









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is causing the novel coronavirus disease–2019 (COVID-19) pandemic that has infected more than 5 million people and killed more than 350 000 worldwide.
The systematic investigation of clinically approved drugs is a priority to improve disease outcomes and invest resources to go to full-scale production.
The search for an effective therapy is ongoing actively but is currently limited in success. Perhaps we should look outside the box and consider what is hidden in plain sight such as the biological reasons why women are relatively protected from COVID-19 compared to men.
This review highlights experimental evidence that the steroid hormones 17β-estradiol (E2) and progesterone (P4), at high physiological concentrations, are powerful immunomodulators and argues that acute steroid therapy with the combination of E2 and P4 may represent a safe and viable therapeutic option that needs to be tested in clinical trials to mitigate severe COVID-19 outcomes.
Coronavirus Disease–2019 Mortality is Lower in Women Compared to Men
Since the beginning of the 21st century, 2 previous deadly zoonotic betacoronavirus outbreaks have crossed the species barriers to infect humans and exhibited the same apparent female protection from severe outcomes.
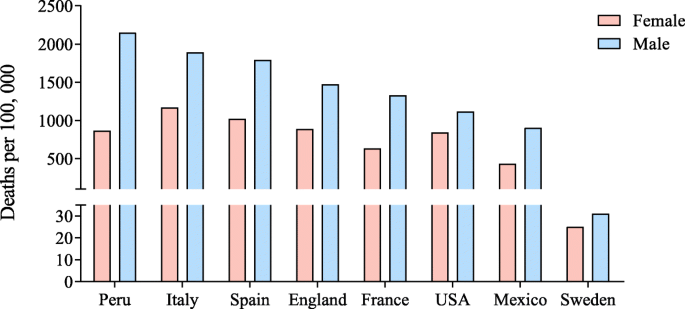
The first SARS-CoV outbreak emerged in 2002 in Guangdong province, China, and among 1755 hospitalized patients in Hong Kong the case fatality rates was 13% in women compared to 22% in men (1). During the ongoing Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak that began in 2012 in Saudi Arabia, among 425 reported cases, disease occurrence was lower among women (38% of cases) and the case fatality rate was 23% for women compared to 52% for men (2).
Today in China, Europe, and the United States, COVID-19 severity and mortality is consistently lower in women than in men (3-8).
Taking the most representative series to date, in the cohort of 1099 COVID-19 hospitalized patients in Wuhan, China, only 42% of the patients were women (4). Among severe cases (ie, admitted to an intensive care unit, requiring mechanical ventilation, or fatal), women accounted for 32% of patients (4).
Similarly, women represented only 18% of all COVID-19 admissions in intensive care units in the Lombardy region of Italy (9). In New York City, among 5700 hospitalized patients, women represented 33% of cases and 39% of deaths (7).
The International Severe Acute Respiratory and Emerging Infections Consortium (ISARIC) in a prospective observational cohort study of more than 17 000 patients in the United Kingdom reported that among hospitalized patients, women accounted for only 40%, with a 20% lower mortality than in men (10).
Although advancing age is associated with greater risk of mortality in both sexes, female protection remains evident (11). An analysis of COVID-19 data from Italy, Spain, Germany, Switzerland, Belgium, and Norway reveals that among all age groups older than 20 years, fatality rates are greater for males than females (12).
In contrast, male-female differences in the rate of confirmed SARS-CoV-2 infections are age dependent in all countries, being greater among females age 10 to 50 years and greater among males younger than 10 years and older than 50 years (12).
We interpret these data to suggest that biological sex differences contribute to female-biased protection against death, but sex-associated risk of exposure may affect rates of infection differently for males and females at differential ages.
A question then arises as to what biological factors are protective in women compared to men, and how can we harness these modifiable factors to mitigate COVID-19 morbidity and mortality?
Sex hormones and viral infection
Gonadal hormones not only are involved in the differentiation of reproductive organs, but also exert sex-specific regulation to multiple tissues including brain and those of the immune system [52a, 72a, 73a].
In humans, sex chromosome constitution (XX/XY) determines sex and the sex determining region Y (SRY) gene present on Y chromosome is the master regulator gene of sex differentiation [74a]. SRY drives testis differentiation by activating downstream genes, and the cascade of gene activation primes the gonad to secrete testosterone.
The secreted testosterone further helps to differentiate the male reproductive systems. Testosterone is also suggested to reach the brain and organize neuronal networks. Testosterone can mediate gene expression directly by binding to the androgen receptor (AR) or indirectly following conversion into estrogen by the enzyme aromatase [73a, 75a].
On the other hand, estrogen and progesterone are important hormones in females that lead to differential regulation of reproductive and immune systems [51a].
There are three different types of estrogens produced in females: estrone (E1), 17β-estradiol (E2), and estriol (E3). E2 is the predominant form that is produced by ovaries, and the level of hormones fluctuates during ovulation and pregnancy. Estrogens act through estrogen receptors (ERs) which exist in two forms, ERα and ERβ [76a].
The expression of both ERα and ERβ has been identified in human immune cells, including B and T lymphocytes, mast cells, macrophages, dendritic cells, monocytes, and natural killer cells [77a,78a,79a].
The expression of ERs have been shown to be cell specific as ERα was found to be the predominant form in CD4+ T cells, and ERβ was the predominant form in B cells [78a].
Sex- and age-specific expression of ERα has been identified in human monocytes with higher expression in post-menopausal females and males than pre-menopausal females [78a].
However, sex-dependent ER expression was not observed in B cells and T cells. Since there was no difference in ER expression in male and female T and B cells, the authors argued that the sex differences in immune response may not be a direct effect of estrogen but could be indirect through gonadotropin-releasing hormone [78a].
Nakada et al. using a murine model showed that the ERα RNA levels were higher in male hematopoietic stem cells (HSCs) than in female HSCs and that the level of ERβ was low in both male and female HSCs.
