











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Researchers from the Hubrecht Institute in Utrecht, Erasmus MC University Medical Center Rotterdam, and Maastricht University in the Netherlands have found that the coronavirus SARS-CoV-2, which causes COVID-19, can infect cells of the intestine and multiply there.
Using state-of-the-art cell culture models of the human intestine, the researchers have successfully propagated the virus in vitro, and monitored the response of the cells to the virus, providing a new cell culture model for the study of COVID-19.
These findings could explain the observation that approximately one third of COVID-19 patients experience gastrointestinal symptoms such as diarrhea, and the fact that the virus often can be detected in stool samples. The results of this study were published in the scientific journal Science on the 1st of May 2020.
Patients with COVID-19 show a variety of symptoms associated with respiratory organs – such as coughing, sneezing, shortness of breath, and fever – and the disease is transmitted via tiny droplets that are spread mainly through coughing and sneezing.
One third of the patients however also have gastrointestinal symptoms, such as nausea and diarrhea. In addition, the virus can be detected in human stool long after the respiratory symptoms have been resolved. This suggests that the virus can also spread via so-called “fecal-oral transmission.”
Though the respiratory and gastrointestinal organs may seem very different, there are some key similarities. A particularly interesting similarity is the presence of the ACE2 receptor, the receptor through which the COVID-19 causing SARS-CoV-2 virus can enter the cells.
The inside of the intestine is loaded with ACE2 receptors. However, until now it was unknown whether intestinal cells could actually get infected and produce virus particles.
Intestinal organoids
Researchers from the Hubrecht Institute, Erasmus MC and Maastricht University set out to determine whether the SARS-CoV-2 virus can directly infect the cells of the intestine, and if so, whether it can replicate there as well.
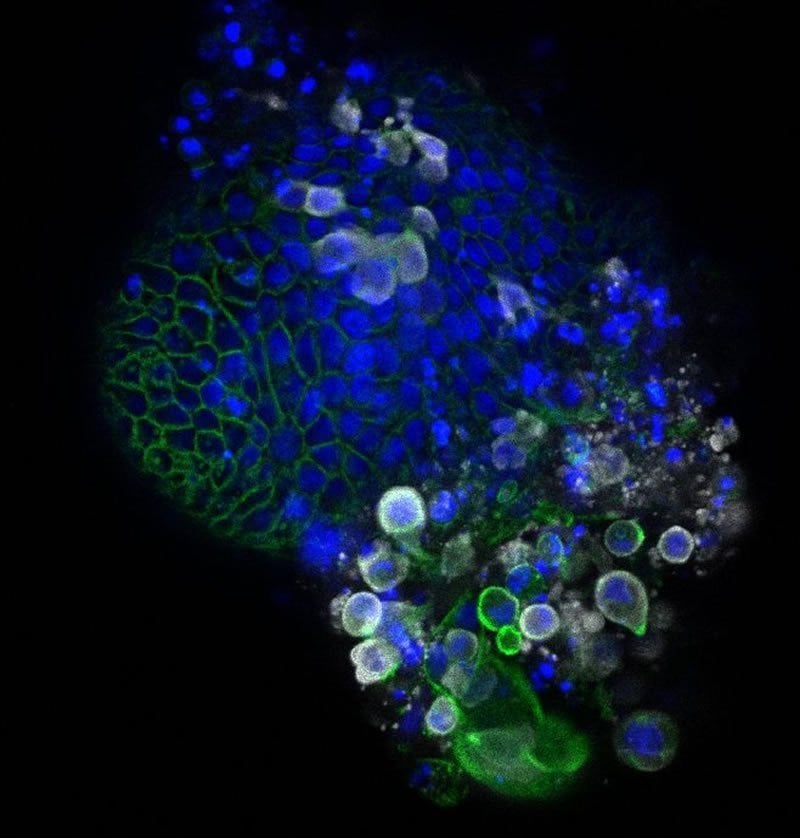
They used human intestinal organoids: tiny versions of the human intestine that can be grown in the lab. Hans Clevers (Hubrecht Institute) states: “These organoids contain the cells of the human intestinal lining, making them a compelling model to investigate infection by SARS-CoV-2.”
