











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The Imperial College London and UCL researchers say their proof-of-concept study, published today in npj Digital Medicine, paves the way for the development of high-fidelity clinical imaging of the human brain that could be superior to existing technology.
Unlike existing brain imaging methods like MRI, CT and PET scanning, the technology could be applied to imaging any patient, and could be suitable for the continuous monitoring of high-dependency patients. It could be delivered by a relatively small device, which would also potentially make it portable via ambulance and enable fast investigation in advance of arrival to hospital.
The researchers are confident the technology will be safe as sound waves are already used for ultrasound scanning and this technology uses similar sound intensities. Ultrasound cannot easily penetrate through bone, whereas the new device, which is designed to be worn like a helmet, is able to overcome this barrier.
The new approach is of special value in patients investigated for stroke – the second commonest cause of death and commonest cause of adult neurological disability – where rapid, universally applicable, high-fidelity imaging is essential.
Lead author Dr. Lluís Guasch, of Imperial’s Department of Earth Science and Engineering, said: “An imaging technique that has already revolutionised one field – seismic imaging – now has the potential to revolutionise another – brain imaging.”
Professor Bryan Williams Director NIHR UCL Hospitals Biomedical Research Centre, which partly funded the research, said: “This is an extraordinary and novel development in brain imaging which has huge potential to provide accessible brain imaging in routine clinical practice to evaluate the brain in head trauma, stroke and a variety of brain diseases.
“If this lives up to its promise it will be a major advance. It is also a fabulous illustration of how the collaboration between engineers and clinicians, using methods from another sphere of science, can bring ground-breaking innovation into medical care.”
Transcending disciplines
Earth scientists use seismic data and a computational technique called full waveform inversion (FWI) to map the inside of the earth. Seismic data from earthquake detectors (seismometers) are plugged into FWI algorithms that extract 3-D images of the Earth’s crust that can be used to predict earthquakes and search for reservoirs of oil and gas.
