











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Clinical observations of COVID-19 patients, who went on to have a stroke, suggest coronavirus may cause clots within blood vessels (arteries) in the brain, finds a team of neurologists from UCL and UCLH (the National Hospital for Neurology and Neurosurgery), London.
The findings suggest early testing for D-dimer, a protein fragment in the blood associated with increased blood clotting (thrombosis) in COVID-19 patients, could enable clinicians to prescribe specific treatments, including anticoagulants (“blood thinners”), at a much earlier stage, which might reduce the number of people subsequently having further strokes or blood clots elsewhere in the body.
In a research article published in the Journal of Neurology, Neurosurgery, and Psychiatry, corresponding author Professor David Werring (UCL Queen Square Institute of Neurology) and colleagues report on six consecutive patients assessed between April 1 to 16 2020 at the National Hospital for Neurology and Neurosurgery, London, (part of University College London Hospitals NHS Foundation Trust) with acute ischaemic stroke (due to blockage of a large brain artery) and proven COVID-19.
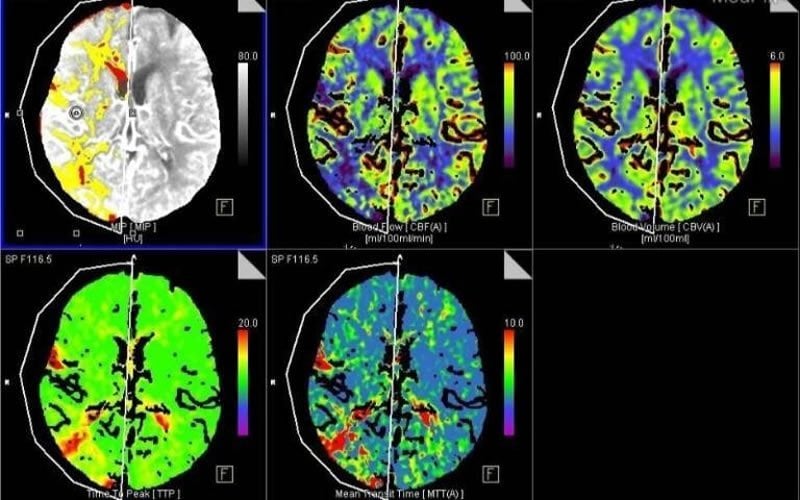
Acute ischaemic stroke is caused by the sudden loss of blood circulation to an area of the brain, resulting in loss of neurological function.
In summary, all six patients (aged between 53 and 85) had large vessel occlusion (large arterial blockage), with markedly elevated blood levels of D-Dimer indicating the presence of abnormally high “fibrin degradation products” – components in the blood produced when clots break down.
This report is based on a small number of patients, and doesn’t confirm a direct link between COVID-19 and stroke (as other factors that are linked to stroke were present in most patients).
However, the findings support other recent evidence: the exaggerated inflammatory immune response known to occur in COVID-19 patients stimulates abnormal blood coagulation, including raised D-dimer and the production of antiphospholipid antibodies—which are usually caused by a disorder in the immune system.
Furthermore, five of the six ischaemic strokes occurred 8-24 days after COVID-19 symptom onset (cough, headache, and chills), and in one patient during the pre-symptomatic phase, suggesting that COVID-19 associated ischaemic stroke is usually delayed, but can occur both early and later in the course of the disease.
Discussing the findings, Professor Werring, Professor of Clinical Neurology at UCL and a Consultant Neurologist at the National Hospital for Neurology and Neurosurgery, Queen Square, London, said: “We now know that COVID-19 is not just a disease of the lungs. Our findings suggest that blockages of large brain arteries in COVID-19 patients are associated with highly abnormal blood clotting.
“Early use of anticoagulant drugs might be helpful, but this needs to be balanced against their brain bleeding risk, especially soon after an ischaemic stroke.
“Clinical studies (ideally controlled trials) are needed to find out the best treatment to reduce the disability caused by ischaemic stroke in people with COVID-19. Our findings emphasise that even during the lockdown people with suspected stroke must attend hospital immediately to ensure they get the best treatment.”
As of April 3rd, 2020, global cases had passed 1 million, with more than 55,000 deaths worldwide. The United States continues to have the most confirmed cases worldwide, with over 265,000 cases and 6,700 deaths (3).
The continuous rise in cases of COVID-19 with the associated demand for medical attention has caused a major burden on health care systems, with increases in health care utilization beyond current hospital capacities.
This extends to increase bed occupancy, shortage of intensive care beds, and extensive need for expansion of workforce and allocation of limited resources.
Vascular neurologists need to stay vigilant as majority of stroke patients are older and have underlying medical conditions associated not only with risk for ischemic stroke, but poor outcomes associated with COVID-19 as well (6, 7).
We believe that it is crucial for the stroke community to relax guidelines and stroke pathways while continuously providing high quality of care, including treatment algorithms, post intravenous thrombolysis monitoring, diagnostic work up, disposition planning, prevention measures, in order to optimally care for stroke patients while minimizing the chances of contributing to the rapid spread of COVID-19.