Infection of intestinal cells
When the researchers added the virus to the organoids, they were rapidly infected. The virus enters a subset of the cells in the intestinal organoids, and the number of cells that are infected increases over time.
Using electron microscopy, an advanced way to visualize different components of the cell in great detail, the researchers found virus particles inside and outside the cells of the organoids. Peter Peters (Maastricht University) says: “Due to the lockdown, we all studied virtual slides of the infected organoids remotely from home.”
The researchers investigated the response of the intestinal cells to the virus with RNA sequencing, a method to study which genes are active in the cells. This revealed that so-called interferon stimulated genes are activated. These genes are known to combat viral infection. Future work will focus on these genes more carefully, and on how they could be used to develop new treatments.
The researchers also cultured the organoids in different conditions that result in cells with higher and lower levels of the ACE2 receptor, through which SARS-CoV-2 can enter the cells. To their surprise, they found that the virus infected cells with both high and low levels of the ACE2 receptor. Ultimately, these studies may lead to new ways to block the entry of the virus into our cells.
Implications
Bart Haagmans (Erasmus MC) concludes: “The observations made in this study provide definite proof that SARS-CoV-2 can multiply in cells of the gastrointestinal tract.
However, we don’t yet know whether SARS-CoV-2, present in the intestines of COVID-19 patients, plays a significant role in transmission. Our findings indicate that we should look into this possibility more closely.”
The current study is in line with other recent studies that identified gastrointestinal symptoms in a large fraction of COVID-19 patients and virus in the stool of patients free of respiratory symptoms.
Special attention may be needed for those patients with gastrointestinal symptoms. More extensive testing using not only nose and throat swabs, but also rectal swabs or stool samples may thus be needed.
In the meantime, the researchers are continuing their collaboration to learn more about COVID-19. They are studying the differences between infections in the lung and the intestine by comparing lung and intestinal organoids infected with SARS-CoV-2.
This study was a collaboration between the Hubrecht Institute in Utrecht, the Erasmus MC University Medical Center Rotterdam, Maastricht University, the UMC Utrecht and Single Cell Discoveries in the Netherlands.
The microscopy data are publicly available via the Image Data Resource (idr0083, https://idr.openmicroscopy.org – with help from the University of Dundee and the European Bioinformatics Institute) and the genomic data are publicly available via the Gene Expression Omnibus (GSE149312, https://www.ncbi.nlm.nih.gov/geo), to ensure efficient sharing of data related to COVID-19 between researchers all across the world.
Highlights
- Amongst the gastrointestinal manifestations experienced by COVID-19 patients, those commonly noted are diarrhea, anorexia, nausea, vomiting, and abdominal pain – which can be present even in the absence of respiratory symptoms.
- Hepatic injury is evident in some patients, the degree of which at times can mirror severity of disease; pancreatic injury has been noted as well.
- SARS-CoV-2 RNA has been found in fecal samples even after viral RNA in respiratory samples clears, raising concern for gastrointestinal viral replication and potential for fecal-oral transmission.
- While no definitive treatment for COVID-19 exists, mainstay remains supportive including oxygen and mechanical ventilation; at this time, gastrointestinal manifestations are largely managed symptomatically as well.
- The potential for fecal-oral spread of infectious virions may warrant additional precautions and patient education about proper hand hygiene, social distancing, and understanding the risk for close contacts and re-infection.
GASTROINTESTINAL SYMPTOMOLOGY
The most characterized symptoms of COVID-19 include fever, cough, fatigue, dyspnea, sore throat, headache, and myalgias or arthralgias 6.
Approximately 80% of patients demonstrate mild symptoms; 20% have severe disease; about 5% of patients exhibit critical disease symptoms such as respiratory arrest, septic shock, or multiple organ failure 6.
The median incubation period for COVID-19 is five days 10. As SARS-CoV-2 has widely been studied as a respiratory tract pathogen, its extent of involvement in the gastrointestinal system is currently under investigation.
