA | ||
| Spike | ND | ND | ND | ND | ND | NA | ||
| Stool | .. | .. | .. | .. | .. | .. | ||
| RdRp | NA | NA | ND | ND | ND | NA | ||
| Spike | NA | NA | ND | ND | ND | NA | ||
| Real-time RT-PCR (spike gene) | .. | .. | .. | .. | .. | .. | ||
| Nasopharyngeal swab | + (Ct 31) | + (Ct 27) | ND | + (Ct 31) | ND | + (Ct 27) | ||
| Throat swab | NA | NA | ND | ND | + (Ct 40) | + (Ct 33) | ||
| Sputum | NA | NA | NA | NA | + (Ct 27) | + (Ct 25) | ||
| Serum | ND | + (Ct 40) | NA | NA | ND | NA | ||
| Plasma | NA | NA | ND | ND | ND | ND | ||
| Urine | ND | ND | ND | ND | ND | NA | ||
| Stool | NA | NA | ND | ND | ND | ND | ||
| FilmArray RP2 plus (nasopharyngeal swab only) | ND | ND | ND | ND | ND | ND | ||
| Xpert Xpress Flu/RSV (nasopharyngeal swab only) | ND | ND | ND | ND | ND | ND | ||
| FilmArray GI panel (faecal sample only) | NA | NA | ND | ND | NA | NA |
Ct values for real-time RT-PCR presented in parentheses. Ct=cycle threshold. NA=not available. +=positive. ND=not detected. RdRp=RNA-dependent RNA polymerase. RP2=respiratory panel 2. Flu=influenza. RSV=respiratory syncytial virus. GI=gastrointestinal.


Two complete virus genomes (HKU-SZ-002a and HKU-SZ-005b) were sequenced using Nanopore technology and showed a novel coronavirus that is most closely related to those of the bat SARS-like coronavirus bat-SL-CoVZXC21 (NCBI accession number MG772934) and bat-SL-CoVZC45 (NCBI accession number MG772933). Their genome organisation is typical of a lineage B betacoronavirus.
The size of the virus genomes from patient 2 (HKU-SZ-002a) and patient 5 (HKU-SZ-005b) are around 29·8 kilobases with GC content of 38% (appendix p 6). HKU-SZ-002a and HKU-SZ-005b differ from each other by only two bases. One of them is a non-synonymous mutation at amino acid position 336 of non-structural protein 4 (Ser336 for HKU-SZ-002a; Leu336 for HKU-SZ-005b; figure 4).
Although amino acid sequence of the N-terminal domain of Spike subunit 1 of this novel coronavirus is approximately 66% identical to those of the SARS-related coronaviruses, and the core domain of the receptor binding domain of this novel coronavirus has about 68% amino acid identity with those of the SARS-related coronavirus, the protein sequence of the external subdomain region of receptor binding domain of Spike subunit 1 has only 39% identity, which might affect the choice of human receptor and therefore the biological behaviour of this virus (figure 4).

All six patients were admitted to hospital under isolation, supportive care, and remained stable as of Jan 20, 2020.
Discussion
We report here a familial cluster of unexplained pneumonia due to 2019-nCoV. Six of seven family members had radiological changes of viral pneumonia, among whom five (patients 1, 2, 4, 5, and 7) tested positive for 2019-nCoV by RT-PCR. Five patients (patients 1, 2, 3, 4, and 7) had associated symptoms at the time of presentation. Complete genome sequences of the two strains from patients 2 and 5 showed almost complete nucleotide identity with each other, and were closest to the bat SARS-related coronaviruses reported in 2018. Several possible scenarios of transmission exist.
The first and most likely scenario is that one virologically documented patient with pneumonia (patient 1) acquired the infection from a Wuhan hospital while visiting their relative (relative 1) and then patients 1–5 transmitted the virus to patient 7 on returning to Shenzhen. The second scenario is that patients 1–5 have directly acquired the infection from relatives 2–5 and transmitted it to patient 7 on returning to Shenzhen.
But this scenario is less likely because patients 1–5 developed symptoms before relatives 2–5. The third scenario is that patients 1–5 acquired the infection from an unknown common source in Wuhan and transmitted it to patient 7 when back in Shenzhen.