The authors also found that HSCs in females divide more frequently than in males. Interestingly, conditional deletion of ERα resulted in reduced HSC proliferation in females but not in males [80a].
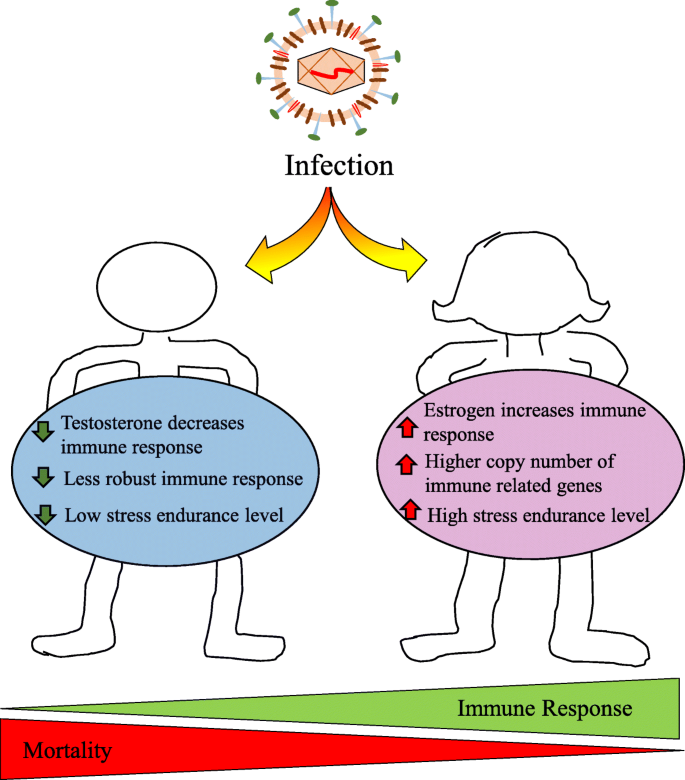
Males and females are under the influence of different hormonal milieu.
Testosterone has been shown to have immunosuppressive effect while estrogen has immunoenhancing effect [60a].
Testosterone has been found to inhibit T helper cell differentiation [81a] and positively correlate with the viral load of Venezuelan equine encephalitis virus in macaques [82a].
Testosterone is also known to decrease the responsiveness towards influenza vaccine [83]. Analysis of testosterone levels in females showed that the level is usually low in females suffering from autoimmune disease compared to healthy females [55a].
Furthermore, androgen ablation in male mice showed improved performance of immune cells towards prostate cancer [84a]. Androgen ablation also alters immune organs as the thymus and spleen have been reported to increase weight [85a].
Although the mature peripheral CD4 T cell population declined, the one that reached the spleen showed enhanced activation [85a]. This suggests that male sex hormones (androgens) could lead to susceptibility and severity towards pathogenic infections.
It is indicated that prostate cancer patients who are under androgen-deprivation therapy (ADT) to regulate androgen production have lowered risk for SARS-CoV-2 infection compared with patients who did not receive ADT [86a].
The authors argued that [86a] since TMPRSS2 expression is induced by androgens [87a], the ADT could downregulate TMPRSS2 and this in turn could be lowering SARS-CoV-2 infection.
It is suggested that ADT could be beneficial for COVID-19, and since this disease progresses rapidly, the ADT intervention will be beneficial during the initial stage of viral infection and not in later stages [88a].
However, the expression of TMPRSS2 in human male and female lungs is not different [89a, 90a], and in mice models, treatment with enzalutamide, an AR antagonist, did not result in decreased pulmonary TMPRSS2 expression [89a]. Hence, the use of AR antagonists to regulate TMPRSS2 expression for COVID-19 warrants further research.
Estrogen, on the other hand, provides protection against pathogens as it has antiviral properties in different viral infections including HIV, hepatitis C virus, Ebola, and human cytomegalovirus [91a]. Estrogen was shown to inhibit influenza A virus replication in cultured nasal epithelial cells isolated from female mice [91a].
Interestingly, the protective effect of estrogen was not observed in nasal epithelial cells isolated from male mice [91a]. Since SARS predominantly replicates in airways, higher estrogen levels in females may increase the protection from SARS infections [63a].
Inhibition of ER function using ER antagonist ICI 182,780 resulted in higher SARS-CoV infections in females. However, gonadectomy or treatment with the AR antagonist flutamide did not affect morbidity or mortality in male mice following SARS-CoV infection [63a].
Based on this, it was suggested that the estrogen receptor signaling plays an important role in coronavirus infection and mortality, while androgens do not play a role in pathogenesis [63a]. This suggests that estrogen signaling is critical in regulating viral infection and could be one of the reasons why females are showing fast recovery and low mortality from COVID-19.
Testis and viral clearance
The testis is an immune-privileged organ as both allo- and auto-antigens are incapable of provoking immune response. This characteristic is important for keeping the immunogenic germ cells away from the immune response [92a].
The unchecked immune system can react with the surface antigen on sperm cells known as meiotic germ cell antigen (MGCA), and this can result in infertility [92a]. Although testis is an immune-privileged organ, it can elicit innate immunity when microbial pathogens infiltrate the organ.
Viruses including HIV, cytomegalovirus, and mumps are known to infect testis and lead to testicular disorders [93a]. Moreover, viruses including Zika, Ebola, and Marburg have been isolated from semen samples and they are known to be transmitted sexually [94a].
