











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Scientists have detected Marburg virus in fruit bats in Sierra Leone, marking the first time the deadly virus has been found in West Africa.
Eleven Egyptian rousette fruit bats tested positive for active Marburg virus infection. Research teams caught the bats separately in three health districts.
The presence of Marburg virus, a close relative to Ebola virus that also causes hemorrhagic disease in people, was detected in advance of any reported cases of human illness in Sierra Leone.
However, the virus’s presence in bats means people who live nearby could be at risk for becoming infected. No outbreaks have been reported to date.
The findings, based on PCR, antibody and virus isolation data, were officially published today in the journal Nature Communications. Preliminary findings were announced earlier in December 2018 to ensure rapid notification to the citizens of Sierra Leone and the international health community.
The paper highlights the value of collaborating with government and key stakeholders across human, animal and environmental sectors to engage at-risk communities about the discovery, address health concerns and communicate risk-reduction strategies before recognized spillovers occur.
Marburg virus was detected by projects led by the Centers for Disease Control and Prevention, the USAID-funded PREDICT project led by the One Health Institute at the UC Davis School of Veterinary Medicine, Njala University, Sierra Leone and the University of Makeni, Sierra Leone.
“Finding Marburg virus in bats in Sierra Leone before any known cases in people is a huge success, as public health officials and doctors can now include Marburg virus among the possible causes when diagnosing hemorrhagic fever cases in the region,” said Tracey Goldstein, co-principal investigator and pathogen detection lead for the PREDICT project from the UC Davis One Health Institute.
Angolan strains detected in bats for first time
To date, there have been 12 known outbreaks of Marburg virus with the most recent in Uganda in 2017.
The largest and deadliest outbreak occurred in Angola in 2005 where 227 people died. Five of the new strains identified among the Marburg-positive bats in Sierra Leone were genetically similar to the strain that caused the outbreak in Angola.
This is the first time scientists have detected these Angolan-like strains in bats.
The virus-positive bats were all Egyptian rousette bats, the known reservoir for Marburg virus, which primarily feed on fruit. Infected bats shed the virus in their saliva, urine and feces.
Egyptian rousette bats are known to test-bite fruits, urinate and defecate where they eat, potentially contaminating fruit or other food sources consumed by other animals or people, particularly children.
These bats sometimes serve as a food source for local populations as well. People may be exposed to Marburg virus through bat bites as they catch the bats.
Reducing risk of spillover through community outreach, risk-reduction training
Following the announcement of the preliminary findings by the government of Sierra Leone, the PREDICT team worked with government partners, universities and other key stakeholders to develop and implement evidence-based public health messaging across national, district, and local community levels in Sierra Leone.
Researchers and government officials met with community members to present their findings, answer questions about Marburg virus, and address how to reduce people’s risk of exposure and live safely with bats.
As an additional national-level public preparedness measure, Marburg virus disease has been included in testing regimens at national laboratories in Sierra Leone.
“PREDICT opened up the window to show there is more beyond Ebola, and demonstrated the need for partnership well before outbreak events unfold,” said Amara Jambai, deputy minister of health for Sierra Leone.
Scientists emphasize that people should not attempt to kill or eradicate bats in response to the discovery. Bats play important ecological and agricultural roles.
Fruit bats pollinate important crops, and insect-eating bats eat thousands of insects each night, including mosquitoes, which helps control pests that transmit disease and damage crops. Killing and coming into direct contact with bats can actually increase the risk of virus transmission, not halt it.
Finding viruses before they find us
The PREDICT team at UC Davis/University of Makeni and the team led by CDC/Njala University both began work in Sierra Leone in 2016 following the massive Ebola outbreak in West Africa. They each sought to discover the Ebola reservoir, the animal that helps maintain the virus in nature by spreading it without getting sick.
This Marburg discovery, the PREDICT team’s discovery of the sixth ebolavirus—Bombali virus—in Angolan and little free-tailed bats in Sierra Leone, and its subsequent finding of Bombali virus in Angolan free-tailed bats in Guinea illustrate the strengths and mission of USAID’s PREDICT project, which is to find viruses before they spill over into humans and become epidemics.
