










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



According to many experts, early diagnosis and management is critical for slowing the spread of SARS-CoV-2, the new coronavirus that causes COVID-19.
Therefore, the race is on to develop diagnostic tests for the virus that are faster, easier and more accurate than existing ones.
Now, researchers reporting in ACS Nano have developed a field-effect transistor-based biosensor that detects SARS-CoV-2 in nasopharyngeal swabs from patients with COVID-19, in less than one minute.
Currently, most diagnostic tests for COVID-19 rely on a technique called real-time reverse transcription-polymerase chain reaction (RT-PCR), which amplifies SARS-CoV-2 RNA from patient swabs so that tiny amounts of the virus can be detected.
However, the method takes at least 3 hours, including a step to prepare the viral RNA for analysis.
Edmond Changkyun Park, Seung Il Kim and colleagues wanted to develop a faster diagnostic test that could analyze patient samples directly from a tube of buffer containing the swabs, without any sample preparation steps.
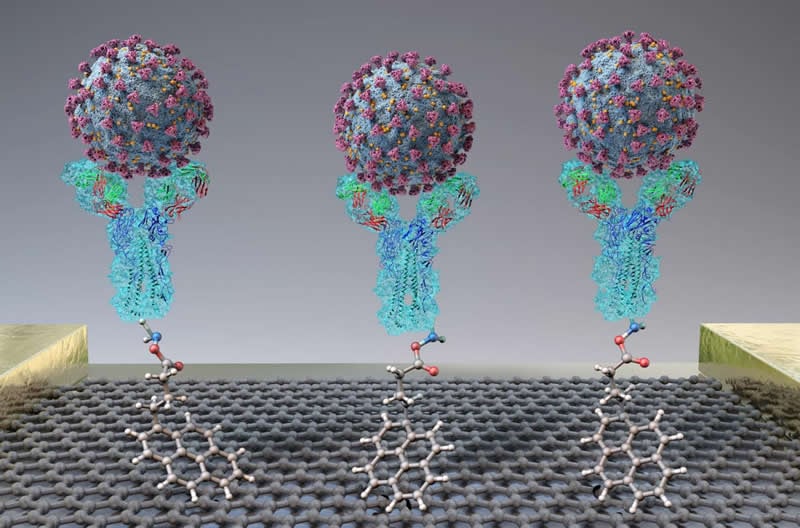
The team based their test on a field-effect transistor — a sheet of graphene with high electronic conductivity.
The researchers attached antibodies against the SARS-CoV-2 spike protein to the graphene.
When they added either purified spike protein or cultured SARS-CoV-2 virus to the sensor, binding to the antibody caused a change in the electrical current.
Next, the team tested the technique on nasopharyngeal swabs collected from patients with COVID-19 or healthy controls.
Without any sample preparation, the sensor could discriminate between samples from sick and healthy patients.
The new test was about 2-4 times less sensitive than RT-PCR, but different materials could be explored to improve the signal-to-noise ratio, the researchers say.
Funding: The authors acknowledge funding from the National Research Council of Science and Technology funded by the Ministry of Science and ICT, Korea and the Korea Health Technology R&D Project through the Korea Health Industry Development Institute funded by the Ministry of Health & Welfare, Korea.
Coronaviruses (CoVs) cause mild to moderate upper respiratory tract illnesses in both humans and animals.(7) SARS-CoV-2, a betacoronavirus, has a single-positive strand RNA genome.
CoV genomes encode four structural proteins: spike (S), envelope (E), matrix (M), and nucleocapsid (N). Two betacoronaviruses, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), caused serious epidemics over the past two decades.(8) Phylogenetic analysis revealed that SARS-CoV-2 is more similar to SARS-CoV than MERS-CoV.(9)
Although the viral pathogenesis of SARS-CoV-2 is unknown, recent studies reported that SARS-CoV-2 uses angiotensin-converting enzyme II (ACE2) as a cellular entry receptor; ACE2 is also a well-known host cell receptor for SARS-CoV.(10) SARS-CoV-2 colocalizes with ACE2 in animal cells,(11) and its spike (S) protein binds ACE2 with high affinity.(12,13)
For emerging pathogens, real-time reverse transcription–polymerase chain reaction (RT-PCR) is the primary means of diagnosis. Currently, real-time RT-PCR is used for the detection of SARS-CoV-2 based on previously published laboratory protocols.(14) SARS-CoV-2 is highly contagious and is currently spreading rapidly around the world; the rate of COVID-19 transmission is much faster than those of SARS and MERS.
Moreover, cases of asymptomatic COVID-19 transmission have been reported.(15,16) Molecular diagnosis using real-time RT-PCR takes at least 3 h, including preparation of viral RNA. In addition, the RNA preparation step can affect diagnostic accuracy.
Hence, highly sensitive immunological diagnostic methods that directly detect viral antigens in clinical samples without sample preparation steps are necessary for rapid and accurate diagnosis of COVID-19.
Among the many diagnostic methods currently available, field-effect transistor (FET)-based biosensing devices have several advantages, including the ability to make highly sensitive and instantaneous measurements using small amounts of analytes.(17,18) FET-based biosensors are considered to be potentially useful in clinical diagnosis, point-of-care testing, and on-site detection.
Graphene is a two-dimensional sheet of hexagonally arranged carbon atoms, all of which are exposed on its surface.(19) It has proven to be a useful material for various sensing platforms due to its extraordinary properties, including high electronic conductivity, high carrier mobility, and large specific area.(20)
Graphene-based FET biosensors can detect surrounding changes on their surface and provide an optimal sensing environment for ultrasensitive and low-noise detection. From this standpoint, graphene-based FET technology is very attractive for applications related to sensitive immunological diagnosis.(21,22)
In this study, we developed a graphene-based biosensing device functionalized with SARS-CoV-2 spike antibody (COVID-19 FET sensor) for use as a SARS-CoV-2 virus detection platform. SARS-CoV-2 spike antibody was immobilized onto the fabricated device through 1-pyrenebutyric acid N-hydroxysuccinimide ester (PBASE), an efficient interface coupling agent used as a probe linker (Figure 1).
Our COVID-19 FET sensor detects target SARS-CoV-2 antigen protein with a limit of detection (LOD) of 1 fg/mL. Most critical of all, we confirmed the potential for clinical application by detecting SARS-CoV-2 antigen protein in transport medium used for nasopharyngeal swabs and cultured SARS-CoV-2 virus, as well as SARS-CoV-2 virus from clinical samples.
Furthermore, our sensor could distinguish the SARS-CoV-2 antigen protein from those of MERS-CoV. These results demonstrate the successful fabrication of a COVID-19 FET sensor based on integration of SARS-CoV-2 spike antibody with graphene, enabling highly sensitive detection of the SARS-CoV-2 virus in clinical samples.

