










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



One of the defining features of COVID-19 is the excessive immune response that can occur in severe cases.
This burst of immune overreaction, also called a cytokine storm, damages the lungs and can be fatal.
A team of MIT researchers has developed specialized proteins, similar in structure to antibodies, that they believe could soak up these excess cytokines.
“The idea is that they can be injected into the body and bind to the excessive cytokines as generated by the cytokine storm, removing the excessive cytokines and alleviating the symptoms from the infection,” says Rui Qing, an MIT research scientist who is one of the senior authors of the study.
The researchers have reported their initial findings in the journal Quarterly Review of Biophysics (QRB) Discovery, and they now hope to begin testing their proteins in human cells and in animal models of cytokine release and coronavirus infection.
Shuguang Zhang, a principal research scientist in the MIT Media Lab’s Laboratory of Molecular Architecture, is also a senior author of the paper. Shilei Hao, a visiting scientist at MIT, is the lead author of the study, and David Jin, CEO and president of Avalon GloboCare, is also an author.
A molecular sponge
The researchers’ work on blocking cytokine storms grew out of a project that Zhang began 10 years ago to develop modified versions of membrane-embedded proteins.
These proteins are usually difficult to study because once they are extracted from the cell membrane, they only maintain their structure if they are suspended in special types of detergents.
After working on the problem for several years, Zhang and Qing developed a method for modifying the hydrophobic regions of these proteins, making them soluble in water and much easier to study.
Their method, called the QTY code, calls for replacing some hydrophobic amino acids with hydrophilic amino acids that have similar structures.
Leucine is converted to glutamine, isoleucine and valine are converted to threonine, and phenylalanine is converted to tyrosine.
Following the development of the QTY code, Jin approached Zhang’s lab with the idea of designing water-soluble versions of proteins known as cytokine receptors.
These receptors are found on the surface of immune cells, where they bind to cytokines — signaling proteins that stimulate inflammation and other immune responses.
Jin believed that proteins that mimic these cytokine receptors could help combat cytokine storms, which can be produced by viral or bacterial infections, including HIV and hepatitis. They can also occur as a side effect of cancer immunotherapy.
In April 2019, Zhang’s team set out to design proteins that could sop up these excess cytokines like a sponge.
To do that, they used the QTY code to make water-soluble versions of cytokine receptors. When proteins are soluble in water, they can travel efficiently through the human bloodstream, while the original, hydrophobic versions of the proteins would likely stick to cells that they encountered.
The researchers also attached an antibody segment called the Fc region to their water-soluble receptor proteins.
This region helps to further stabilize the proteins in the bloodstream, and makes them less likely to be attacked by the immune system.
The researchers designed proteins that mimic six different cytokine receptors, which can bind to cytokines such as interferon and interleukin, as well as a class of cytokines called chemokines.
In laboratory tests of the proteins’ binding strength, the researchers found that their modified proteins were able to bind to cytokines with similar strength as naturally occurring cytokine receptors.
Driven by curiosity
In March, when evidence began to suggest that the SARS-CoV-2 virus was inducing cytokine storms in some patients, the researchers realized that the receptor proteins they had designed might be able to help.
They decided to quickly publish the results they have generated so far, and they are now planning to do additional tests in human cells and in animal models of Covid-19 infection.
The potential usefulness of this approach underscores the importance of “curiosity-driven research,” Zhang says.
“As it turns out, our research initiated in April 2019 is directly relevant to the treatment of Covid-19 infected patients,” he says. “Curiosity-driven, or even proactive research often leads to preparedness, which is key to preventing future disasters.”
The researchers have filed for patents on the proteins that they designed, as well as on their overall approach to creating water-soluble cytokine receptors.
They hope to license the technology quickly and to collaborate with pharmaceutical and biotech companies who can help to move it toward clinical trials.
“Obviously this approach will need further animal studies, and potentially human clinical studies,” Jin says. “But we have confidence that this discovery will contribute to clinical applications to address viral diseases that involve cytokine storms.”
Funding: The research was funded primarily by Avalon GloboCare, and also by a fellowship from the China Scholarship Council and Chongqing University, China.