For the patients’ relatives (relatives 2–5), they could have acquired the infection from the hospital or the community, although no virological confirmation was possible and they had no animal contacts, game food, or visits to the Huanan seafood wholesale market. Notably, patient 1 or patient 3 who had visited Wuhan hospital might have been infectious before symptom onset because patient 5 was shedding virus without symptoms.
These findings suggested that person-to-person transmission and intercity spread of 2019-nCoV by air travel are possible, supporting reports of infected Chinese travellers from Wuhan being detected in other geographical regions.Many of the epidemiological, clinical, laboratory, and radiological features of this novel coronavirus pneumonia were similar to those of SARS patients in 2003.8, 15, 16
The incubation period of the Wuhan pneumonia appeared similar to that of SARS. The attack rate is rather high, up to 83% if we included the five patients (patients 1, 2, 3, 4, and 5) with unexplained ground-glass radiological changes of the lungs on CT scan as the case definition in this family outbreak after visiting Wuhan.
A rather unexpected finding from the lung CT scan of patient 5, which was done on the insistence by the nervous parents, also showed ground-glass pneumonic changes. Patient 5 was later confirmed virologically to have an asymptomatic infection. Although asymptomatic patients with SARS were uncommon, they were documented in our retrospective study in the minor 2004 SARS outbreak after reopening of the wildlife market in Guangzhou.17
Notably, patients 3 and 4 were afebrile at presentation to our hospital. These cryptic cases of walking pneumonia might serve as a possible source to propagate the outbreak. Further studies on the epidemiological significance of these asymptomatic cases are warranted.The symptoms of this novel pneumonia were also non-specific.
The three oldest patients in this family with comorbidities had more severe systemic symptoms of generalised weakness and dry cough. As expected, they might have decreased total white blood cell, lymphocyte, or platelet counts, with also extended activated thromboplastin time and increased C-reactive protein level.
The multifocal ground-glass changes on lung CT scan were typical of viral pneumonia. Their lung involvement was also more diffuse and extensive than those of the younger patients, whose blood test results were largely normal. Patient 4, who had a history of chronic sinusitis, might have a bacterial superinfection because he had a productive cough instead of a dry cough.
He also had a high white blood cell count, although the bacterial test was negative.Interestingly, the two younger adults (patients 3 and 4) initially had diarrhoea, which was also reported in 10·6% (15 of 142) of our SARS patients at presentation;18 however, the subsequent faecal samples of patients 3 and 4 that were collected 9–10 days after symptom onset were negative for the virus after the diarrhoea had long subsided. Up to 30% of patients with Middle East respiratory syndrome coronavirus (MERS-CoV) also have diarrhoea.19
Subgenomic RNA indicating viral replication was seen in faecal samples of patients with MERS.20 Moreover, MERS-CoV was shown to survive in simulated fed gastrointestinal juice and the ability to infect intestinal organoid models.20
Diarrhoea and gastrointestinal involvement are well known in coronavirus infections of animals and humans.21On microbiological testing, we did not find any evidence of other known respiratory viral or bacterial infections, but specific RT-PCR assays for two widely separated genome targets—the highly conserved RdRp and the highly variable S genes—were positive for this novel 2019-nCoV.
Two complete genome sequences of this novel coronavirus were recovered from the nasopharyngeal swab of patient 2 and the sputum sample of patient 5 with an earlier cycle threshold value indicating a higher viral load. Patient 2 had more underlying comorbidities and clinical features and radiological findings of more severe disease than the other patients included here. Moreover, the serum sample of patient 2 was also positive for 2019-nCoV, which might indicate some virus spillover from the more severely infected lung into the systemic circulation, as previously reported in patients with SARS.22 Sputum samples were available for testing from patients 5 and 7.
The cycle threshold values of the sputum samples were 8–13 cycles earlier than those of throat swabs, indicating higher viral loads detected in the lower respiratory tract. This finding is consistent with the observations in patients with MERS who had higher viral loads in lower respiratory tract samples than in upper respiratory tract samples.23
Thus, repeat testing of upper respiratory tract samples or testing of lower respiratory tract samples are warranted in clinically suspected cases with an initially negative result in nasopharyngeal or throat swab.