A multicenter and cross-sectional study demonstrated that approximately 50% of patients experienced symptoms such as diarrhea, nausea, vomiting, abdominal pain. Similar studies in China supported the presence of these symptoms among COVID-19 patients (Table 1) 7,11,16,17.
Furthermore, the time from onset of gastrointestinal symptoms to hospital presentation is delayed compared to respiratory symptoms (9.0 vs. 7.3 days) 11.
Table 1. Percentage of 2019 coronavirus disease COVID-19 patients exhibiting gastrointestinal manifestations in various studies completed from China.
| Incidence of Gastrointestinal (GI) Manifestations exhibited in COVID-19 Patients | |||
|---|---|---|---|
| Study | Number of Patients N | GI symptoms N (%) | No GI symptoms N (%) |
| Pan L, et al. 11 | 203 | 103 (50.7%) | 100 (49.3%) |
| Jin X., et al. 7 | 651 | 74 (11.3%) | 577 (88%) |
| Fang D, et al. 16 | 201 | 159 (79.1%) | 42 (20.8%) |
| Zhang JJ, et al 17 | 139 | 55 (39.6%) | 84 (60.4%) |
COVID-19-coronavirus disease 2019, N- Number.
Additional studies have characterized similar results among COVID-19 patients. One study examining 651 patients in the Zhejiang Province of China showed that 11.4% presented with at least one gastrointestinal symptom consisting of nausea, vomiting, or diarrhea; the average age of these patients was 46.1 years, with 10.8% having pre-existing liver disease 7. Of COVID-19 patients with gastrointestinal symptoms, a subset also experienced significantly higher rates of fever, fatigue, shortness of breath, and headache 7.
The first COVID-19 patient in the United States presented with nausea, vomiting, cough, with additional gastrointestinal symptoms of loose bowel movements and abdominal pain during his hospitalization. He eventually tested positive for SARS-CoV-2 RNA in his stool and respiratory specimens upon rRT-PCR testing 12,13. Additionally, the first case of hematochezia as a possible initial presenting symptom of COVID-19 was reported. Although the patient’s stool specimens were not tested for viral RNA, this case highlights a rare gastrointestinal manifestation of the COVID-19 14.
A recent paper by Tian et al. reviewing studies to date on gastrointestinal manifestations and COVID-19 infection investigated the incidence of specific symptoms in both children and adults. Diarrhea was the most common symptom in both children and adults, lasting approximately four days. There was a higher proportion of children who exhibited vomiting compared to adults. Furthermore, other symptoms noted were anorexia (39.9%-50.2%), vomiting (3.6%-66.7%), nausea (1%-29.4%), abdominal pain (2.2%-6.0%), and gastrointestinal bleeding (4%-13.7%) 12. Additional studies have characterized similar results amongst COVID-19 patients (see Table 2) 7,11,[16], [17], [18], [19], [20], [21], [22], [23], [24]. It is crucial to note that adult and children patients with COVID-19 may present with digestive symptoms in the absence of respiratory symptomatology.
Table 2. Incidence of specific gastrointestinal symptoms exhibited by COVID-19 patients in studies completed from China.
| Incidence of Type of Gastrointestinal Symptoms exhibited in COVID-19 Patients | ||||||
|---|---|---|---|---|---|---|
| Study | Number of Patients N | Anorexia N (%) | Nausea N (%) | Vomiting N (%) | Diarrhea N (%) | Abdominal Pain N (%) |
| Pan L, et al. 11 | 103 | 81 (78.6%) | NA | 4 (3.9%) | 35 (34%) | 2 (2%) |
| Jin X., et al. 7 | 74 | NA | 13 (17.5%) | 14 (18.6%) | 56 (75%) | NA |
| Fang D, et al. 16 | 201 | NA | 59 (29.4%) | 32 (16 %) | 44 (22%) | 12 (6%) |
| Guan W, et al. 18 | 1095 | NA | 55 (5%) | 55 (5%) | 42 (3.8%) | NA |
| Zhang JJ, et al. 17 | 139 | 17 (12.2%) | 24 (17.3%) | 7 (5%) | 18 (13%) | 8 (13%) |
| Wang D, et al. 19 | 138 | 55 (40%) | 14 (10%) | 5 (3.6%) | 14 (10%) | 3 (2.2%) |
| Shi H, et al. 20 | 81 | 1 (1%) | NA | 4 (5%) | 3 (4%) | NA |
| Zhou F, et al. 21 | 191 | NA | 7 (4%) | 7 (4%) | 9 (5%) | NA |
| Mo P, et al. 22 | 155 | NA | 3 (3.7%) | 3 (4%) | 7 (4.5%) | 3 (2%) |
| Chen N, et al. 23 | 99 | NA | 1 (1%) | 1 (1%) | 2 (2%) | NA |
| Yang X. et al. 24 | 52 | NA | NA | 2 (4%) | NA | NA |
COVID-19-coronavirus disease 2019, NA- not applicable.