Preparation of the COVID-19 FET Sensor
To evaluate the presence of the SARS-CoV-2 spike antibody on the graphene surface, we carried out electrical measurements. Figure 3C shows the current–voltage (I–V) curves of the graphene device over a range from −0.1 to +0.1 V before and after attachment of the antibody. After PBASE functionalization and immobilization of the antibody onto the graphene channel, the slopes (dI/dV) decreased. This difference in slope indicates the successful introduction of the SARS-CoV-2 spike antibody.
Figure 3

Figure 3. Electrical characterization of pristine, PBASE-modified, and SARS-CoV-2 spike antibody-immobilized graphene. (A) Schematic diagram of the aqueous-solution-gated FET (COVID-19 FET sensor) configuration using the antibody-conjugated graphene. (B) IDS–VDS output curves of the antibody-conjugated FET with various gating voltages from 0 to −1.5 V in steps of −0.3 V. IDS negatively increased as VGS negatively increased. (C) Current–voltage (I–V) characteristics of the graphene-based device of each functionalization process for the antibody modification. (D) Measurement of transfer curves of the COVID-19 FET sensor in steps of the antibody conjugation (VDS = 0.01 V).
To investigate the possibility of transducing an electrical signal with the COVID-19 FET sensor, we prepared an aqueous solution-gated FET.
The geometry of the COVID-19 FET sensor was designed using a graphene channel conjugated to the SARS-CoV-2 spike antibody, and the FET was covered with phosphate-buffered saline (PBS; pH 7.4) buffer as the electrolyte to maintain an efficient gating effect.
As shown in Figure 3A, the aqueous solution-gated FET system could detect SARS-CoV-2 based on changes in channel surface potential and the corresponding effects on the electrical response.
We measured the transfer curves of the graphene-based FET after each modification process (Figure 3D). After PBASE functionalization, an obvious positive shift was observed due to the p-doping effect of the pyrene group. However, the transfer curve was shifted negatively, suggesting that the positive charge of the antibody exerted an n-doping effect on graphene after the antibody was immobilized.
Figure 3B shows the output curves of the COVID-19 FET sensor as a function of gate voltage (VG) over a range from 0 to −1.5 V in steps of −0.3 V. IDS negatively increased as VG negatively increased, corresponding to the predicted behavior of a p-type semiconductor.(26,27)
Moreover, the linear I–V curves exhibited highly stable ohmic contact, indicating that the COVID-19 FET sensor provided a reliable electrical signal for detection of the target analytes (SARS-CoV-2 antigen protein, cultured SARS-CoV-2 virus, or SARS-CoV-2 virus from clinical samples).
Real-Time Detection of SARS-CoV-2 Antigen Protein
To investigate the performance of the COVID-19 FET sensor, we evaluated the dynamic response of the sensor to spike protein (Figure 4A). First, we measured the sensor’s LOD for spike protein. The sensor responded to 1 fg/mL of SARS-CoV-2 spike protein in PBS (Figure 4B); that is, the LOD of the FET sensor was substantially lower than that of the ELISA platform (Figure S2).
However, the pristine graphene-based device without SARS-CoV-2 spike protein conjugation did not show any remarkable signal change after the introduction of various sample concentrations (gray line in Figure 4D).
The control experiment indicates that the SARS-CoV-2 spike protein is essential for specific binding with the SARS-CoV-2 antigen.
In addition, the COVID-19 FET sensor exhibited no response to MERS-CoV spike proteins (Figure 4D), indicating that the COVID-19 FET sensor was both highly sensitive and specific for the SARS-CoV-2 spike antigen protein.
Figure 4