“Over a year ago, we worked with our Sierra Leone government colleagues to inform people across the country as fast as possible of this new health risk and remind people not to harm or come in contact with bats,” said Brian Bird from the UC Davis One Health Institute and global lead for Sierra Leone and Multi-Country Ebola operations for PREDICT-USAID. “I’m very proud of that work and our teams now that this full report is available.”
Marburg virus (MARV) is the causative agent of Marburg virus disease (MVD) in humans, with a case fatality rate ranging from 23 to 90%, depending on the outbreak [1]. MARV is a member of the Filoviridae family, which consists of the genera Marburgvirus, Ebolavirus, Cuevavirus, Striavirus, and Thamnovirus [2, 3].
The family, known as filoviruses, contains several viruses that are known to cause hemorrhagic, often lethal disease in humans and nonhuman primates (NHPs) all of which are within the Marburgvirus or Ebolavirus genera. Cuevavirus, Striavirus, and Thamnovirus are not known to cause disease in humans or NHPs.
Filoviruses have a non-segmented RNA genome in the negative sense, encoding for seven open reading frames; nucleoprotein NP, virion protein (VP) 35, VP40, glycoprotein GP, VP40, VP24, and viral polymerase L [4]. The filovirus genome is packaged into a unique filamentous virion, approximately 790 to 970 nm in length and 80 nm in width [5].
Within the genus Marburgvirus there is one species, Marburg marburgvirus, which is represented by two viruses; MARV and Ravn virus (RAVV) [6]. Although generally less well known than its cousin Ebola virus (EBOV), MARV was the first filovirus discovered following outbreaks in Germany and Yugoslavia (now Serbia) in 1967 [7].
Following its discovery, MARV cases were sporadically identified in Africa. However, in 1999 an outbreak was identified in the Democratic Republic of Congo, where multiple spillover events into the human population are thought to have taken place over the course of 2 years. This outbreak resulted in a total of 154 cases, with a case fatality rate of 83% [8].
In 2005, the largest documented outbreak of MARV occurred in Angola with 252 documented human infections and 227 deaths; a case fatality rate of 90% [9]. Outbreaks have continued to pop up since 2005, with a 2007 outbreak in Uganda, two instances in 2008 that involved tourists visiting Uganda returning home to the United States and Netherlands with MVD, and outbreaks in Uganda in 2012, 2014, and 2017 [1]. MARV was quickly recognized as a pathogen of extreme global importance and is currently classified as a Risk Group 4 pathogen by the World Health Organization and as a Select Agent by the US Centers for Disease Control and Prevention.
There are no licensed vaccines or treatments for MVD, partly due to the difficulty of performing clinical trials given the severity, infrequency, and rural nature of MVD outbreaks. Animal models of MVD are necessary to develop and test potential vaccines and treatments, and the ability of these models to reflect human pathogenesis is essential to moving forward into clinical trials.
MARV reservoir
All recorded MARV outbreaks have originated in Africa, excluding laboratory infections, where the virus is thought to be maintained in a natural reservoir [10]. Several bat species have been implicated in being a reservoir host for filoviruses [11], and there is strong evidence that Rousettus aegyptiacus, the Egyptian fruit bat, serves as a reservoir for MARV. Several cases of tourists and miners most likely acquiring MARV in caves populated by R. aegyptiacus have been reported [12–14]. Live virus was isolated from R. aegyptiacusbats within the Kitaka Cave, Uganda, the place where miners that had been diagnosed with MVD had worked [15].
Experimental infection of R. aegyptiacus bats with MARV yielded no outward symptoms of infection but was associated with a mild immune response and detection of viremia in multiple organs, with viral shedding detected in oral and rectal swabs [16–18]. Despite the shedding of virus and maintenance of viremia, there was a lack of transmission to susceptible R. aegyptiacus bats when cohoused with infected bats for up to 42 days [17].