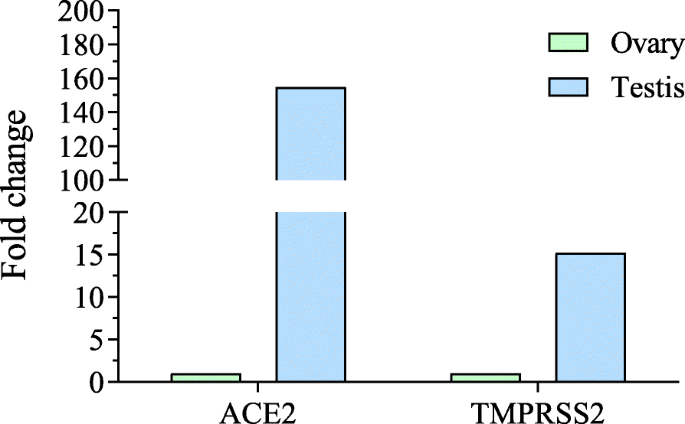
Shastri and coworkers showed that males in families required a longer time to recover from COVID-19 than other family members. The authors observed that testis had a high expression of ACE2 both at the mRNA and protein levels [26a].
The authors suggested that coronavirus can enter the testis and consequently lead to higher viral load and take more time for viral clearance. The total subjects in this study was only 68 (48 males and 20 females) with a median age of 37 years. A thorough study with a higher number of patients is required to support the author’s hypothesis.
In another study, coronavirus genetic material was detected in the semen samples of males infected with coronavirus [95a]. Analysis of RNA sequencing data obtained from the NCBI database [96] showed that both ACE2 and TMPRSS2 were highly expressed in the testis compared to the ovary (Fig. 4).
This supports the observation that the coronavirus may enter the human testis. The sex hormones in males were also altered following infection with SARS-CoV-2. Analysis of 81 infected men with SARS-CoV-2 showed increased luteinizing hormone (LH), but the ratio of testosterone to LH and follicle stimulating hormone to LH was decreased [97a].
Although coronavirus RNA was detected in semen samples, active viral particles have not been isolated from testis so far. Hence, the theory of involvement of testis in delayed viral clearance and high mortality in men [26a] should be taken with caution.
Disturbance of immune regulation in testis can result in orchitis, a condition where leukocytes infiltrate testis and damage seminiferous tubules and consequently result in infertility. Hence, whether testis is a contributing factor in poor prognosis and high mortality in men needs to be accessed more thoroughly.
In the SARS outbreak in 2002, higher mortality was observed in males compared to females.
The infected individuals showed multiple organ damage, and in males, testis was also affected with germ cell destruction, lack of spermatozoon, thickened basement membrane, and leukocyte infiltration [98a]. However, no viral particles or viral RNA was detected in the tissue samples and it was suggested that the virus-mediated testis damage was due to an immune response.
Role of the Proinflammatory Cytokine Storm in Coronavirus Disease–2019 Outcomes
Severe COVID-19 outcomes are associated with delayed and exaggerated innate immune responses, including hypercytokinemia and inflammatory cell infiltration in the lungs. Our current understanding of the disease, which is rapidly evolving as we write this review, is that patients with COVID-19 do not die from damage caused by virus replication, they die from the consequences of a so-called “cytokine storm” (13-16).
In an attempt to protect the body from SARS-CoV-2, immune cells infiltrate the lungs, causing hyperactivation of monocytes and macrophages, and elevated production of proinflammatory cytokines (eg, interleukin-6 [IL-6], interleukin-1β [IL-1β], tumor necrosis factor α [TNF-α]) and chemokines (eg, monocyte chemoattractant protein-1 (MCP-1/CCL2]) (15).
The cytokine storm is also associated with lymphopenia, and a study in 21 patients from Wuhan reported a decrease in CD4+ and CD8+ T cells, as well as suppressed interferon γ production by CD4+ T cells, which was associated with COVID-19 severity (15).
The local outpouring of chemokines and cytokines attracts more inflammatory cells, such as neutrophils and monocytes, into lung tissue, resulting in lung injury. Ironically, the cytokine storm is a result of the immune system responding to infection in an effort to protect the host, but results in acute respiratory distress syndrome and multiorgan failure (13, 14).
Increased production and elevated local and systemic IL-6 is hypothesized to be central to the development of the cytokine storm (17, 18).
Accordingly, therapeutic strategies targeting the inflammatory response such as IL-6 blockade (19) or the transplantation of mesenchymal stem cells to restore immune tolerance (20) are showing promising preliminary results in mitigating the cytokine storm. Here we discuss a paradigm in which therapy with the steroid hormones E2 and P4 could mitigate this virally induced innate immune inflammatory response.
Females Generally Exhibit Greater Immune Responses to Viruses
Females generally develop heightened immune responses compared to males.
In 1967, Butterworth et al reported that women produce higher levels of circulating immunoglobulins IgG and IgM than men (21), which was subsequently confirmed by multiple studies. Accordingly, following vaccination against influenza, yellow fever, rubella, measles, mumps, hepatitis, herpes simplex 2, rabies, smallpox, and dengue viruses, protective antibody responses are twice as high in women than in men (22).
Women also have higher frequencies of CD4+ T helper cells than men (23).
The biological reasons why females develop a more robust immune response than males against pathogens, including viruses, likely explain the observed female protection from COVID-19 fatal outcomes. First, females enjoy the genetic benefit of 2 X chromosomes and being a mosaic of X-linked genes (ie, randomly expressing alleles inherited from their mother or father), including more than 60 immune-response genes (24).
By contrast, males have only one X chromosome inherited from their mother. Several studies show that genetic diseases associated with deleterious X-linked alleles are more frequently observed in males (25).
Generally, there should be no dosage effect associated with position of 2 X chromosomes in females. Incomplete inactivation of immunoregulatory genes on the X chromosome in females, however, can cause a gene dosage imbalance between the sexes (26, 27), which is implicated in female-biased autoimmune diseases (28) and vaccine efficacy (29).
The Y chromosome also has immunoregulatory functions (30) that are linked to influenza outcomes, at least in mice (31).
Sex steroids are potent immune-modulators and the different concentrations of estrogens, P4, and androgens between women and men, in addition to the genetics described previously, are likely to influence COVID-19 immune responses and inflammatory outcomes.