Now Imperial researchers have adapted this approach to medical imaging, developing a method that uses sound waves with the ultimate aim of producing high-resolution images of the brain.
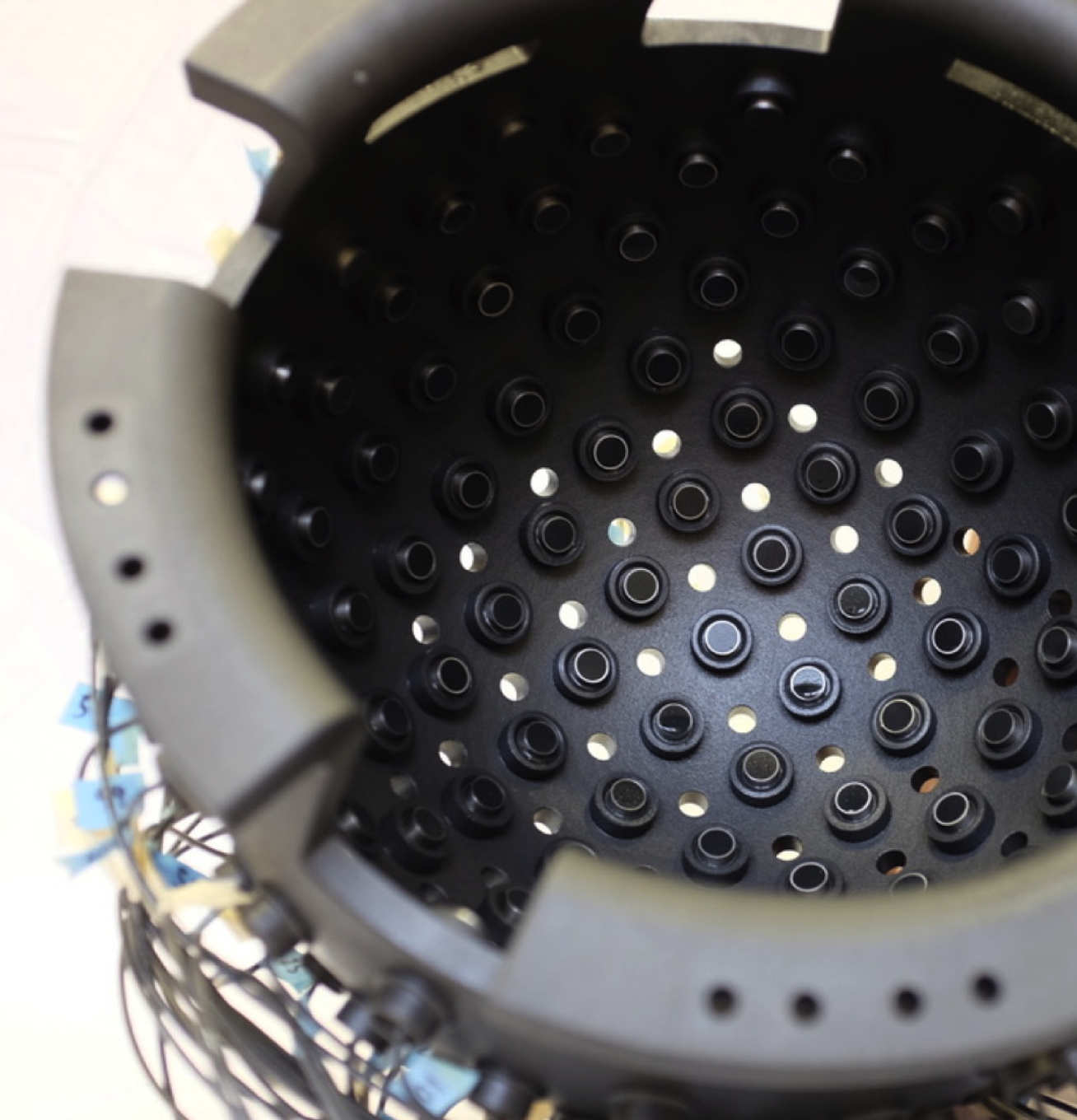
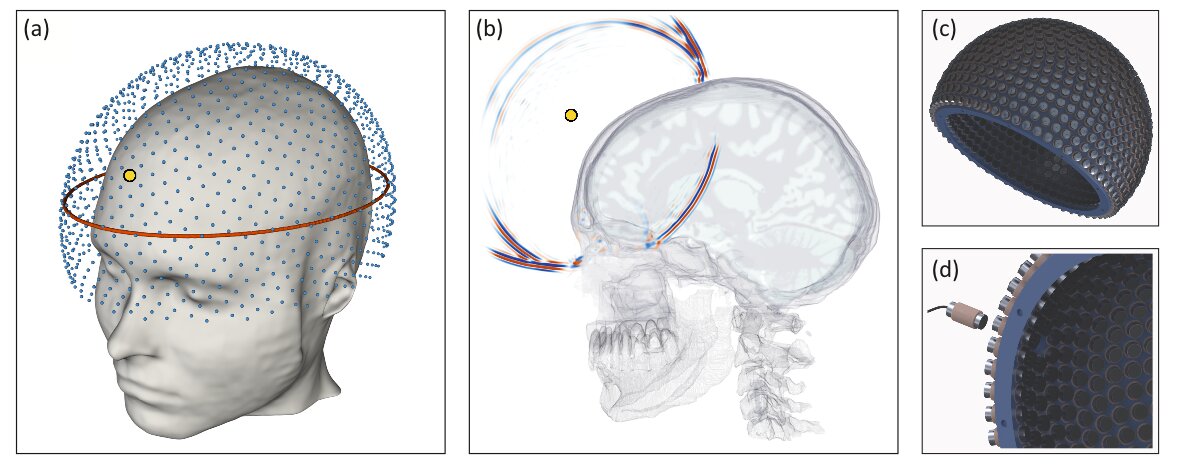
They built a helmet lined with an array of acoustic transducers that each sends sound waves through the skull. The ultrasound energy that propagates through the head is recorded and fed via the helmet into a computer. FWI is then used to analyse the reverberations of the sound throughout the skull, constructing a 3-D image of the interior.
The researchers tested their helmet on a healthy volunteer and found that the quality of the recorded signals was sufficient for the algorithm to generate a detailed image, and they are confident the scattered energy from the brain will be interpretable.
Using computer modelling, they also found they could obtain high-resolution images with sound frequencies low enough to penetrate the skull at safe intensities.
They created detailed computer simulations based on the properties of different types of human brain tissue to establish that sound waves would be effective for composing high-resolution images of the brain.
Dr. Guasch said: “This is the first time FWI has been applied to the task of imaging inside a human skull. FWI is normally used in geophysics to map the structure of the Earth, but our collaborative, multidisciplinary team of earth scientists, bioengineers and neurologists are using it to create a safe, cheap and portable method of generating 3-D ultrasound images of the human brain.”
Potential clinical use
Magnetic Resonance Imaging (MRI) is generally the best method for obtaining high-resolution images of the brain, and its use is currently essential to the investigation of many neurological disorders including stroke, brain cancer, and brain injury.
Nonetheless, MRI requires large, complex, expensive, non-portable machines cooled to three degrees above absolute zero, and it cannot be used on patients for whom the presence of metallic implants or foreign bodies cannot be scrupulously ruled out. This makes emergency use in patients with potentially altered consciousness, such as those suspected of stroke, difficult or impossible.
The researchers say that if it proves successful in human trials, their device will overcome these obstacles.