In addition, the livers of MARV-infected bats showed hepatocellular necrosis and changes in inflammatory cells beginning at 3 days post infection (dpi) and progressed through to 7 dpi [17]. Hepatocytes and macrophages of the liver contained MARV antigen, as did macrophages of the spleen. This is reflected by increased alanine aminotransferase levels measured in infected bats, indicating liver damage [17].
Subcutaneous macrophages and other cells of the subcutaneous tissue from the site of inoculation also contained MARV antigen, as did small numbers of cells in the draining lymph nodes [19]. These pieces of information collectively support the narrative of R. aegyptiacus being a reservoir host of MARV and provide evidence for possible routes of transmission.
MARV human pathogenesis
There are few detailed clinical descriptions of MVD, due to the rural and severe nature of most outbreaks in Africa, and the availability of pathological and laboratory data from patients is limited. The detailed descriptions that do exist come from the initial outbreak in Marburg, Germany [20–22], an outbreak in Johannesburg, South Africa, involving three patients [23], and a few smaller, isolated cases and outbreaks originating elsewhere in Africa [13, 24–28]. In the following descriptions of various cases and outbreaks have been compiled to create an overall description of MARV pathogenesis in humans (Fig. 1).

Similar to many other infectious diseases, cases of MVD begin with flu-like symptoms such as chills, fever, headache, sore throat, myalgia, joint pain, and malaise, 2–21 days after the initial infection. Within 2–5 days of the first symptoms, patients can experience abdominal pain, nausea, vomiting, watery diarrhea, and lethargy.
On days 5–7, the intensity of the disease increases, and may include a maculopapular rash spreading from the torso to the limbs, conjunctivitis, sustained fever, and symptoms of hemorrhagic fever, such as mucosal bleeding, petechiae, blood in the stool and vomitus, and bleeding from venipuncture sites. The maculopapular rash begins as small, dark red spots around hair follicles of the trunk and sometimes upper arms, developing into a diffuse rash, and can become a dark erythema that covers the face, neck, chest, and arms.
Neurological symptoms such as confusion, agitation, increased sensitivity, seizures, and coma can occur in later stages of the disease, and all patients of the initial outbreak in Marburg, Germany, were described as having a sullen, negative, and slightly aggressive behavior [29].
Increases in alanine and aspartate aminotransferase (ALT and AST) and increased serum creatinine levels indicate hepatic and kidney damage [20, 23, 24]. Disseminated intravascular coagulation (DIC) [22, 28], lymphopenia, and thrombocytopenia [20] appear typically within 1 week of the first symptoms. In the late stages of disease, lymphopenia is offset by neutrophilia [30].
Patients either recover from their illness or die of dehydration, internal hemorrhage, organ failure, or some combination of systemic factors aided by a dysregulated immune response to the virus. Patients that survive typically don’t experience the severe late stage symptoms, but may experience sequelae such as arthritis, conjunctivitis, myalgia, and symptoms of psychosis during and after recovery [20].
Experiments with cultured cells from survivors indicate a proper adaptive response mounted by immune cells to the virus infection. In addition, serum samples from survivors showed IgG responses to MARV NP and GP, with two of the patients having significant neutralizing antibody titers. The neutralizing antibody titer diminished over time, with the decrease beginning at 21 months post infection (mpi) and dropping below detectable limits at 27 mpi [31].
Autopsies of RAVV-infected patients with lethal outcomes showed swelling of the heart, brain, spleen, kidneys, and lymph nodes, as well as hemorrhage of mucous membranes, soft tissues, and various other organs. All tissues examined had some form of hemorrhage, and focal necrosis was found on almost all organs and was especially prominent in hepatic and lymphatic tissues, as well as the testis and ovaries [32].