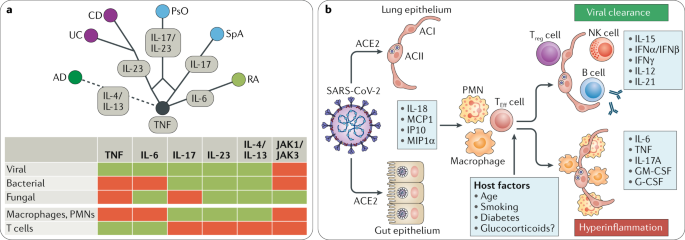
Immune-mediated inflammatory diseases (IMIDs) often affect the inner and outer barriers of the body, such as the joints (rheumatoid arthritis (RA) and spondyloarthritis (SpA)), the gut (Crohn’s disease (CD) and ulcerative colitis (UC)) and the skin (psoriasis (PsO) and atopic dermatitis (AD)).
Treatment of IMIDs has developed rapidly in the past few years owing to better molecular profiling and the use of targeted interventions that neutralize disease-specific pro-inflammatory cytokines.
In RA, the inhibition of TNF and IL-6R is effective, whereas SpA responds to inhibition of TNF and IL-17A. In CD and UC, TNF and IL-23 are the main effector cytokines. PsO is responsive to inhibition of TNF, IL-17A and IL-23, while inhibition of IL-4 and IL-13 works in AD1 (Fig. 1).
Despite differences in the target organs and the cytokine repertoires among individual IMIDs, commonalities exist, which are reflected by an exaggerated and sustained innate and adaptive immune response.
In many forms of IMID, independent of the target organ or whether they are initiated via T helper 1 (TH1), TH17 or TH2 cell activation, infiltration of target tissues with large numbers of innate immune cells such as granulocytes and inflammatory macrophages is a hallmark.
Coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus2, leads to fast activation of innate immune cells, especially in patients developing severe disease.
Circulating neutrophil numbers are consistently higher in survivors of COVID-19 than in non-survivors, and the infection also induces lymphocytopenia that mostly affects the CD4+ T cell subset, including effector, memory and regulatory T cells3.
Reflecting innate immune activation, levels of many pro-inflammatory effector cytokines, such as TNF, IL-1β, IL-6, IL-8, G-CSF and GM-CSF, as well as chemokines, such as MCP1, IP10 and MIP1α, are elevated in patients with COVID-19, with higher levels in those who are critically ill. In addition, the levels of some T cell-derived cytokines, such as IL-17, are increased in the context of SARS-CoV-2 infection4.
SARS-CoV-2 infection drives a profound cytokine response in the host, comprising a series of mediators that are targeted in IMIDs (Fig. 1). In some patients with COVID-19, a cytokine storm develops that resembles secondary haemophagocytic lymphohistiocytosis, a hyperinflammatory state triggered by viral infections5.
Although the bulk of cytokines induced by SARS-CoV-2 infection as well as those being targeted in the various aforementioned IMIDs are important to mount inflammation, they do not seem to be essential for controlling virus clearance.
Targeting IL-23 and IL-4/IL-13 does not increase the risk for viral, bacterial or fungal infections, while inhibition of IL-17A only shows a signal for Candida species but not for viral infection. Targeting TNF and IL-6 increases the risk of bacterial infections but has lesser effects on viral infections (except for hepatitis B activation).
Notably, although the incidence of influenza and the risk of developing complications from influenza infection are higher for patients with RA and CD, no signal associated with cytokine inhibitors was found6.
Also, patients with RA or CD achieve normal immune responses to influenza vaccination when treated with anti-TNF agents, further supporting the concept that the effector cytokines induced by SARS-CoV-2 and targeted for treatment of IMIDs are critical for the inflammatory response but not for viral clearance7. Viral clearance seems to primarily depend on other cytokines such as IL-15, type I interferons and IFNγ.
Targeting pro-inflammatory cytokines with antibodies such as adalimumab, dupilumab, infliximab, ustekinumab, secukinumab and tocilizumab is clinical routine in IMIDs. Potential risk and benefits of cytokine inhibition need to be carefully addressed in order to recommend whether to continue or stop such treatments.
Although at first sight cytokine inhibition might be considered as ‘immune suppression’ and therefore harmful in the context of the COVID-19 pandemic, these compounds neutralize individual mediators of the inflammation cascade rather than leading to broad immune suppression.
