










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")


While researchers are certain that coronavirus spreads through mucus and droplets expelled by coughing or sneezing, it is unclear if the virus is spread through other bodily fluids, such as tears.
Today’s just-published study offers evidence that it is unlikely that infected patients are shedding virus through their tears, with one important caveat.
None of the patients in the study had conjunctivitis, also known as pink eye.
However, health officials believe pink eye develops in just 1 percent to 3 percent of people with coronavirus.
The study’s authors conclude that their findings, coupled with the low incidence of pink eye among infected patients, suggests that the risk of virus transmission through tears is low.
Their study was published online today in Ophthalmology.
To conduct the study, Ivan Seah, MBBS, and his colleagues at the National University Hospital in Singapore collected tear samples from 17 patients with COVID-19 from the time they showed symptoms until they recovered about 20 days later.
Neither viral culture nor reverse transcription polymerase chain reaction (RT-PCR) detected the virus in their tears throughout the two-week course of the disease.
Dr. Seah also took samples from the back of the nose and throat during the same time period. While the patients’ tears were clear of virus, their noses and throats were teeming with COVID-19.
Dr. Seah said he hopes their work helps to guide more research into preventing virus transmission through more significant routes, such as droplets and fecal-oral spread.
While the patients’ tears were clear of virus, their noses and throats were teeming with COVID-19.
Despite this reassuring news, it’s important for people to understand that guarding your eyes — as well as your hands and mouth — can slow the spread of respiratory viruses like the coronavirus.
Here’s why:
- When a sick person coughs or talks, virus particles can spray from their mouth or nose into another person’s face. You’re most likely to inhale these droplets through your mouth or nose, but they can also enter through your eyes.
- You can also become infected by touching something that has the virus on it — like a table or doorknob — and then touching your eyes.
Coronaviruses: what are they?
Coronaviruses (CoV) belong to the subfamily Coronavirinae, in the family Coronaviridae of the order Nidovirales. There are four genera: Alphacoronavirus, Betacoronavirus, Gammacoronavirus and Deltacoronavirus [3].
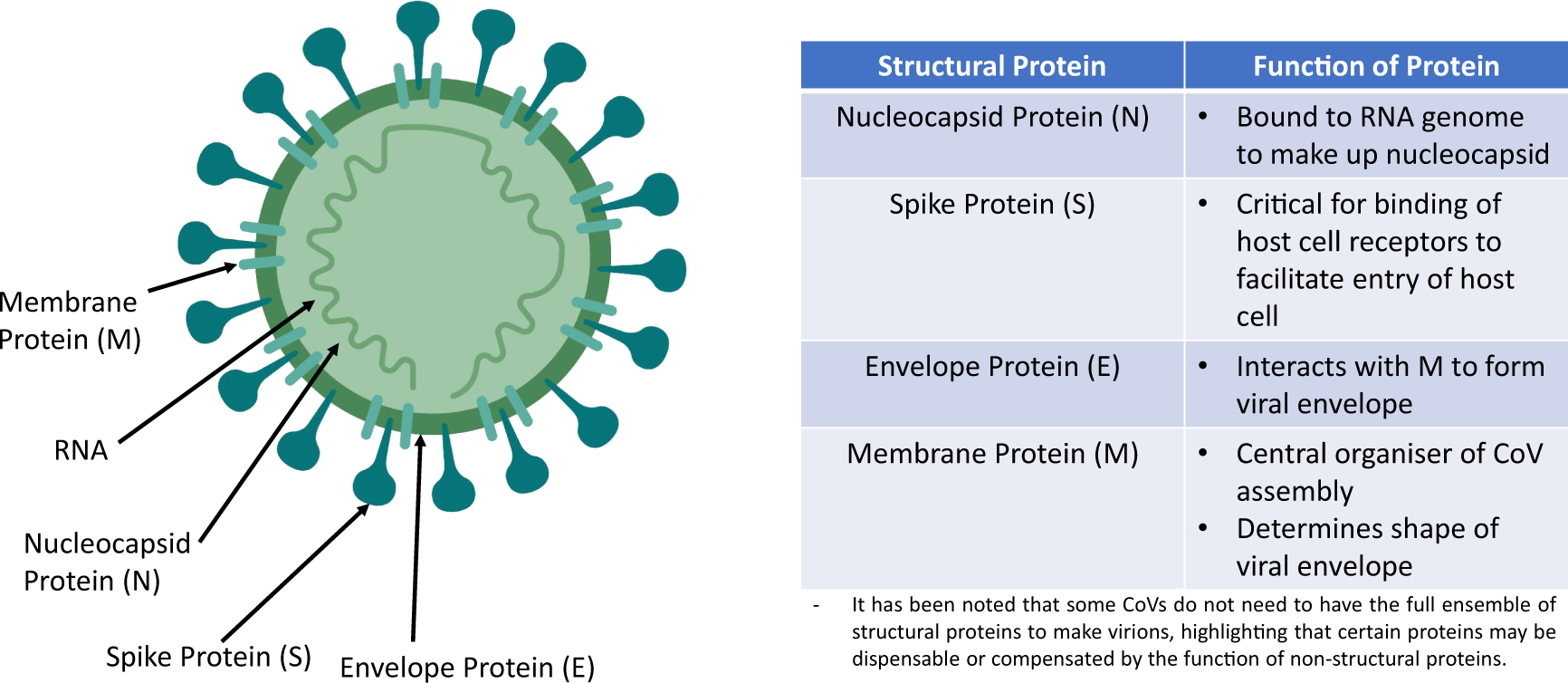
It is a single positive-sense RNA virus. Mutation rates of RNA viruses are greater than DNA viruses, suggesting a more efficient adaptation process for survival. The genome codes for at least four main structural proteins: spike (S), membrane (M), envelope (E), nucleocapsid (N) proteins and other accessory proteins which aid the replicative processes and facilitate entry into cells [4].