Unlike our patients in the 2003 SARS outbreak,22 we found no evidence of viral shedding in urine and faeces in these six patients. However, improved systematic serial collection and testing of an increased number of such samples is warranted.Coronaviruses are enveloped, positive-sense, single-stranded RNA viruses, capable of rapid mutation and recombination.
They are classified into alphacoronaviruses and betacoronaviruses, which both have their gene source from bats and are mainly found in mammals such as bats, rodents, civets, and humans; and gammacoronaviruses and deltacoronaviruses, which both have their gene source from birds and are mainly found in birds.24, 25, 26
Phylogenetic analysis of the PCR amplicon fragments from five of our six patients and the complete virus genome of 29·8 kilobases from patients 2 and 5 showed that the virus is a novel betacoronavirus belonging to the lineage B or subgenus sarbecovirus, which also includes the human SARS coronavirus.
The genome of our virus strains are phylogenetically closest to the bat SARS-related coronaviruses first found in the Chinese horseshoe bats, Rhinolophus sinicus, captured in Zhoushan, Zhejiang province, China, between 2015 and 2017.27 Notably, the first SARS-related coronavirus was also discovered in the R sinicus found in Hong Kong, and central and south China in 2005.28, 29
The full virus genome had about an 89% nucleotide identity with bat-SL-CoVZC45, which makes it a new species. Moreover, the Spike protein of our virus has an 84% nucleotide identity with the bat-SL-CoVZC45 coronavirus and an 78% nucleotide identity with the human SARS coronavirus.
Although substantial genetic differences exist between this and other betacoronaviruses, cross reactions in RT-PCR or antibody assays for SARS or other betacoronaviruses are possible if the primers and antigenic epitopes are not carefully chosen, as previously reported.30 Further studies on the optimal diagnostic tests are warranted.In summary, an outbreak of novel coronavirus is ongoing at Wuhan in the winter of 2019–20.
Similar to the 2003 SARS outbreak in Guangzhou, Wuhan is also a rapidly flourishing capital city of the Hubei province and the traffic hub of central China. Moreover, both outbreaks were initially connected to wet markets where game animals and meat were sold.
In the case of SARS, person-to-person transmission was efficient and super-spreading events had led to major outbreaks in hotels and hospitals. Learning from the SARS outbreak, which started as animal-to-human transmission during the first phase of the epidemic, all game meat trades should be optimally regulated to terminate this portal of transmission.
But as shown in this study, it is still crucial to isolate patients and trace and quarantine contacts as early as possible because asymptomatic infection appears possible (as shown in one of our patients), educate the public on both food and personal hygiene, and alert health-care workers on compliance to infection control to prevent super-spreading events. Unlike the 2003 SARS outbreak, the improved surveillance network and laboratory capability of China was able to recognise this outbreak within a few weeks and announced the virus genome sequences that would allow the development of rapid diagnostic tests and efficient epidemiological control.
Our study showed that person-to-person transmission in family homes or hospital, and intercity spread of this novel coronavirus are possible, and therefore vigilant control measures are warranted at this early stage of the epidemic.
ContributorsJF-WC and K-YY had roles in the study design, clinical management, patient recruitment, data collection, data analysis, data interpretation, literature search, and writing of the manuscript. SY, K-HK, KK-WT, HChu, CC-YY, RW-SP, H-WT, SK-FL, K-HC, VK-MP, W-MC, JDI, J-PC, VC-CC, and HChe had roles in the experiments, data collection, data analysis, and data interpretation. JY, CK-MH, FX, and JL had roles in recruitment, data collection, and clinical management. All authors reviewed and approved the final version of the manuscript.



{kind=link}
30154-9&id=gr1.jpg){kind=link}
30154-9&id=gr2.jpg){kind=link}
30154-9&id=gr3a.jpg){kind=link}
30154-9&id=gr3b.jpg){kind=link}
30154-9&id=gr4.jpg){kind=link}