This is especially important because acute and severe illnesses, such as COVID-19, may alter the function of the hypothalamic-pituitary gonadal axis and decrease the endogenous production of estrogens and P4.
Hormones are also amenable to therapeutic intervention. Later, we discuss immunomodulation provided by high physiological serum concentrations of estrogens and P4 as it relates to SARS-CoV-2 infection. This background knowledge is paramount to appreciate the potential benefits that E2 and P4 treatment could provide in the context of SARS-CoV-2–mediated hyperinflammation and acute respiratory distress syndrome.
Estrogens, Progesterone, and Immune Function
Estrogen receptors (ERs) are expressed in all immune cells, serving as transcriptional regulators of cellular function.
In human peripheral blood mononuclear cells, CD4+ T lymphocytes express higher levels of ERα messenger RNA than ERβ, whereas B cells express higher levels of ERβ than ERα messenger RNA (32).
Peripheral blood CD8+ T cells and monocytes express low but comparable levels of both ERs (32). Therapy with E2, leading to serum concentrations equivalent to ovulation or pregnancy, possess beneficial immunomodulatory and anti-inflammatory actions in mice and humans (reviewed in [24, 33]).
In most experimental human or rodent models, the anti-inflammatory actions of E2 on innate immunity includes the suppression of the production of proinflammatory cytokines, for example, IL-6, IL-1β, and TNF-α, by monocytes and macrophages (a major factor in the COVID-19 cytokine storm) and a strong inhibition of CCL2, thus preventing innate immune cells migration into inflamed areas, particularly neutrophils and monocytes.
E2 stimulates CD4+ T-helper cell production of anti-inflammatory cytokines, for example, interleukin 4 (IL-4), interleukin 10 (IL-10), and interferon γ.
Generally, high E2 concentrations favor helper T-cell type 2 (Th2)-type anti-inflammatory responses. E2 decreases interleukin 17 production by proinflammatory Th17 helper cells. E2 enhances the expansion of regulatory T cells (Tregs) thus promoting immune tolerance. E2 also stimulates antibody production by B cells (Figure 1).

Anti-inflammatory and immunomodulatory actions of estradiol and progesterone. High physiological concentrations of 17β-estradiol (E2) suppress the production of proinflammatory cytokines, for example, interleukin 6 (IL-6), interleukin 1β (IL-1β), and tumor necrosis factor α (TNF-α), and chemokine CCL2 by macrophages, thus preventing neutrophils and monocytes migration into inflamed areas. Progesterone (P4) also inhibits proinflammatory cytokines IL-1β and interleukin 12 production by macrophages and dendritic cells. High concentrations of E2 or P4 stimulate CD4+ T-helper cell production of anti-inflammatory cytokines, for example, interleukin 4 and interleukin 10, and favor Th2-type anti-inflammatory responses. E2 and P4 also enhance the expansion of regulatory T cells (Treg), thus promoting immune tolerance. Finally, E2 stimulates antibody production by B cells.
There is strong evidence in metabolic bone disease and virus-induced liver disease that estrogens inhibit disease pathogenesis through suppression of IL-6 production.
For example, estrogens inhibit osteoclast development and resorptive function in bone by inhibiting IL-6 gene transcription and production (34).
Additionally, the incidence of chronic hepatitis B–induced hepatocellular carcinoma (HCC) in humans shows a strong male predominance.
IL-6 is believed to be a key component in inflammation-associated tumorigenesis of HCC (35).
In a retrospective study of postmenopausal women with chronic hepatitis C, progression to liver fibrosis was decreased in women who took menopausal estrogen therapy, compared to women who did not (36). In a rat model of chemically induced HCC, males produced more IL-6 from liver Kupffer cells and were more prone to HCC than females (37). Estrogens protected males from HCC via inhibition of IL-6 production by Kupffer cells.
In a mouse model of acute lung inflammation by instillation of bacterial lipopolysaccharide, males and ovariectomized females exhibited increased lung infiltration of polymorphonuclear cells with elevated production of IL-6, IL-1β, and ICAM-1 (intercellular adhesion molecule-1), which was reduced by E2 treatment of males and ovariectomized females (38).
In preclinical models of influenza infection, estrogens exhibit powerful immunomodulatory actions leading to a more appropriate innate immune response in the lungs, which is associated with decreased proinflammatory cytokines and chemokine responses before the clinical disease develops (39-41).
In primary human nasal epithelial cell cultures, estrogenic compounds, including E2, signaling through ERβ significantly reduce influenza virus replication (42). Further, SARS-CoV-2 and SARS-CoV both produce deadly pneumonias with the same apparent female protection.
In a mouse model of SARS-CoV infection, female mice developed lower virus titers, lower infiltration with inflammatory monocyte, macrophages, and neutrophils producing fewer inflammatory cytokines (IL-6, IL-1β, and TNF-α) and chemokines (CCL2), resulting in milder pulmonary damage and a lower female mortality (20%) compared to males (80%) (43), a sex distribution similar to that observed in patients with SARS.
Importantly, the endogenous production of E2 in female mice was instrumental in this protection. Castration of males had no effect on the disease, while surgical removal of the ovaries or treatment with the ER antagonist fulvestrant in female mice infected with SARS-CoV resulted in the same pulmonary damages and mortality rate as in males.
Further, treatment of ovariectomized mice with the Food and Drug Administration–approved selective estrogen receptor modulator (SERM) tamoxifen—a mixed ER agonist and antagonist prescribed for the treatment of breast cancer—restored the female protection.
This study indicates that in a murine model of SARS-CoV infection, ovarian hormones and especially estrogens protected females from lethal pneumonia, and tamoxifen mimicked the female-biased protection. A screening of multiple Food and Drug Administration–approved compounds for anticoronavirus activity identified tamoxifen and toremifene (another SERM) among the top 10 most effective and safe drugs at inhibiting MERS-CoV and SARS-CoV infections in vitro (44).