The gastrointestinal manifestations secondary to SARS-CoV-2 infection can occur through different mechanisms. Firstly, ACE2 receptors, by which the virus uses to gain cellular entry, is expressed in both the respiratory tract and gastrointestinal tract epithelium, creating the potential for viral replication in the gastrointestinal tract.
Secondly, there could be a direct injury of the gastrointestinal system due to an inflammatory response 11. Absorptive enterocytes may be infected and destroyed by SARS-CoV-2, potentially leading to malabsorption, unbalanced intestinal secretion, and an activated enteric nervous system resulting in symptoms like diarrhea 15.
HEPATOBILIARY SYSTEM
An increasing number of COVID-19 patients have been noted to experience hepatic injury, ranging on a spectrum of mild to severe damage 25. Hepatic injury has been evident in specific laboratory abnormalities in these patients – the pathophysiology behind SARS-CoV-2 infection may suggest the injury is due to the disease process.
According to the American College of Gastroenterology (ACG), abnormal liver enzymes are observed in 20-30% of persons with confirmed COVID-19 infection 26. In a study examining 148 confirmed SARS-CoV-2 infected patients in China, 50.7% of patients were found to have abnormal liver functions at admission 25.
Additional studies have demonstrated similar results with abnormalities in liver enzymes and total bilirubin (Table 3) 11,16,18,[20], [21], [22], [23],30,31. Patients with elevated liver function tests were more likely to have a moderate-high degree fever, and these elevations were significantly more prevalent in male patients (68.67% vs. 38.36%). Additionally, in these patients, the CD4+ and CD8 + T cells were substantially lower as compared to those with normal liver function tests 25.
Per the ACG, drops in leukocyte counts are observed in COVID-19 infection, and an elevated white blood cell count is considered a poor prognostic sign 26.
Studies have found that most liver injuries are mild and transient, but severe liver damage can also occur 27. A higher magnitude of liver injury was noted in individuals with severe COVID-19, in which cases hepatoprotective drugs can be administered 5,27.
Table 3. Percentage of COVID-19 patients exhibiting hepatobiliary laboratory abnormalities including AST, ALT, and total bilirubin in studies completed from China.
| Hepatobiliary Laboratory Abnormalities seen in COVID-19 Patients | ||||
|---|---|---|---|---|
| Study | Number of Patients (N) | AST N (%) | ALT N (%) | Total Bilirubin N (%) |
| Pan L, et al. 11 | 204 | 22 (11%) | 27 (13%) | NA |
| Fang D, et al. 16 | 304 | 24 (8%) | 19 (6%) | 6 (2%) |
| Guan W, et al. 18 | 741 | 168 (22%) | 158 (21%) | 76 (10%) |
| Chen N, et al. 23 | 99 | 35 (35%) | 28 (28%) | 18 (18%) |
| Xu X, et al. 30 | 62 | 10 (16%) | 26 (20-32)+ | NA |
| Huang C et al. 31 | 41 | 15 (37%) | 32 (21-50)+ | 11.7 (9.5-13.9)++ |
| Zhou F, et al. 21 | 189 | NA | 59 (31%) | NA |
| Mo P, et al. 22 | 155 | 32 (24-48)++ | 23 (16-38) | NA |
| Shi H, et al. 20 | 81 | 43 (53%) | NA | NA |
COVID-19-coronavirus disease 2019, AST-Aspartate aminotransferase, ALT- Alanine aminotransferase, ++ median in mmol/L, + median in U/L, N- number.