Study co-author Professor Parashkev Nachev, of UCL, said: “This is a vivid illustration of the remarkable power of advanced computation in medicine. Combining algorithmic innovation with supercomputing could enable us to retrieve high-resolution images of the brain from safe, relatively simple, well-established physics: the transmission of soundwaves through human tissue.
“The practicalities of MRI will always limit its applicability, especially in the acute setting, where timely intervention has the greatest impact. Neurology has been waiting for a new, universally applicable imaging modality for decades: full-waveform inversion could well be the answer.”
Next, the researchers will build a new prototype for live imaging of normal human brains as the first step to a device that could be evaluated in clinical contexts.
The use of ultrasound imaging
in intensive care and peri- operative medicine has increased
enormously over the past decades. Brain
ultrasonography, used to assess brain parenchyma and cerebral blood flow (CBF), is a generally
safe, non-invasive and relatively low-cost neuromoni- toring method that is
easily applicable at the bedside. Potentially,
it could provide
crucially important informa- tion in the early detection and
monitoring of neurologi- cal diseases, and to allow bedside assessment of cerebral
haemodynamics in critically ill patients.
It can be applied in a range of settings, including neuro- intensive and general intensive care units, the operating room and the emergency department. At present, how- ever, brain ultrasonography is not routinely performed in critical care settings. The aim of this review is to provide a brief overview of the physical and anatomical principles underlying brain ultrasonography, and of its potential clinical applications.
The techniques
Basically, two brain ultrasound techniques are currently available: B-mode transcranial colour-coded duplex (TCCD) and transcranial Doppler (TCD) sonogra phy. TCD, introduced in clinical practice approximately 40 years ago [1], identifies the cerebral arteries “blindly”, on the basis of the spectral display and standard criteria (including arterial depth, arterial blood flow direction and waveform analysis). It allows assessment and contin- uous monitoring of CBF velocity, and is thus an excellent technique for use in multimodal brain monitoring and evaluation of basic and advanced parameters. Advanced parameters such as cerebral autoregulation, critical closing pressure and cerebral compliance can be assessed with TCD, and it can also be used to perform functional tests for evaluating cerebrovascular reactivity [2].
TCCD, which combines colour-coded Doppler vessel representation with bi-dimensional pulsed-wave Dop- pler ultrasound imaging, has further improved the above technique, allowing direct visualisation and better iden- tification of the cerebral arteries. TCCD is therefore a newer, more technically advanced tool, and it is useful for high-precision freehand real-time scanning and haemo- dynamic assessment of the brain. While it permits direct visualisation of the brain parenchyma and vessels, it does not allow prolonged continuous monitoring of CBF.
TCCD is usually performed using a 2–2.5-MHz probe that allows visualisation of the main cerebral structures and vessels. On duplex imaging, the midbrain can be identified through the transtemporal window (Fig. 1), and individual arteries of the circle of Willis can be then visualised. Each artery is identified by its depth and blood flow direction in relation to the probe and other visualised arteries. TCCD can provide basic informa- tion regarding blood flow velocity (systolic, diastolic and mean values) in an insonated artery, as well as the pulsa- tility index (PI).

This review focuses mainly on the expanding clini- cal applications of TCCD. The basic conditions allowing a complete TCCD-based brain examination (including normal anatomy and insonation windows, and normal blood flow velocity patterns of the cerebral arteries), as well as acquisition techniques and interpretation of images, are described in Figs. 1 and 2 and electronic sup- plementalmaterial (ESM1a–e). Basic and advanced TCD- derived parameters are described in detail in ESM2.
Clinical applications
Table 1 summarises all the clinical applications of brain ultrasonography. Below, we analyse the most common ones in the neurocritical care, general intensivecare unit (ICU), emergency department and prehospital medicine settings.
Brain ultrasonography in neurocritical care
Brain ultrasonography can be used in a wide range of clinical applications in neurocritical care, and the main ones are listed below. In general, although we recom- mend implementation of this technique in clinical prac- tice, we also suggest that it should not replace invasive neuromonitoring techniques [such as invasive intracra- nial pressure (ICP) monitoring] or substitute diagnostic tools such as computed tomography (CT) or magnetic resonance imaging (MRI).
Take‑home message
Brain ultrasonography enables assessment of the main structures of the brain, including the parenchyma and major cerebral vessels.
Brain ultrasonography can be performed using commonly used ultra- sound systems, through four main acoustic windows (transtemporal, occipital, submandibular and transorbital).
Brain ultrasonography can be used for rapid bedside assessment of pathological changes in neurocritically ill patients, allowing, for exam- ple, evaluation of intracerebral haematomas, estimation of raised intrac- ranial pressure, and detection of midline shift and intracranial masses.