Toremifene also inhibits Ebola virus infection in vitro and in vivo in mice (45). The mechanism of toremifene action seems related to the multiple cationic amphiphile structure of the molecule that impairs the late step of virus entry or fusion.
Taken together, these findings suggest that E2 and related SERMs have 2 potential protective mechanisms of action against SARS-CoV–mediated pneumonias in mice:
1) an estrogen-dependent decrease in the deadly innate immune response and cytokine storm in the lungs, thus preventing respiratory failure, and
2) specific to SERMs, an off-target direct inhibition of SARS-CoV replication and cytopathic effects.
P4 is another important immunomodulatory and anti-inflammatory hormone that is produced at high levels by the placenta during pregnancy. Progesterone receptors are expressed in most immune cells, including epithelial cells, macrophages, dendritic cells, lymphocytes, mast cells, and eosinophils (24).
However, P4 can also signal via glucocorticoid and mineralocorticoid receptors. P4 inhibits proinflammatory cytokines IL-1β and interleukin 12 production by human and rodent macrophages and dendritic cells. Progesterone favors the skewing of CD4+ T-helper cell responses from Th1-type toward Th2-type and the production of anti-inflammatory IL-4 and IL-10 cytokines (24, 46, 47).
Treatment of cord blood cells with P4 increases the percentage of FOXP3+ Treg cells (thus promoting immune tolerance), while decreasing the frequencies of proinflammatory Th17 cells (Fig. 1). Administration of P4 at concentrations mimicking the luteal phase to progesterone-depleted adult female mice conferred protection from lethal influenza A virus pneumonia (48).
In these mice, P4 treatment decreased the inflammatory environment of the lungs, improved pulmonary function, and promoted cell proliferation and pulmonary repair, which resulted in an earlier recovery, without effects on viral load.
Interestingly, in this case, P4 treatment promoted faster recovery by increasing transforming growth factor β, IL-6, interleukin 22, and the numbers of regulatory Th17 cells expressing CD39.
Importantly, progesterone promoted pulmonary tissue repair by upregulating the epidermal growth factor amphiregulin in the lungs (48).
Although influenza A virus infection is different and produces an immune reaction different from that induced by SARS-CoV-2 (eg, the beneficial effect of IL-6), this study provides important insight into the immunomodulatory and healing effects of P4. Further, P4 also seems to exhibit antiviral activity in VeroE6 cells infected with SARS-CoV-2 (49).
Pregnancy and Coronavirus Disease–2019
During pregnancy, the innate and adaptive immune responses shift from an inflammatory to an anti-inflammatory phenotype to avoid fetal rejection and favor passive transfer of maternal antibodies to the fetus (reviewed in [50]).
These effects, which are relevant to COVID-19 protection, are largely mediated by E2 and P4. During pregnancy, increased levels of E2 suppress many cytotoxic and innate immune inflammatory responses but stimulate antibody production by B cells (33, 51).
In fact, one of the most important immunological features of pregnancy is the increase in B-cell responses with enhanced antibody production due to dual stimulation by estrogens and P4, the production of which is maximal in the third trimester (33, 51).
P4 also stimulates the synthesis of progesterone-induced binding factor (PIBF) by lymphocytes, which promotes the differentiation of CD4+ T cells into Th2 cells secreting anti-inflammatory cytokines, including IL-4, interleukin 5, and IL-10 (52).
This explains why during pregnancy B-cell/antibody-driven diseases, like systemic lupus erythematosus, exacerbate; whereas T-cell–driven diseases with cytotoxic and innate immune responses, like rheumatoid arthritis or multiple sclerosis, improve (50, 53).
Pregnant women are not protected from SARS-CoV-2 infection but seem to be relatively protected from the severe outcomes of SARS-CoV-2. Currently, studies evaluating COVID-19 outcomes during pregnancy have not yet separated outcomes occurring during pregnancy (ie, when E2 and P4 concentrations are high) from those in the immediate postpartum period (ie, when E2 and P4 concentrations are undetectable).
In a Chinese retrospective series of 82 women (28 pregnant women, 54 reproductive-aged nonpregnant women) hospitalized in Wuhan with confirmed COVID-19, pregnant women exhibited comparable severity of disease, virus clearance time, and length of hospital stay compared with reproductive-aged nonpregnant women (54).
The authors concluded that pregnant women infected with SARS-CoV-2 have comparable clinical course and outcomes compared with control women. However, in this study, the nonpregnant women received more antiviral, corticosteroid, and immunoglobulin therapies than pregnant women and therefore the groups were not comparable in terms of treatments and related outcomes.
A larger retrospective review of 118 pregnant women admitted for COVID-19 pneumonia in China reported only 9 cases (8%) of severe pneumonia with hypoxemia. Notably, in 6 of these women, including 1 requiring mechanical ventilation, the exacerbation of pneumonia occurred during the postpartum period, after serum concentrations of E2 and P4 had already dropped (55).
Therefore, the actual number of severe cases in this study was 3 (2.5% of the pregnant population), which is less than the severity of COVID-19 in Chinese women in a similar age range (around 6%) (2).
In fact in the only published series of 9 pregnant women with fatal COVID-19, a detailed analysis of the cases reveals that 7 of these women deteriorated and died in the hours or days following delivery (56). Therefore, larger studies addressing COVID-19 mortality during pregnancy compared to early postpartum as a primary end point are needed to determine whether the hormonal environment of the third trimester is protective.
Immunomodulation by Hormone-Based Therapies in Women
Treatment of postmenopausal women with menopausal hormone therapy (MHT) and use of oral contraceptives by women during reproductive age are accompanied by concomitant physiological changes associated with increased concentrations of estrogens and progestins.
Thus, the effects of these 2 hormones cannot be separated. Most studies assessing the effect of MHT using E2 alone or in combination with progestins showed that MHT inhibits the production of proinflammatory cytokines (eg, TNF-α, IL-1β, and IL-6) by peripheral blood mononuclear cells ex vivo or in vivo in the serum of MHT-treated women (57-60).