The definitive mechanism by which liver injury occurs in COVID-19 patients is unclear.
There are multiple theories of the pathophysiology of the viral infection that could explain this phenomenon:
(1) ACE2-mediated direct viral infection of hepatocytes,
(2) Critically-ill status and immune-mediated injury, or
(3) Drug hepatotoxicity 5.
As it has been established that the receptor ACE2 by which SARS-CoV-2 uses to gain cellular entry is highly expressed in gastrointestinal epithelial cells, the virus could have the ability to infect cholangiocytes via this receptor to dysregulate liver function 1,5. Liver injury may also occur as ACE2 expression in liver tissue is upregulated as a compensatory proliferation of hepatocytes derived from bile duct epithelial cells 11.
While SARS-CoV-2 may cause dysregulation of hepatic function by binding directly to ACE2-receptor cholangiocytes, histological examination of a liver biopsy obtained from a deceased COVID-19 patient showed no viral inclusions, but rather microvesicular steatosis and mild lobular activity 27,5.
Furthermore, in critically-ill COVID-19 patients, hepatocellular injury or even liver failure may be secondary to hypotension and immune-mediated inflammation, such as cytokine storm or pneumonia-associated hypoxia 27.
Lastly, drug-induced hepatotoxicity may play a role in the elevation of liver enzymes, including medications such as remdesivir (an RNA polymerase inhibitor) and hydroxychloroquine 5,28.
Patients with pre-existing liver disease are an important group of individuals that require additional attention. In a study of 1099 COVID-19 patients, 23 patients had hepatitis B infection – severe cases of COVID-19 were more likely to have hepatitis B infection than non-severe cases (2.4% vs. 0.6%) 29.
Furthermore, in patients with COVID-19 with autoimmune hepatitis, the role of glucocorticoids in disease management is currently unclear 27. In the setting of primary biliary cholangitis (PBC), COVID-19 may aggravate cholestasis.
Therefore, alkaline phosphatase and gamma-glutamyl transfersase (GGT) levels should carefully be monitored. Given their immunocompromised state, patients with hepatic cirrhosis or cancer may be more susceptible to COVID-19 27.
PANCREAS
In a recent study by Wang et al. examining 52 patients with COVID-19 pneumonia, 17% of patients experienced pancreatic injury defined by any abnormality in amylase or lipase 32. They did not exhibit clinical symptoms of severe pancreatitis, however.
The ACE2 receptor is also highly expressed in pancreatic islet cells, therefore SARS-CoV-2 infection can theoretically cause islet damage resulting in acute diabetes.
Of the nine patients with pancreatic injury, six had abnormal blood glucose levels.
Mechanisms by which pancreatic injury could occur include the direct cytopathic effects of SARS-CoV-2, or indirect systemic inflammatory and immune-mediated cellular responses, resulting in organ damage or secondary enzyme abnormalities 32,33.
Antipyretics, which most of the patients in this study took prior to admission, could also cause drug-related pancreatic injury 32. Further research is necessary to definitively determine the effect of SARS-CoV-2 on pancreatic function and regulation.
ROUTES OF TRANSMISSION
SARS-CoV-2 can be found in the respiratory secretions of patients 1-2 days before onset of clinical symptoms and for up to two weeks after symptoms subside. The virus has previously been found in whole blood, serum, urine, and fecal samples 6.
A study by Cai et al. demonstrated that some pediatric patients were noted to have a high frequency of SARS-CoV-2 RNA detection in feces. It also confirmed prolonged viral RNA shedding in feces for at least two weeks and upwards of more than a month, raising suspicion that the gastrointestinal tract acts as another site of viral replication 8.