These suggestions apply not only to individual hospitals, but larger systems as well. Stroke care often involves large networks of hospitals; commonly with a comprehensive “hub” and multiple spoke sites, which identify, start appropriate treatment and transfer stroke patients to the hub of the spoke for continued stroke care.
Given the economics of the healthcare system in the United States, large metropolitan cities frequently have separate hub and spoke systems that overlap geographically with each other to a significant extent.
It is a real possibility that one or more of these hub an d spoke systems may become overwhelmed with COVID-19 patients, thus it is important for hospital leadership to re-examine existing relationships to allow for smooth reallocation of resources, mobilizing workforce, optimizing new beds availability, and rapidly liberating ICU beds.
We present our recommendations for the management of acute stroke during the COVID-19 pandemic, in a chronologic fashion following care from the pre-hospitalization stage to rehabilitation; with the goal of adapting care without sacrificing quality despite potentially limited resources as suggested by Ezekiel and colleagues (8).
Prehospitalization
Stroke remains a medical emergency requiring ordinary urgent care even in the midst of the COVID-19 outbreak. Patients should continue to call 911 for symptoms suspicious for stroke. In addition to standard triage, the emergency medical system (EMS) personnel should screen over the phone for COVID-19 symptoms.
Patients with low suspicion for stroke, or mild symptoms with no potential indication for acute intervention may be evaluated via telemedicine (when possible) to aid in determination if immediate hospitalization is necessary.
Given the degree of community spread of COVID-19, along with cases of asymptomatic transmission, all patient with acute stroke symptoms should be treated as suspected or possible COVID-19 patients (frequently termed person under investigation, PUI), and all personnel physically in contact should wear appropriate personal protective equipment (PPE).
Of note, several centers in Chicago have seen a decline in stroke admissions and EMS calls for stroke are down by twenty percent. If this is a result of social distancing practices reducing the frequency of which patients with stroke are found, or from fear on behalf of patients of contracting COVID-19 by seeking out care is unclear.
Emergency room evaluation
In the emergency room, patients should be screened for COVID-19 prior to evaluation by the stroke team. Given the emergent nature of stroke care, difficulty in obtaining in many cases a complete review of systems and contact history, tele-stroke evaluation could be conducted in centers that have this capability.
It is preferable that all patient be given a mask to secure protection of the in person treating team. Appropriate personal protective equipment (PPE) should be used according to the CDC and local institution guidelines, (a so called ‘protected stroke code,’ (9)) along with treatment in designated location separate than the rest of the patients.
All patients should receive the standard of stroke care and should be evaluated for potential thrombolysis with intravenous tissue plasminogen activator (rtPA) or tenecteplase (TNK), along with endovascular thrombectomy (ET) when large vessel occlusion (LVO) is suspected.
It may be possible in select cases (such as a transient ischemic attack and small lacunar infarct with minimal deficits) to obtain expedited testing and critical evaluations in the emergency room, sparing a hospital admission (10).
Hospitalization
As the hospitals progress to becoming crowded out by the influx of COVID-19 patients, and as units are being converted to accommodate and treat infected patients, distribution of beds in separate isolated units should be planned in advance.
Patients receiving intravenous chemical thrombolysis should be monitored per current stroke guidelines; however, to avoid exposure of personnel, monitoring could be performed virtually with two-way video conferencing in some cases.
In the event that resources are so strained that standard protocol cannot be effectively adhered to, a difficult decision would have to be made to either with-hold thrombolysis, or utilize an abbreviated protocol for post thrombolysis monitoring (11).
As mentioned by a recent AHA position paper, treatment for eligible patients should continue to be offered, even if every vital sign assessment cannot occur at the prescribed time interval (12).
Current practices involve institutions admitting post thrombolysis patient to intensive care units (ICU); to avoid utilization of ICU beds, stroke patients post thrombolysis may be admitted to intermediate care unit (IMCU) or stroke ‘step down’ units, supervised by neurologists or vascular neurologists presuming there is a low probability of intensive care unit needs (12, 13) along with early acceptance of patients with small, stable intracerebral hemorrhages and those with subarachnoid hemorrhage at low risk for vasospasm as suggested by Chartrain and colleagues (14).
Patients with large strokes and otherwise requiring close intensive care monitoring for high risk of hemorrhagic transformation, intubation, stent re-occlusion or other critical care needs may be admitted to ICU in a designated COVID-19 rule out part of these units.
This would ideally occur under the supervision of an intensivist as a primary attending, with the vascular neurologist rounding remotely or with daily telephone-based discussion on management and treatment plans to minimize both PPE use as well as opportunities for inadvertent viral transmission.
Early transfer to IMCU or stroke unit should be initiated when the patient is deemed stable to liberate ICU beds. In centers that do not have IMUC beds, it may be possible to work with hospital administration, physicians and nursing to designate floor beds as such, to allow for less critically ill patients to move out of intensive care units if needed (15).
Diagnostic testing should be consolidated when possible and should only be ordered if deemed necessary to initiate appropriate management. For example, in patients with subcortical infarctions suspected to be due to small vessel disease, sonographic studies should be limited or even avoided to minimize exposure to technicians, especially as ultrasound machines may need to be cleaned between patients.