In addition, transdermal E2 blunted the proinflammatory cytokine responses to an inflammatory challenge (59). The anti-inflammatory effect of E2 therapy in menopausal women with regard to low-grade systemic inflammation seemed to be observed mostly following transdermal rather than oral E2 administration and was not reproduced by conjugated equine estrogens. Bazedoxifene belongs to a new generation of SERMs used in combination with estrogens in oral menopausal hormone therapy.
In obese female mice, treatment with bazedoxifene decreases IL-6 and multiple markers of systemic inflammation (61).
However, this effect was not observed in a pilot randomized trial of 8-week treatment with oral estrogens and bazedoxifene in obese postmenopausal women (62). Likely, the absence of beneficial effect of orally administered estrogens on systemic inflammation is related to the first-pass liver metabolism following oral estrogen administration, which increases C-reactive protein production and markers of inflammation (63).
Transdermal and oral estrogen therapy with or without progestin increases CD19+ B-cell numbers and activity (64). Accordingly, the stimulating effects of menopausal therapy with estrogens and progestins on B cells promotes the progression of systemic lupus erythematosus in postmenopausal women (33).
Classical ERα, ERβ, and P4 receptors are present both in extranuclear and nuclear pools in most cells (65). To what extent each receptor cellular pool has collaborative or unique effects on immune function has not been determined and will be of interest for the design of future studies assessing the effect of sex-steroid receptor ligands in modulating immune functions.
Repurposing Estrogens and Progesterone to Mitigate Coronavirus Disease–2019 Mortality?
High physiological concentrations of E2 and P4 possibly synergize to mitigate innate immune cells production of proinflammatory cytokines, promote T cells’ anti-inflammatory responses and immune tolerance, and stimulate antibody production by B cells (Fig. 1).
In individuals with confirmed COVID-19, acute hormone therapy with E2 and P4 could mitigate the cytokine storm while increasing antibody production.
Pandemics such as SARS-CoV-2 provide little time for drug development. Repurposing existing and approved drugs that have already been tested in humans—and for which detailed information is available on their pharmacology, formulation, dose, and potential toxicity—provides an expedited and safe approach for off-label use of potentially life-saving therapeutics.
As discussed earlier, acute E2 and P4 treatment would be expected to blunt innate immune inflammatory responses and at the same time stimulate B-cell responses and antibody production (33, 51) without noticeable side effects.
A critical advantage of estrogen, SERMs, and progestin compounds is the depth of knowledge regarding their clinical efficacy and toxicity that has accumulated from decades of clinical and basic studies. Hormone therapy is used by millions of women for contraception and prevention of menopausal symptoms.
It is widely available in hospitals, inexpensive, manufacturable to scale, and can be prescribed immediately. As this review is being written, 2 clinical trials are testing E2 (ClinicalTrials.gov identifier NCT04359329) or P4 (ClinicalTrials.gov identifier NCT04365127) individually in COVID-19 patients.
It is worth considering the potential benefit of hormone therapy alone or in combination therapy with antiviral drugs or IL-6 blockade as an immune modulation in single-center off-label clinical trials. In an outbreak like this, and while we are waiting for a safe and efficient vaccine to be developed, the systematic investigation of clinically approved drugs is a priority to determine which compounds may mitigate the disease and to invest resources to begin full-scale production.
References
1. Karlberg J, Chong DS, Lai WY. Do men have a higher case fatality rate of severe acute respiratory syndrome than women do? Am J Epidemiol. 2004;159(3):229-231. [PMC free article] [PubMed] [Google Scholar]
2. Alghamdi IG, Hussain II, Almalki SS, Alghamdi MS, Alghamdi MM, El-Sheemy MA. The pattern of middle east respiratory syndrome coronavirus in Saudi Arabia: a descriptive epidemiological analysis of data from the Saudi Ministry of Health. Int J Gen Med. 2014;7:417-423. [PMC free article] [PubMed] [Google Scholar]
3. Mauvais-Jarvis F, Bairey Merz CN, Barnes PJ, et al. . Sex and gender: modifiers of health, disease and medicine. Lancet. 2020;396. [PMC free article] [PubMed] [Google Scholar]
4. Guan WJ, Ni ZY, Hu Y, et al. . Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708-1720. [PMC free article] [PubMed] [Google Scholar]
5. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. 2020;323(18):1775-1776. [PubMed] [Google Scholar]
6. COVID-19 National Emergency Response Center, Epidemiology and Case Management Team, Korea Centers for Disease Control and Prevention. Coronavirus disease-19: the first 7755 cases in the Republic of Korea. Osong Public Health Res Perspect. 2020;11(2):85-90. [PMC free article] [PubMed] [Google Scholar]
7. Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, and the Northwell COVID-19 Research Consortium Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area. JAMA. 2020;323(20):2052-2059. [PMC free article] [PubMed] [Google Scholar]
8. Klein S, Dhakal S, Ursin R, Deshpante S, Sandberg K, Mauvais-Jarvis F. Biological sex impacts COVID-19 outcomes. PLoS Pathog. 2020;16(6):e1008570. [PMC free article] [PubMed] [Google Scholar]
9. Grasselli G, Zangrillo A, Zanella A, et al. ; for the COVID-19 Lombardy ICU Network Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574-1581. [PMC free article] [PubMed] [Google Scholar]
10. Docherty AB, Harrison EM, Green CA, et al. . Features of 16 749 hospitalised UK patients with COVID-19 using the ISARIC WHO clinical characterisation protocol. [Published online ahead of print April 28, 2020.] medRxiv. Doi:10.1101/2020.04.23.20076042. [PMC free article] [PubMed] [Google Scholar]
11. Scully E, Haverfield J, Ursin R, Tannenbaum C, Klein SL. Sex is a variable in immune responses and COVID-19 outcomes. Nat Rev Immunol. 2020;20:442-447. [PMC free article] [PubMed] [Google Scholar]
12. Marina S, Piemonti L. Gender and age effects on the rates of infection and deaths in individuals with confirmed SARS-CoV-2 infection in six European countries. SSRN website. https://ssrn.com/abstract=3576790 or http://dx.doi.org/10.2139/ssrn.3576790. Posted April 28, 2020. Accessed June 20, 2020.