A study conducted by Xiao et al. demonstrated results favoring gastrointestinal viral replication with potential fecal-oral route of transmission 34. Amongst 73 hospitalized COVID-19 patients in China, ranging from 10 months to 78 years old, 53.42% tested positive for SARS-CoV-2 RNA in the stool.
Positive stool results ranged from 1-12 days, and 23.29% continued to have positive stool results after having negative respiratory samples 34. Upon endoscopy and biopsy, the study also found that SARS-CoV-2 RNA was detected with positive staining of the viral nucleocapsid protein in gastric, duodenal, and rectal epithelium. These findings further support the evidence of replication of infectious virions occurring within the gastrointestinal tract 34.
Accordingly, fecal-oral transmission must be taken into consideration. Of great significance is the fact that viral RNA in feces can remain even after viral RNA in the respiratory tract clears – therefore providing a potential source of spread. Considerations for testing of viral RNA in feces by rRT-PCR can be taken to monitor for adequate source and infection control 34.
DIAGNOSTIC TESTING & LABORATORY ABNORMALITIES
Currently, nasopharyngeal samples are used for the testing of suspected COVID-19; however, with the occurrence of gastrointestinal manifestations, the use of fecal testing may be beneficial as well. Additionally, recognizing that gastrointestinal symptoms could be the initial presentation of COVID-19, prompt and timely diagnostic testing is necessary for early detection.
The use of fecal nucleic acid tests to diagnose COVID-19 have recently increased. A study by Zhang et al. demonstrated that fecal specimens were as accurate as pharyngeal specimens 35. It was also found that a positive stool test did not correlate to the severity of the lung infection. Advantages of stool testing include the possibility that it may reduce infections in medical staff compared to oropharyngeal swab specimens 35.
The definitive role of endoscopy and colonoscopy in the diagnosis of COVID-19 remains largely unclear at this point. According to the Spanish Society of Digestive Pathology and the Spanish Association of Gastroenterology, upper endoscopies, ERCP, and placement of peg tube procedures have a high risk of infection transmission; colonoscopies and lower echoendoscopies are intermediate risk 36.
The American Society of Gastrointestinal Endoscopy currently has similar recommendations as of March 13, 2020: endoscopy is a high-risk procedure because of the potential transmission of the virus via a fecal-oral route and the risk of transmitting COVID-19 during its incubation period in asymptomatic patients 37.
Aggressive Personal Protective Equipment (PPE) should be utilized during these procedures for adequate infection control.
Apart from diagnostic tests, certain laboratory abnormalities have been noted in patients with COVID-19. In a study of 1099 confirmed COVID-19 cases from mainland China, patients exhibited lymphocytopenia (83.2%), thrombocytopenia (36.2%), and leukopenia (33.7%) on admission 18.
Based on a study involving 140 COVID-19 patients, those with severe disease were noted to have an elevated D dimer (2.0-fold), C-reactive protein (1.7-fold), procalcitonin (2.0-fold), lactate dehydrogenase (2.1-fold), decreased lymphocyte count, and leukopenia as compared to individuals with milder disease 10.
Recognizing that the earliest presenting symptoms of COVID-19 could be gastrointestinal rather than respiratory may improve early detection with various available diagnostic tests. Extending beyond the usage of nasopharyngeal sample testing alone to include routine fecal RNA testing can be beneficial. Furthermore, identifying common laboratory abnormalities that these patients exhibit can also help in assessing the severity of the infection.