Damage to the liver tissue was severe, and there was extensive hepatocellular swelling and degeneration. Basophilic cytoplasmic inclusions were found in eosinophils near areas with necrosis and were positive for viral antigen [32]
. Additionally, there were hepatocytes and Kupffer cells that had inclusions similar to the ones found in eosinophils, though most Kupffer cells were unidentifiable in the tissues analyzed. In the spleen, there was moderate necrosis in both the red and white pulp, with lymphoid depletion evident in the white pulp. The red pulp had deposits of fibrin and cellular debris. The sinuses had cellular debris and granular material deposited, along with a small amount of fibrin [32].
Hemorrhage and severe necrosis were observed in the germinal centers. Viral antigen was present in the marginal zone of the red pulp and in macrophages, but was not present in the germinal centers, despite the severe necrosis. In the lymphatic organs and mucous membranes of the stomach and intestines, there was a high number of plasma cells and monocytes. There was a marked depletion of lymphocytes, now thought to be the product of bystander apoptosis rather than direct infection [32].
The kidneys were swollen, pale, and hemorrhagic, and there was tubule necrosis and parenchymal damage. Macrophages in the intestines and kidney contained what looked like viral inclusions. The alveoli of the lungs were congested, hemorrhaged, and contained alveolar macrophages surrounded by fibrin, and occasionally stained positive for viral antigen.
Three of the five autopsied cases in the outbreak in Marburg, Germany had glial nodule encephalitis, spread throughout the brain [23, 29, 33]. Taken together, the disease manifestations in the organs fit with the course of disease and give insight into the potential of sequelae experienced by MVD survivors.
Conclusions
MARV infection in humans is often characterized by a swift onset, a high chance of transmission to ill-equipped primary caregivers, and a high mortality rate. These traits, combined with the rural, infrequent, and chaotic nature of most outbreaks make human efficacy trials for MARV vaccines and treatments logistically and ethically challenging. The animal efficacy rule put forward by the US Food and Drug Administration (FDA) states that when human efficacy trials are not feasible, efficacy data from one or more animal models that accurately mimic disease and predict response in humans can be used as evidence of effectiveness [77].
In order to develop and test vaccines and therapeutics for MARV, animal models of MVD must be developed and characterized, and reflect human pathogenesis as accurately as possible. Based on a review of the literature and as described above, it’s clear that the NHP model best recapitulates MVD pathogenesis in humans. However, the animal husbandry burden, financial cost, and ethical concerns surrounding NHPs make them a poor choice for pilot experiments involving untested vaccines and treatments.
The easier and more cost-effective approach is to test potential vaccines and therapeutics in small animal models of MVD, to establish some degree of efficacy before moving to NHP studies. The VSV-EBOV vaccine, the first EBOV vaccine with clinical data showing effectiveness in humans [78], was shown to protect mice, guinea pigs, hamsters, and NHPs from EBOV challenge [79–81].
The Syrian golden hamster model of MVD presents an outcome very similar to MVD in humans, but requires an adapted virus, and has a limited array of commercially available reagents and assays. Guinea pigs have more commercially available products, but do not recapitulate some of the important aspects of human MVD (Tables (Tables11 and and2).2).
Mice are incredibly easy to acquire and handle, and have by far the most reagents available, as well as a multitude of transgenic and knockout models. However, mice also present pathology that is furthest from human MVD and are either immunodeficient or require an adapted virus to cause disease.
The animal models for MVD reviewed in this paper are effective at recapitulating human MVD pathogenesis in different capacities, and each has its place in the long process of testing vaccines and treatments for licensure. However, there is room for further characterization and development of new animal models of MVD, in order to close the gap between using simple animal models and accuracy of disease progression.