Figure 1 summarises the coronavirus’s structure and the function of the structural proteins. CoVs mainly affect birds and mammals. Prior to 2019, there were only six CoVs that can infect human and cause respiratory diseases: HCoV-229E, HCoV-OC43, HCoV-NL63, HKU1, SARS-CoV, MERS-CoV. The last 2 are capable of causing severe respiratory syndrome in humans.
From: Revisiting the dangers of the coronavirus in the ophthalmology practice
A possible threat in the ophthalmology clinic
While the 2019-nCoV transmission route is still unknown, countries have been preparing measures based on past experiences with coronaviruses namely SARS-CoV and MERS-CoV.
These viruses transmit primarily through droplets and other bodily secretions. In the ophthalmology practice, healthcare workers may be particularly susceptible to these infections.
Firstly, ophthalmologists are extremely reliant on physical examination during patient consultation. Of particular concern is the proximity between the patient and ophthalmologist during the slit lamp microscope examination.
It has been shown that droplets from a cough or sneeze can be propelled for up to 6 m [8], a range that definitely encompasses the distance between the patient and ophthalmologist.
Secondly, during the SARS-CoV epidemic, clinical reports have suggested tears as a medium of infection. In a case series by Loon et al., it was shown that viral RNA of the SARS-CoV can be detected by reverse-transcription polymerase chain reaction (RT-PCR) from the tears of infected individuals [9].
While anecdotal in nature, such accounts highlight the possible infectivity of tears, a fluid which ophthalmologists and instruments come in contact on a daily basis.
If true, this represents a crucial need for further development of disinfection and personal protective equipment (PPE) protocols for the ophthalmology clinic.
Bringing back strategies to prevent transmission
In view of the potential threat in the ophthalmology practice, it may be prudent to revisit the strategies that successfully curbed the transmission of SARS in 2003 [10]. With particular relevance to the ophthalmic practice, it may be beneficial to triage patients according to produced surveillance case definitions [11].
In 2003, the WHO launched a case classification scheme which triaged patients into general, suspect and probable categories. Ophthalmology practices in Hongkong, a country badly hit by SARS, recommended the full PPE for all cases regardless of SARS status.
For suspect and probable cases, appointments were recommended to be deferred unless in the event of an ophthalmic emergency. These patients were seen in an isolation ward.