REFERENCES
[1] Y.R. Guo, Q.D. Cao, Z.S. Hong, Y.Y. Tan, S.D. Chen, H.J. Jin, K.S. Tan, D.Y. Wang, Y. Yan
The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status
Military Medical Research, 7 (1) (2020), p. 11, 10.1186/s40779-020-00240-0
[2] World Health Organization – Naming the coronavirus disease (COVID-19) and the virus that causes it
World Health Organization, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (2020)
[3] World Health Organization – Coronavirus disease 2019 (Covid-19) Situation Report – 88 (2020)
[4] S. Singh, et al. – Coronavirus: A threat to Global Public Health Indian J Comm Health., 32 (1) (2020), pp. 21-27
[5] S.H. Wong, R.N. Lui, J.J. Sung – Covid-19 and the Digestive System Journal of Gastroenterology and Hepatology (2020), 10.1111/jgh.15047
[6] K. Buruk, T. Ozlu – New Coronavirus: SARS-COV-2 – Mucosa (2020), pp. 1-4 doi: 10.33204/mucosa.706906
[7] X. Jin, J. Lian, J. Hu, et al. – Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms – Gut (2020), 10.1136/gutjnl-2020-320926 Published Online First: 24 March
[8] Jiehao Cai, Jing Xu, Daojiong Lin, zhi Yang, Lei Xu, Zhenghai Qu, et al., A Case Series of children with 2019 novel coronavirus infection: clinical and epidemiological features, Clinical Infectious Diseases,, ciaa198, https://doi.org/10.1093/cid/ciaa198.
[9] J. Chen, et al. – Clinical Features of Stool SARS-CoV-2 RNA Positive in 137 COVID-19 Patients in Taizhou, China https://ssrn.com/abstract=3551383 (2020), 10.2139/ssrn.3551383 Available at SSRN
[10] S.A. Lauer, K.H. Grantz, Q. Bi, et al. – The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application Ann Intern Med. (2020), 10.7326/M20-0504 [Epub ahead of print 10 March 2020]
[11] L. Pan, et al. – Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, cross-sectional, multicenter study – Preprint at https://journals.lww.com/ajg/Documents/COVID_Digestive_Symptoms_AJG_Preproof.pdf (2020)
[12] Y. Tian, L. Rong, W. Nian, Y. He – Review article: gastrointestinal features in COVID-19 and the possibility of faecal transmission – Alimentary Pharmacology & Therapeutics (2020), 10.1111/apt.15731
[13] M.L. Holshue, C. Debolt, S. Lindquist, K.H. Lofy, J. Wiesman, H. Bruce, et al. – First Case of 2019 Novel Coronavirus in the United States – New England Journal of Medicine, 382 (10) (2020), pp. 929-936, 10.1056/nejmoa2001191
[14] L. Guotao, Z. Xingpeng, D. Zhihui, W. Huirui – SARS-CoV-2 infection presenting with hematochezia Médecine Et Maladies Infectieuses (2020), 10.1016/j.medmal.2020.03.005
[15] H. Zhang, et al. – The digestive system is a potential route of 2019-nCov infection: a bioinformatics analysis based on single-cell transcriptomes – Preprint at https://www.biorxiv.org/content/10.1101/2020.01.30.927806v1 (2020)
[16] D. Fang, J.D. Ma, J.L. Guan, et al. – Digestive manifestations in hospitalized patients with COVID-19: A single-center descriptive study Chin J Dig, 40 (3) (2020), 10.3760/cma J.D.issn.0254-1432.2020.0005
[17] J.-J. Zhang, X. Dong, Y.-Y. Cao, Y.-D. Yuan, Y.-B. Yang, Y.-Q. Yan, et al. – Clinical characteristics of 140 patients infected with SARS‐CoV‐2 in Wuhan, China Allergy (2020), 10.1111/all.14238
[18] W.-J. Guan, Z.-Y. Ni, Y. Hu, W.-H. Liang, C.-Q. Ou, J.-X. He, et al. – Clinical Characteristics of Coronavirus Disease 2019 in China – New England Journal of Medicine (2020), 10.1056/nejmoa2002032
[19] D. Wang, B. Hu, C. Hu, et al. – Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China -JAMA, 323 (11) (2020), pp. 1061-1069, 10.1001/jama.2020.1585