Figure 2. Marburg virus disease outbreak distribution map
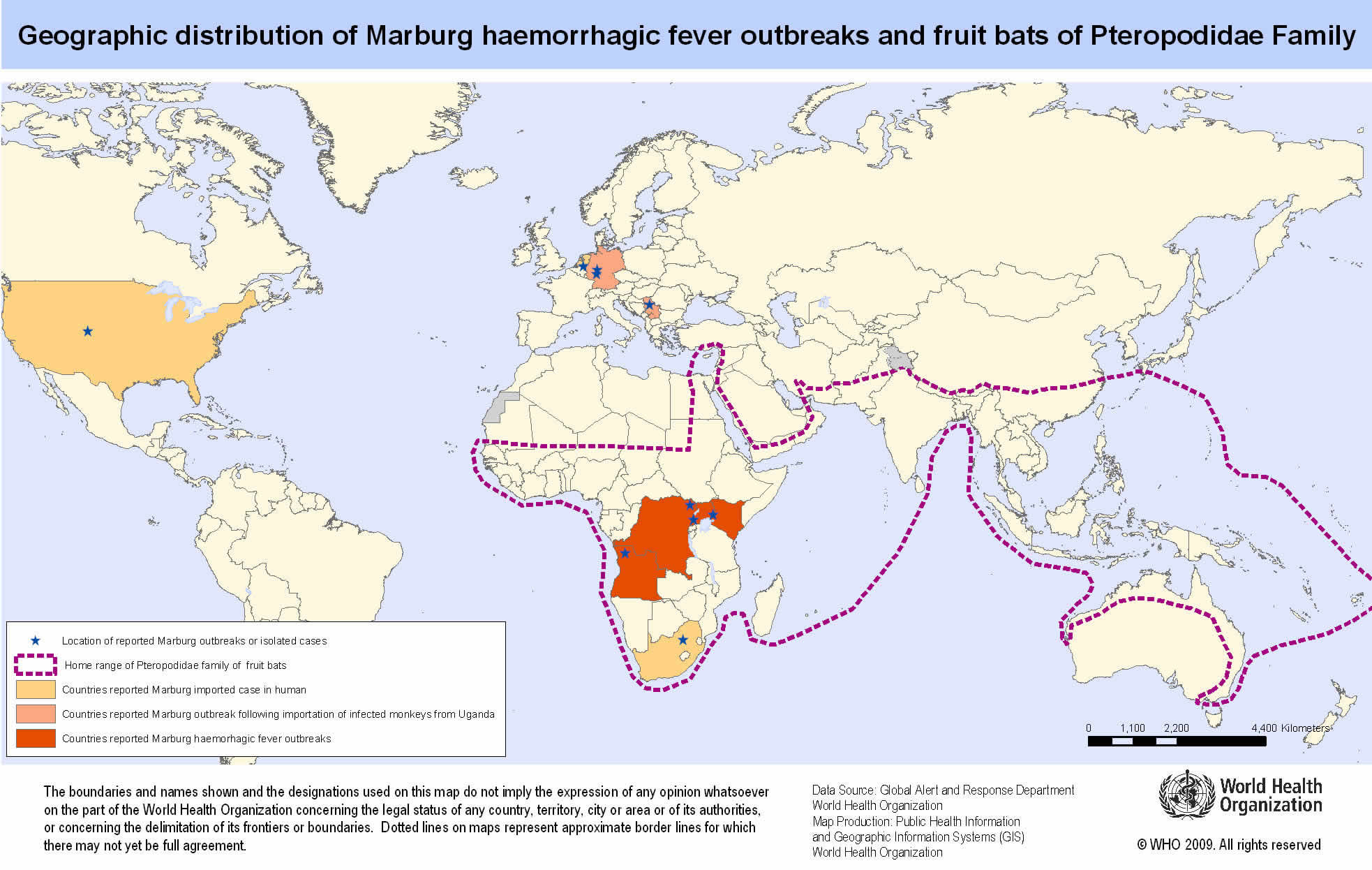
Countries reporting outbreaks of Marburg Hemorrhagic Fever
- Angola
- DR Congo
- Germany
- Kenya
- Serbia
- South Africa
- Uganda
Marburg virus transmission
Marburg virus has been found in monkeys, chimps and fruit bats in Africa. It is unknown how Marburg virus first transmits from its animal host to humans; however, for the 2 cases in tourists visiting Uganda in 2008, unprotected contact with infected bat feces or aerosols are the most likely routes of infection. After this initial crossover of Marburg virus from host animal to humans, transmission occurs through person-to-person contact.