13. Chousterman BG, Swirski FK, Weber GF. Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol. 2017;39(5):517-528. [PubMed] [Google Scholar]
14. Ye Q, Wang B, Mao J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J Infect. 2020;80(6):607-613. [PMC free article] [PubMed] [Google Scholar]
15. Chen G, Wu D, Guo W, et al. . Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest. 2020;130(5):2620-2629. [PMC free article] [PubMed] [Google Scholar]
16. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ; HLH Across Speciality Collaboration, UK COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033-1034. [PMC free article] [PubMed] [Google Scholar]
17. Tanaka T, Narazaki M, Kishimoto T. Immunotherapeutic implications of IL-6 blockade for cytokine storm. Immunotherapy. 2016;8(8):959-970. [PubMed] [Google Scholar]
18. McGonagle D, Sharif K, O’Regan A, Bridgewood C. The role of cytokines including interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease. Autoimmun Rev. 2020;19(6):102537. [PMC free article] [PubMed] [Google Scholar]
19. Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab treatment in COVID-19: a single center experience. J Med Virol. 2020;92(7):814-818. [PMC free article] [PubMed] [Google Scholar]
20. Leng Z, Zhu R, Hou W. Transplantation of ACE2– mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging Dis. 2020;11(2):216-228. [PMC free article] [PubMed] [Google Scholar]
21. Butterworth M, McClellan B, Allansmith M. Influence of sex in immunoglobulin levels. Nature. 1967;214(5094):1224-1225. [PubMed] [Google Scholar]
22. Klein SL, Jedlicka A, Pekosz A. The Xs and Y of immune responses to viral vaccines. Lancet Infect Dis. 2010;10(5):338-349. [PMC free article] [PubMed] [Google Scholar]
23. Amadori A, Zamarchi R, De Silvestro G, et al. . Genetic control of the CD4/CD8 T-cell ratio in humans. Nat Med. 1995;1(12):1279-1283. [PubMed] [Google Scholar]
24. Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626-638. [PubMed] [Google Scholar]
25. Migeon BR. Females are Mosaics: X Inactivation and Sex Differences in Disease. 2nd ed. New York: Oxford University Press; November 12, 2013. [Google Scholar]
26. Carrel L, Brown CJ. When the Lyon(ized chromosome) roars: ongoing expression from an inactive X chromosome. Philos Trans R Soc Lond B Biol Sci. 2017;372(1733):20160355. [PMC free article] [PubMed] [Google Scholar]
27. Tukiainen T, Villani AC, Yen A, et al. ; GTEx Consortium; Laboratory, Data Analysis &Coordinating Center (LDACC)—Analysis Working Group; Statistical Methods groups—Analysis Working Group; Enhancing GTEx (eGTEx) groups; NIH Common Fund; NIH/NCI; NIH/NHGRI; NIH/NIMH; NIH/NIDA; Biospecimen Collection Source Site—NDRI; Biospecimen Collection Source Site—RPCI; Biospecimen Core Resource—VARI; Brain Bank Repository—University of Miami Brain Endowment Bank; Leidos Biomedical—Project Management; ELSI Study; Genome Browser Data Integration &Visualization—EBI; Genome Browser Data Integration &Visualization—UCSC Genomics Institute, University of California Santa Cruz Landscape of X chromosome inactivation across human tissues. Nature. 2017;550(7675):244-248. [PMC free article] [PubMed] [Google Scholar]
28. Souyris M, Cenac C, Azar P, et al. . TLR7 escapes X chromosome inactivation in immune cells. Sci Immunol. 2018;3(19):eaap8855. [PubMed] [Google Scholar]
29. Fink AL, Engle K, Ursin RL, Tang WY, Klein SL. Biological sex affects vaccine efficacy and protection against influenza in mice. Proc Natl Acad Sci U S A. 2018;115(49):12477-12482. [PMC free article] [PubMed] [Google Scholar]
30. Case LK, Wall EH, Dragon JA, et al. . The Y chromosome as a regulatory element shaping immune cell transcriptomes and susceptibility to autoimmune disease. Genome Res. 2013;23(9):1474-1485. [PMC free article] [PubMed] [Google Scholar]
31. Krementsov DN, Case LK, Dienz O, et al. . Genetic variation in chromosome Y regulates susceptibility to influenza A virus infection. Proc Natl Acad Sci U S A. 2017;114(13):3491-3496. [PMC free article] [PubMed] [Google Scholar]
32. Phiel KL, Henderson RA, Adelman SJ, Elloso MM. Differential estrogen receptor gene expression in human peripheral blood mononuclear cell populations. Immunol Lett. 2005;97(1):107-113. [PubMed] [Google Scholar]
33. Straub RH. The complex role of estrogens in inflammation. Endocr Rev. 2007;28(5):521-574. [PubMed] [Google Scholar]
34. Manolagas SC. Role of cytokines in bone resorption. Bone. 1995;17(2 Suppl 1):S63-S67. [PubMed] [Google Scholar]
35. Shi L, Feng Y, Lin H, Ma R, Cai X. Role of estrogen in hepatocellular carcinoma: is inflammation the key? J Transl Med. 2014;12:93. [PMC free article] [PubMed] [Google Scholar]
36. Di Martino V, Lebray P, Myers RP, et al. . Progression of liver fibrosis in women infected with hepatitis C: long-term benefit of estrogen exposure. Hepatology. 2004;40(6):1426-1433. [PubMed] [Google Scholar]
37. Naugler WE, Sakurai T, Kim S, et al. . Gender disparity in liver cancer due to sex differences in MyD88-dependent IL-6 production. Science. 2007;317(5834):121-124. [PubMed] [Google Scholar]