Brain ultrasonography is not used exclusively in neurocritical care; clinical applications have been described in different settings, including general intensive care and the emergency department.
Brain ultrasonography in the emergency department and prehospital medicine
The bedside availability and dynamic nature of ultra- sound techniques are two features that make them appealing in the emergency department and/or in pre- hospital scenarios as potential sources of real-time infor- mation on cerebral physiology.
Brain ultrasonography within the whole‑body ultrasound approach in multiple trauma
Ever since the introduction, in the prehospital setting and emergency room, of the focused assessment with sonogra- phy for trauma (FAST) protocol [90] and the further devel- opment of its paradigm into a multi-organ approach [91, 92], point-of-care ultrasound (PoCUS) has become a widely used and extensively taught approach for the rapid evalua- tion of acute trauma patients.
PoCUS involves multi-site investigation, and includes cardio-thoracic, abdominal, vas- cular and skeletal scans (Fig. 6), and it aims to detect life- threatening lesions and provide immediate assessment of the pathophysiology of the haemodynamic impairment [91]. Due to obvious technical limitations, both the prehospital
scenario and the emergency department share a lack of information on ICP. TCCD screening for signs of intracra- nial hypertension could potentially fill this gap.
In a prospective multicentre study, TCD upon emer- gency department admission was able to predict neuro- logical worsening after mild to moderate TBI with good sensitivity and specificity [92].
Although evidence on the prehospital feasibility and benefits of brain ultrasonogra- phy is still lacking, its role within the multi-organ PoCUS approach to trauma, namely to determine the need for neurosurgical care and allow the early implementation of neuroprotective strategies, is noteworthy.
Preliminary data suggest that high-quality measurements of ONSD in the ambulance or helicopter, conducted to estimate the risk of raised ICP in TBI, are feasible [93]. In TBI patients,
TCCD-estimated MLS demonstrated a mean difference of 0.12 ± 1.08 mm (95% CI, 0.15–0.41 mm, p = 0.36), a
linear correlation of 0.88 (p < 0.0001), no significant bias and limits of agreement of +2.33 to −2.07 mm when compared with CT scan images [94]. TCD may also allow early detection of low CBF by detecting low MCA dias- tolic flow velocities and high PI values.
In a pilot feasibil- ity study, Tazarourte et al. [95] performed prehospital MCA TCD in severe TBI patients with the aim of improv- ing cerebral perfusion by using an early goal-directed approach (norepinephrine infusion if PI was > 1.4 and MAP was < 80 mmHg; mannitol administration if PI was > 1.4 and MAP was > 80 mmHg).
Although no statisti- cally significant conclusions can be drawn from this small prospective study (nine patients with PI > 1.4), normali- sation of TCD flows was obtained in the majority of the treated patients. Finally, a recently published multicentre prospective pilot study conducted in 38 ICU patients sug- gested that TCD could be used as an early tool to rule out raised ICP in severe TBI.
In this study, Rasulo et al. [96], by comparing TCD-estimated ICP with invasive ICP moni- toring, showed that TCD can detect ICP > 20 mmHg with high sensitivity. According to these results, TCCD can be useful not to assess ICP as a number, but to safely exclude patients with intracranial hypertension.
In all the above-mentioned settings, standardisation of clinical practice of brain ultrasonography and research is warranted. Data on clinical studies regarding the ultra- sound-based management of patients are lacking, as is a standardised training and certification process.
A panel of neurointensive care experts is currently finalising a consensus aimed at providing recommendations that will pave the way for standardisation of minimal require- ments for brain ultrasonography and of the different lev- els of skills required. Also, several teaching programmes and courses are now being developed.
Other specific considerations, including application in the paediatric setting and in pregnancy, are described in ESM12–15. Possible pitfalls and artefacts of brain ultra- sonography, as well as its safety limitations, are described in ESM16.

Conclusions
Brain ultrasonography is a non-invasive, low-cost, gen- erally safe and readily available technique, which can potentially be used at the bedside for both diagnosis and monitoring of patients with brain insults. Assessment of brain anatomy and TCCD-derived indices may provide important bedside information regarding the onset and evolution of several cerebrovascular conditions and facil- itate their clinical management. Brain ultrasonography is an evolving field; although there is a need for further clin- ical development, and research and training and teaching programmes are still lacking, efforts are now being made to address these gaps.
Despite presenting several limitations, brain ultra- sonography has a strong potential for the assessment of cerebral haemodynamics in critically ill patients in many clinical settings.
More information: “Full-waveform inversion imaging of the human brain” by Lluís Guasch, Oscar Calderón Agudo, Meng-Xing Tang, Parashkev Nachev and Michael Warner, published 6 March 2020 in npj Digital Medicine. www.nature.com/articles/s41746-020-0240-8



{kind=link}