This may happen in several ways: direct contact to droplets of body fluids from infected persons, or contact with equipment and other objects contaminated with infectious blood or tissues. Marburg virus spreads through human-to-human transmission via direct contact (through broken skin or mucous membranes) with the blood, secretions, organs or other bodily fluids of infected people, and with surfaces and materials (e.g. bedding, clothing) contaminated with these fluids.
In previous outbreaks, persons who have handled infected non-human primates or have come in direct contact with their fluids or cell cultures have become infected. Spread of the Marburg virus between humans has occurred in close environments and direct contacts. A common example is through caregivers in the home or in a hospital (nosocomial transmission).
Marburg virus transmission from animals to humans
Experts suspect that both viruses are transmitted to humans through an infected animal’s bodily fluids. Examples include:
- Blood. Butchering or eating infected animals can spread the viruses. Scientists who have operated on infected animals as part of their research have also contracted the virus.
- Waste products. Tourists in certain African caves and some underground mine workers have been infected with the Marburg virus, possibly through contact with the feces or urine of infected bats.
Marburg virus transmission from person to person
Infected people typically don’t become contagious until they develop symptoms. Family members are often infected as they care for sick relatives or prepare the dead for burial.
Medical personnel can be infected if they don’t use protective gear, such as surgical masks and gloves.
There’s no evidence that Marburg virus can be spread via insect bites.
Risk of Marburg virus exposure
For most people, the risk of getting Marburg hemorrhagic fever is low. The risk increases if you:
- Travel to Africa. You’re at increased risk if you visit or work in areas where Ebola virus or Marburg virus outbreaks have occurred.
- Conduct animal research. People are more likely to contract the Ebola or Marburg virus if they conduct animal research with monkeys imported from Africa or the Philippines.
- Provide medical or personal care. Family members are often infected as they care for sick relatives. Medical personnel also can be infected if they don’t use protective gear, such as surgical masks and gloves.
- Prepare people for burial. The bodies of people who have died of Ebola or Marburg hemorrhagic fever are still contagious. Helping prepare these bodies for burial can increase your risk of developing the disease.
People who have close contact with African fruit bats, humans patients, or non-human primates infected with Marburg virus are at risk.
Historically, the people at highest risk include family members and hospital staff who care for patients infected with Marburg virus and have not used proper barrier nursing techniques. Particular occupations, such as veterinarians and laboratory or quarantine facility workers who handle non-human primates from Africa, may also be at increased risk of exposure to Marburg virus.
Exposure risk can be higher for travelers visiting endemic regions in Africa, including Uganda and other parts of central Africa, and have contact with fruit bats, or enter caves or mines inhabited by fruit bats.
Marburg virus prevention
Prevention focuses on avoiding contact with the viruses. The following precautions can help prevent infection and spread of Ebola and Marburg.
- Avoid areas of known outbreaks. Before traveling to Africa, find out about current epidemics by checking the Centers for Disease Control and Prevention website.
- Wash your hands frequently. As with other infectious diseases, one of the most important preventive measures is frequent hand-washing. Use soap and water, or use alcohol-based hand rubs containing at least 60 percent alcohol when soap and water aren’t available.
- Avoid bush meat. In developing countries, avoid buying or eating the wild animals, including nonhuman primates, sold in local markets.
- Avoid contact with infected people. In particular, caregivers should avoid contact with an infected person’s body fluids and tissues, including blood, semen, vaginal secretions and saliva. People with Ebola or Marburg are most contagious in the later stages of the disease.
- Follow infection-control procedures. If you’re a health care worker, wear protective clothing, such as gloves, masks, gowns and eye shields. Keep infected people isolated from others. Dispose of needles and sterilize other instruments.
- Don’t handle remains. The bodies of people who have died of Ebola or Marburg disease are still contagious. Specially organized and trained teams should bury the remains, using appropriate safety equipment.