On the other hand, cytokine inhibitors may mitigate the hyperinflammatory state, which is part of the pathogenesis of severe COVID-19. Indeed, studies using IL-6R and IL-6 inhibitors in COVID-19 have just been launched. Hence, approaches that do not affect viral clearance but inhibit hyperinflammatory host responses may exert beneficial effects in COVID-19.
Although targeting individual cytokines (TNF, IL-6, IL-17A, IL-23 or IL-4/IL-13), in contrast to glucocorticoids8, does not appear to increase viral infection rates or induce a more severe course of viral infection, the inhibition of multiple cytokines, for example, targeting interferon responses, may be different. Janus kinase (JAK) inhibitors, which target JAK1 and JAK3, developed for treatment of RA, CD and PsO show an increased risk for herpes zoster reactivation. T
argeting JAK1 and JAK3 affects the function of several cytokines that are involved in antiviral responses such as type I interferons, IL-2, IL-15, IL-21 and IFNγ. Hence JAK1/JAK3 inhibitors could theoretically inhibit the clearance of SARS-CoV-2. On the other hand, JAK2 inhibition appears to block viral entry of SARS-CoV-2 and IL-17-induced cytokine activation9.
Notably, IL-6 and GM-CSF, which are both induced by SARS-CoV-2, partly or fully depend on JAK2 signalling, suggesting that JAK2 could be a target in treating hyperinflammatory response in COVID-19.
At present, there is very limited experience on how COVID-19 affects patients with IMIDs treated with cytokine inhibitors. Nonetheless, a critical analysis of the role of pro-inflammatory cytokines in the pathophysiology of COVID-19 and of the risk of viral infection during anti-cytokine therapy suggests that most cytokine inhibitors may not automatically put patients with IMIDs at higher risk of developing severe COVID-19.
In accordance, most ad hoc recommendations from specialists in the fields of gastroenterology, rheumatology and dermatology do not support pre-emptively stopping anti-cytokine therapy if no signs of COVID-19 are present. Remarkably, some cytokine inhibition strategies are currently being tested for the treatment of COVID-19, and hydroxychloroquine, a long-known drug used for the treatment of IMIDs, seems to show efficacy in COVID-19 (ref.10).
Apart from these trials, IMID registers are currently being built up that will help to better understand the impact of COVID-19 in patients with autoimmune disease and to potentially uncover a protective role of certain cytokine inhibition strategies.
References
- Schett, G. et al. How cytokine networks fuel inflammation: toward a cytokine-based disease taxonomy. Nat. Med. 19, 822–824 (2013).
- Wu, F. et al. A new coronavirus associated with human respiratory disease in China. Nature 579, 265–269 (2020).
- Wang, D. et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323, 1061–1069 (2020).
- Huang, C. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395, 497–506 (2020).
- Pedersen, S. F. & Ho, Y. C. A storm is raging. J. Clin. Invest. https://doi.org/10.1172/JCI137647 (2020).
- Blumentals, W. A., Arreglado, A., Napalkov, P. & Toovey, S. Rheumatoid arthritis and the incidence of influenza and influenza-related complications: a retrospective cohort study. BMC Musculosskelet. Disord. 13, 158 (2012).
- Andrisani, G. et al. Immune response to influenza A/H1N1 vaccine in inflammatory bowel disease patients treated with anti TNF-α agents: effects of combined therapy with immunosuppressants. J. Crohns Colitis 7, 301–307 (2013).
- Russell, C. D., Millar, J. E. & Baillie, J. K. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet 395, P473–P475 (2020).
- Wu, D. & Yang, X. O. TH17 responses in cytokine storm of COVID-19: an emerging target of JAK2 inhibitor fedratinib. J. Microbiol. Immunol. Infect. https://doi.org/10.1016/j.jmii.2020.03.005 (2020).
- Chen, Z. et al. Efficacy of hydroxychloroquine in patients with COVID-19: results of a randomized clinical trial. Preprint at medRxiv https://doi.org/10.1101/2020.03.22.20040758 (2020).
Source:
MIT
Nature – Schett, G., Sticherling, M. & Neurath, M.F. COVID-19: risk for cytokine targeting in chronic inflammatory diseases?. Nat Rev Immunol (2020). https://doi.org/10.1038/s41577-020-0312-7



{kind=link}