[20] H. Shi, X. Han, N. Jiang, Y. Cao, O. Alwalid, J. Gu, et al. – Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study – The Lancet Infectious Diseases, 20 (4) (2020), pp. 425-434, 10.1016/s1473-3099(20)30086-4
[21] F. Zhou, T. Yu, R. Du, G. Fan, Y. Liu, Z. Liu, et al. – Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study – The Lancet, 395 (10229) (2020), pp. 1054-1062, 10.1016/s0140-6736(20)30566-3
[22] P. Mo, Y. Xing, Y. Xiao, L. Deng, Q. Zhao, H. Wang, et al. – Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China – Clinical Infectious Diseases (2020), 10.1093/cid/ciaa270
[23] N. Chen, M. Zhou, X. Dong, J. Qu, F. Gong, Y. Han, et al. – Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study – The Lancet, 395 (10223) (2020), pp. 507-513, 10.1016/s0140-6736(20)30211-7
[24] X. Yang, Y. Yu, J. Xu, H. Shu, J. Xia, H. Liu, et al. – Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study – The Lancet Respiratory Medicine (2020), 10.1016/s2213-2600(20)30079-5
[25] Z. Fan, et al. – Clinical Features of COVID-19 Related Liver Damage – Preprint at https://www.medrxiv.org/content/10.1101/2020.02.26.20026971v2 (2020)
[26] ACG News Team – Joint GI Society Message on COVID-19 -American College of Gastroenterology, https://gi.org/2020/03/15/joint-gi-society-message-on-covid-19/ (2020)
[27] C. Zhang, L. Shi, F.-S. Wang – Liver injury in COVID-19: management and challenges – The Lancet Gastroenterology & Hepatology, 5 (5) (2020), pp. 428-430, 10.1016/s2468-1253(20)30057-1
[28] M. Cascella, M. Rajnik, A. Cuomo, et al. – Features, Evaluation and Treatment Coronavirus (COVID-19) StatPearls [Internet], StatPearls Publishing, Treasure Island (FL) (2020)- https://www.ncbi.nlm.nih.gov/books/NBK554776/
[29] R. Mao, J. Liang, J. Shen, S. Ghosh, L.-R. Zhu, H. Yang, et al. – Implications of COVID-19 for patients with pre-existing digestive diseases – The Lancet Gastroenterology & Hepatology, 5 (5) (2020), pp. 426-428, 10.1016/s2468-1253(20)30076-5 –
[30] Xu, X.-W., Wu, X.-X., Jiang, X.-G., Xu, K.-J., Ying, L.-J., Ma, C.-L., et al. (2020). Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. Bmj, m606. doi: 10.1136/bmj.m606.
[31] C. Huang, Y. Wang, X. Li, L. Ren, J. Zhao, Y. Hu, et al. – Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China – The Lancet, 395 (10223) (2020), pp. 497-506, 10.1016/s0140-6736(20)30183-5 –
[32] F. Wang, H. Wang, J. Fan, Y. Zhang, H. Wang, Q. Zhao – Pancreatic injury patterns in patients with COVID-19 pneumonia – Gastroenterology (2020), 10.1053/j.gastro.2020.03.055
[33] F. Liu, et al. – Highly ACE2 Expression in Pancreas May Cause Pancreas Damage After SARS-CoV-2 Infection
Preprint at https://www.medrxiv.org/content/10.1101/2020.02.28.20029181v1.full.pdf (2020)
[34] F. Xiao, M. Tang, X. Zheng, Y. Liu, X. Li, H. Shan – Evidence for Gastrointestinal Infection of SARS-CoV-2 – Gastroenterology (2020), 10.1053/j.gastro.2020.02.055
[35] J. Zhang, S. Wang, Y. Xue – Fecal specimen diagnosis 2019 novel coronavirus–infected pneumonia – Journal of Medical Virology (2020), 10.1002/jmv.25742
[36] E.P.-C. Martínez – Recommendations by the SEPD and AEG, both in general and on the operation of gastrointestinal endoscopy and gastroenterology units, concerning the current SARS-CoV-2 pandemic (March, 18) – Revista Española De Enfermedades Digestivas (2020), 10.17235/reed.2020.7052/2020
[37] American Society for Gastrointestinal Endoscopy – ASGE Releases Recommendations for Endoscopy Units in the Era of COVID-19 – American Society for Gastrointestinal Endoscopy, https://www.asge.org/docs/default-source/default-document-library/press-release_impact-of-covid-19-on-endoscopy.pdf (2020)
Source:
Hubrecht Institute



{kind=link}