Marburg virus vaccine development
Scientists are working on a variety of vaccines that would protect people from Ebola and Marburg viruses. Some of the results have been promising, but further testing is needed.
Marburg virus symptoms
After an incubation period of 5-10 days, symptom onset is sudden and marked by fever, chills, headache, and myalgia. Around the fifth day after the onset of symptoms, a maculopapular rash, most prominent on the trunk (chest, back, stomach), may occur. Nausea, vomiting, chest pain, a sore throat, abdominal pain, and diarrhea may then appear. Symptoms become increasingly severe and can include jaundice, inflammation of the pancreas, severe weight loss, delirium, shock, liver failure, massive hemorrhaging, and multi-organ dysfunction.
Because many of the signs and symptoms of Marburg hemorrhagic fever are similar to those of other infectious diseases such as malaria or typhoid fever, clinical diagnosis of the disease can be difficult, especially if only a single case is involved.
The case-fatality rate for Marburg hemorrhagic fever is between 23-90%.
Marburg virus signs and symptoms typically begin abruptly within five to 10 days of infection with Marburg virus. Early signs and symptoms include:
- Fever
- Severe headache
- Joint and muscle aches
- Chills
- Weakness
Over time, symptoms become increasingly severe and may include:
- Nausea and vomiting
- Diarrhea (may be bloody)
- Red eyes
- Raised rash
- Chest pain and cough
- Sore throat
- Stomach pain
- Severe weight loss
- Bruising
- Bleeding, usually from the eyes, and when close to death, possible bleeding from the ears, nose and rectum
- Internal bleeding
Marburg virus complications
Marburg hemorrhagic fever leads to death for a high percentage of people who are affected. As the illness progresses, it can cause:
- Multiple organ failure
- Severe bleeding
- Jaundice
- Delirium
- Seizures
- Coma
- Shock
One reason the Marburg virus is so deadly is that it interferes with the immune system’s ability to mount a defense. But scientists don’t understand why some people recover from Marburg virus and others don’t.
For people who survive, recovery is slow. It may take months to regain weight and strength, and the viruses remain in the body for weeks. People may experience:
- Hair loss
- Sensory changes
- Liver inflammation (hepatitis)
- Weakness
- Fatigue
- Headaches
- Eye inflammation
- Testicular inflammation
Marburg virus diagnosis
Many of the signs and symptoms of Marburg hemorrhagic fever are similar to those of other more frequent infectious diseases, such as malaria or typhoid fever, making diagnosis of the disease difficult. This is especially true if only a single case is involved.
However, if a person has the early symptoms of Marburg hemorrhagic fever and there is reason to believe that Marburg hemorrhagic fever should be considered, the patient should be isolated and public health professionals notified. Samples from the patient can then be collected and tested to confirm infection.
Antigen-capture enzyme-linked immunosorbent assay (ELISA) testing, polymerase chain reaction (PCR), and IgM-capture ELISA can be used to confirm a case of Marburg hemorrhagic fever within a few days of symptom onset. Virus isolation may also be performed but should only be done in a high containment laboratory with good laboratory practices. The IgG-capture ELISA is appropriate for testing persons later in the course of disease or after recovery. In deceased patients, immunohistochemistry, virus isolation, or PCR of blood or tissue specimens may be used to diagnose Marburg hemorrhagic fever retrospectively.
Marburg virus treatment
There is no specific treatment for Marburg hemorrhagic fever. No antiviral medications have proved effective in treating infection with Marburg virus. Supportive hospital therapy should be utilized, which includes balancing the patient’s fluids and electrolytes, maintaining oxygen status and blood pressure, replacing lost blood and clotting factors, and treatment for any complicating infections.
Supportive hospital care includes:
- Providing fluids
- Maintaining blood pressure
- Providing oxygen as needed
- Replacing lost blood
- Treating other infections that develop
Experimental treatments are validated in non-human primates models, but have never been tried in humans.
More information:Nature Communications (2020). DOI: 10.1038/s41467-020-14327-8



{kind=link}