Figure 4. Detection of SARS-CoV-2 antigen protein. (A) Schematic diagram for the COVID-19 FET sensor for detection of SARS-CoV-2 spike protein. (B) Real-time response of COVID-19 FET toward SARS-CoV-2 antigen protein in PBS and (C) related dose-dependent response curve (VDS = 0.01 V). Graphene-based FET without SARS-CoV-2 antibody is presented as negative control. (D) Selective response of COVID-19 FET sensor toward target SARS-CoV-2 antigen protein and MERS-CoV protein. (E) Real-time response of COVID-19 FET toward SARS-CoV-2 antigen protein in UTM and (F) related dose-dependent response curve.
In the clinic, diagnosis of COVID-19 is performed using nasopharyngeal swabs suspended in universal transport medium (UTM). The UTM contains various reagents that may affect performance of the FET sensor, such as Hank’s balanced salts and BSA. Therefore, we assessed the response of the FET sensor to antigens in UTM.
To determine whether the FET sensor could be used in the field, we measured the response of the FET sensor to SARS-CoV-2 spike proteins in 0.01× UTM. The results revealed that the FET sensor could successfully detect SARS-CoV-2 spike antigen proteins starting from a concentration of 100 fg/mL (Figure 4E).
This indicates that the COVID-19 FET sensor can detect antigens in clinical samples without any preparation or preprocessing. To further investigate the normalized sensitivity of the COVID-19 FET sensor, the changes in sensitivity as a function of SARS-CoV-2 antigen protein concentration were characterized by fitting each data point, as shown in Figure 4C,F.
Real-Time Detection of Cultured SARS-CoV-2 Virus
Next, we investigated whether the COVID-19 FET sensor could detect SARS-CoV-2 virus (Figure 5A). To this end, we propagated SARS-CoV-2 in cultured cells and inactivated viral infectivity by heating. Upon application of cultured SARS-CoV-2, the COVID-19 FET sensor responded to concentrations as low as 1.6 × 101 pfu/mL (Figure 5B), and the normalized response curve was linear from 1.6 × 101 to 1.6 × 104 pfu/mL (Figure 5C). This result suggests that the COVID-19 FET sensor has the potential to be used for COVID-19 diagnosis.
Figure 5

Figure 5. Detection of cultured SARS-CoV-2 virus. (A) Schematic diagram for the COVID-19 FET sensor for detection of SARS-CoV-2 cultured virus. (B) Real-time response of COVID-19 FET toward SARS-CoV-2 cultured virus and (C) related dose-dependent response curve.
Detection of SARS-CoV-2 Virus from Clinical Samples
Finally, we tested the detection performance of the COVID-19 FET sensor using clinical samples (Figure 6A). To this end, we collected nasopharyngeal swab specimens from COVID-19 patients and normal subjects and stored them in UTM. Prior to addition of patient samples to the device, we evaluated nasopharyngeal swab samples from normal subjects to determine the basal signal.
The COVID-19 FET sensor clearly discriminated between patient and normal samples (Figure 6B,C). In addition, the FET sensor responded to patient samples diluted as much as 1:1 × 105 (242 copies/mL) (Figure 6D), and the normalized response curve of the FET sensor was linear (Figure 6E).
Given that UTM includes various reagents and generates noise signals, we consider the LOD of the COVID-19 FET sensor to be low enough for practical use Table S2. Nevertheless, development of novel materials of the FET sensor for UTM should be necessary for more accurate detection by reducing the noise signals. For reference, the detection limit of current molecular diagnostic tests of COVID-19 is ∼50–100 copies.(28)
Taken together, our findings show that our COVID-19 FET sensor successfully detected SARS-CoV-2 virus from clinical samples without any preprocessing and with a large dynamic range.
Figure 6

Figure 6. Detection of SARS-CoV-2 virus from clinical samples. (A) Schematic diagram for the COVID-19 FET sensor for detection of SARS-CoV-2 virus from COVID-19 patients. (B,C) Comparison of response signal between normal samples and patient ones. (D) Real-time response of COVID-19 FET toward SARS-CoV-2 clinical sample and (C) related dose-dependent response curve.
Source:
American Chemical Society



{kind=link}