A patient with possible intracranial or extracranial atheromatous disease as an ischemic stroke etiology could have one test with a CT angiogram (CTA) of both the head and neck, as opposed to separate machine and technician utilization with both an MR angiogram (MRA) or CTA of the head with ultrasound imaging of the carotids.
For the most part, assuming low suspicion for endocarditis or cardiac thrombus, echocardiographic studies may be arranged and obtained as outpatient assuming an outpatient imaging center nearby is in operation.
Telemedicine should be used when possible during rounds with residents and fellows to minimize exposure of healthcare personnel, especially if COVID-19 infection is suspected or confirmed. Additionally, telemedicine may be utilized should the physicians test positive for the virus. Physicians who remain medically stable only mild (or absence of any) symptoms can continue to evaluate and treat patients remotely via telemedicine.
Rehabilitation planning
All healthcare workers caring for patients with COVID-19 are at elevated risk of exposure and should wear appropriate protective gears. Physical therapy (PT), occupational therapy (OT), speech therapy (ST), along with rehabilitation services are frequently involved in the care of stroke patients, and are an integral part of stroke recovery (16).
Additional care should be in place when consulting such services as opposed to involving all therapy services indiscriminately, and therapy services (when appropriate) should also emphasize teaching safe rehabilitative exercises that can be done by the patient ‘as homework’ when alone.
In a similar vein, the majority of the important work done by dietary consultants, pharmacists and stroke education nurses regarding risk factor modification could potentially be done without direct patient contact in many cases (17).
Family members
While obtaining history and medical information from family members is frequently necessary, especially when patients are aphasic or have mental status changes, many hospitals have appropriately restricted visitors or have instituted no visitor policy.
Extra effort will need to be made to reach out to families by phone to discuss a patient’s history, condition, treatment options, and discharge planning with family members and caregivers. Exceptions to the visitor policy, such as discussions regarding end of life care, should be made when appropriate.
Transfers
Stroke care often involves networks of hospitals; commonly a comprehensive “hub” with multiple smaller hospitals or “spoke” sites which transfer stroke patients to the hub of the spoke for care for higher level of care such as ET, or ICU care for massive infarcts with cerebral edema or for intracerebral hemorrhage (ICH).
Tele-stroke should be encouraged to evaluate patients and to prevent unnecessary transfers. For acute ischemic stroke, neuroimaging including arterial imaging should be obtained at the spoke site, and should be reviewed both by local radiologists as well as the tele-stroke physician to aid in appropriate patient selection for transfer.
The tele-stroke physicians may be required to make sobering decisions over when to utilize limited resources and risk COVID-19 spread when considering a potential transfer. For example, physician may choose not to accept a transfer of patients with massive hemorrhages, or patients with ischemic stroke who have very low likelihood of a good outcome post stroke treatment.
When transfer is deemed necessary, patients should be screened for COVID-19 at the spoke site. If clinical suspicion of COVID-19 infection is high, the hub interventional team should be prepared using appropriate PPE, with N95 respirators to protect from airborne particles and from liquid contamination during the endovascular procedure in the event that intubation is required. Otherwise, a surgical mask may be sufficient. Post intervention, patients should be admitted to the appropriate ICU units as discussed above.
Elective surgeries
Many institutions both nationwide and worldwide have postponed non-urgent surgical procedures for weeks (e.g. elective carotid or cardiac surgery) and urgent surgical intervention will take precedent. Non-urgent procedures are still being performed in some selected centers.
Discharge Planning
Many patients surviving the initial stroke are left with disabilities requiring intensive physical therapies in inpatient rehabilitation facilities. While early and intense rehabilitation is critical in stroke recovery, (16) discharges to acute rehabilitation institutions and long term facilities have been delayed due to concerns about the spread of COVID-19 infections in long term care facilities and nursing homes, particularly in some parts of the US.
The Seattle-based Life Care Center of Kirkland nursing home in Kirkland, Washington was considered “ground zero” in the COVID-19 pandemic by the CDC director. Case work managers and discharge planners will continue to work with admission teams at the inpatient rehabilitation centers to expedite discharges.
Ideally there would be no change in post hospitalization placement in acute and subacute rehabilitation facilities; realistically, however, hospitals may need to designate rehabilitation beds for patients who do not qualify for transfer to acute inpatient facilities, as well as discuss discharging patients home when medically stable and appropriate until the pandemic is under control if there is no practical placement option.
Establishing stroke networks
Lastly, establishing stroke networks within cities and collaboration between institutions should be seriously considered as the surge of COVID-19 worsens. The COVID-19 pandemic should be considered a war against humankind, and emergency planning should be encouraged by institutional authorities. It is not long until transfer of COVID-19 patients between facilities will be necessary as institutions become overwhelmed with the surge of patients.
The stroke community should encourage collaborations among stroke networks to establish a rotating weekly coverage for acute stroke care in a specified geographic area; thus both freeing hospital resources and releasing stroke call responsibilities and allowing those physicians to help in caring for patients on the COVID-19 units.
Source:
UCL



{kind=link}
[…] Study reveals a link between COVID-19 and clotting in blood vessels… […]