An emphasis on hand hygiene measures and stocking up of PPE such as N95 masks, gloves, gowns and googles should also be considered while the mode of transmission is being identified. Decontamination and sterilisation protocols of clinical rooms and equipment should also be improved on as coronaviruses have been found to survive in environments outside the body for a long time [12].
For instance, it is still not established if higher concentrations of dilute bleach (1:10), a chemical used to sterilise the Goldmann applanation tonometer, can be utilised to eliminate coronaviruses [13].
Other shared equipment like the B-scan probe and contact lenses for photocoagulation will also need strict sterilisation protocols. Finally, the reduction of non-urgent ophthalmic operations should also be considered as the risk of viral transmission may outweigh the surgical benefits.
For emergency operations, full PPE can be considered to reduce the probability of healthcare transmission.
As the WHO Director-General, Tedros Adhanom Ghebreyesus highlighted, “Make no mistake: this is an emergency in China. But it has not yet become a global health emergency. It may yet become one.”
It is currently very difficult to predict the eventual impact of the 2019-nCoV. However, it will be prudent to utilise the lessons gained from SARS-CoV and prepare for the worst. Until a vaccine is created, public health strategies are likely the best weapons against the enemy.
References
- 1.Bloomberg News. China will rack up three billion trips during world’s biggest human migration. Bloomberg News; January 2020.
- 2.WHO. Summary table of SARS cases by country, 1 November 2002–7 August 2003. World Health Organisation (WHO); 2003.
- 3.Chen Y, Liu Q, Guo D. Coronaviruses: genome structure, replication, and pathogenesis. J Med Virol. [e-pub ahead].
- 4.Schoeman D, Fielding BC. Coronavirus envelope protein: current knowledge. Virol J 2019;16:69.
- 5.WHO. Pneumonia of unknown cause—China. 2020. https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/.
- 6.Hui DS, E IA, Madani TA, Ntoumi F, Kock R, Dar O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis 2020;91:264–6.
- 7.Javier C, Hernández AR. China confirms new coronavirus spreads from humans to humans. America: The New York Times; 2020.
- 8.Xie X, Li Y, Chwang AT, Ho PL, Seto WH. How far droplets can move in indoor environments–revisiting the Wells evaporation-falling curve. Indoor Air. 2007;17:211–25.
- 9.Loon S-C, Teoh SCB, Oon LLE, Se-Thoe S-Y, Ling A-E, Leo Y-S, et al. The severe acute respiratory syndrome coronavirus in tears. Br J Ophthalmol. 2004;88:861–3.
- 10.Chan WM, Liu DT, Chan PK, Chong KK, Yuen KS, Chiu TY, et al. Precautions in ophthalmic practice in a hospital with a major acute SARS outbreak: an experience from Hong Kong. Eye (Lond). 2006;20:283–9.
- 11.WHO. Global Surveillance for human infection with novel coronavirus (2019-nCoV). World Health Organisation; 2020 https://www.who.int/publications-detail/global-surveillance-for-human-infection-with-novel-coronavirus-(2019-ncov).
- 12.Casanova LM, Jeon S, Rutala WA, Weber DJ, Sobsey MD. Effects of air temperature and relative humidity on coronavirus survival on surfaces. Appl Environ Microbiol. 2010;76:2712–7.
- 13.Sizun J, Yu MW, Talbot PJ. Survival of human coronaviruses 229E and OC43 in suspension and after drying onsurfaces: a possible source ofhospital-acquired infections. J Hosp Infect. 2000;46:55–60.
Affiliations
- Department of Ophthalmology, National University Hospital, Singapore, Singapore
- Ivan Seah
- , Xinyi Su
- & Gopal Lingam
- Institute of Molecular and Cell Biology (IMCB), Agency for Science, Technology and Research (A*STAR), Singapore, Singapore
- Xinyi Su
- Department of Ophthalmology, Yong Loo Lin School of Medicine, National University Singapore, Singapore, Singapore
- Xinyi Su
- & Gopal Lingam



{kind=link}
[…] COVID-19: researchers are certain that the risk of transmission through tears… […]