38. Speyer CL, Rancilio NJ, McClintock SD, et al. . Regulatory effects of estrogen on acute lung inflammation in mice. Am J Physiol Cell Physiol. 2005;288(4):C881-C890. [PubMed] [Google Scholar]
39. Robinson DP, Lorenzo ME, Jian W, Klein SL. Elevated 17β-estradiol protects females from influenza A virus pathogenesis by suppressing inflammatory responses. PloS Pathog. 2011;7(7):e1002149. [PMC free article] [PubMed] [Google Scholar]
40. Robinson DP, Hall OJ, Nilles TL, Bream JH, Klein SL. 17β-estradiol protects females against influenza by recruiting neutrophils and increasing virus-specific CD8 T cell responses in the lungs. J Virol. 2014;88(9):4711-4720. [PMC free article] [PubMed] [Google Scholar]
41. Vermillion MS, Ursin RL, Attreed SE, Klein SL. Estriol reduces pulmonary immune cell recruitment and inflammation to protect female mice from severe influenza. Endocrinology. 2018;159(9):3306-3320. [PMC free article] [PubMed] [Google Scholar]
42. Peretz J, Pekosz A, Lane AP, Klein SL. Estrogenic compounds reduce influenza A virus replication in primary human nasal epithelial cells derived from female, but not male, donors. Am J Physiol Lung Cell Mol Physiol. 2016;310(5):L415-L425. [PMC free article] [PubMed] [Google Scholar]
43. Channappanavar R, Fett C, Mack M, Ten Eyck PP, Meyerholz DK, Perlman S. Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection. J Immunol. 2017;198(10):4046-4053. [PMC free article] [PubMed] [Google Scholar]
44. Dyall J, Coleman CM, Hart BJ, et al. . Repurposing of clinically developed drugs for treatment of Middle East respiratory syndrome coronavirus infection. Antimicrob Agents Chemother. 2014;58(8):4885-4893. [PMC free article] [PubMed] [Google Scholar]
45. Johansen LM, Brannan JM, Delos SE, et al. . FDA-approved selective estrogen receptor modulators inhibit Ebola virus infection. Sci Transl Med. 2013;5(190):190ra79. [PMC free article] [PubMed] [Google Scholar]
46. Piccinni MP, Giudizi MG, Biagiotti R, et al. . Progesterone favors the development of human T helper cells producing Th2-type cytokines and promotes both IL-4 production and membrane CD30 expression in established Th1 cell clones. J Immunol. 1995;155(1):128-133. [PubMed] [Google Scholar]
47. Szekeres-Bartho J, Wegmann TG. A progesterone-dependent immunomodulatory protein alters the Th1/Th2 balance. J Reprod Immunol. 1996;31(1-2):81-95. [PubMed] [Google Scholar]
48. Hall OJ, Limjunyawong N, Vermillion MS, et al. . Progesterone-based therapy protects against influenza by promoting lung repair and recovery in females. PloS Pathog. 2016;12(9):e1005840. [PMC free article] [PubMed] [Google Scholar]
49. Gordon DE, Jang GM, Bouhaddou M, et al. . A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature. 2020;583(7816):459-468. [PMC free article] [PubMed] [Google Scholar]
50. Robinson DP, Klein SL. Pregnancy and pregnancy-associated hormones alter immune responses and disease pathogenesis. Horm Behav. 2012;62(3):263-271. [PMC free article] [PubMed] [Google Scholar]
51. Doria A, Iaccarino L, Arienti S, et al. . Th2 immune deviation induced by pregnancy: the two faces of autoimmune rheumatic diseases. Reprod Toxicol. 2006;22(2):234-241. [PubMed] [Google Scholar]
52. Szekeres-Bartho J, Faust Z, Varga P, Szereday L, Kelemen K. The immunological pregnancy protective effect of progesterone is manifested via controlling cytokine production. Am J Reprod Immunol. 1996;35(4):348-351. [PubMed] [Google Scholar]
53. Pazos M, Sperling RS, Moran TM, Kraus TA. The influence of pregnancy on systemic immunity. Immunol Res. 2012;54(1-3):254-261. [PMC free article] [PubMed] [Google Scholar]
54. Qiancheng X, Jian S, Lingling P, et al. . Coronavirus disease 2019 in pregnancy. Int J Infect Dis. 2020;95:376-383. [PMC free article] [PubMed] [Google Scholar]
55. Chen L, Li Q, Zheng D, et al. . Clinical characteristics of pregnant women with Covid-19 in Wuhan, China. N Engl J Med. 2020;382(25):e100. [PMC free article] [PubMed] [Google Scholar]
56. Hantoushzadeh S, Shamshirsaz AA, Aleyasin A, et al. . Maternal death due to COVID-19 Disease. Am J Obstet Gynecol. 2020;223(1):109.e1-109.e16. [PMC free article] [PubMed] [Google Scholar]
57. Bernard-Poenaru O, Roux C, Blanqué R, Gardner C, de Vemejoul MC, Cohen-Solal ME. Bone-resorbing cytokines from peripheral blood mononuclear cells after hormone replacement therapy: a longitudinal study. Osteoporos Int. 2001;12(9):769-776. [PubMed] [Google Scholar]
58. Rachoń D, Myśliwska J, Suchecka-Rachoń K, Wieckiewicz J, Myśliwski A. Effects of oestrogen deprivation on interleukin-6 production by peripheral blood mononuclear cells of postmenopausal women. J Endocrinol. 2002;172(2):387-395. [PubMed] [Google Scholar]
59. Puder JJ, Freda PU, Goland RS, Wardlaw SL. Estrogen modulates the hypothalamic-pituitary-adrenal and inflammatory cytokine responses to endotoxin in women1. J Clin Endocrinol Metab. 2001;86(6):2403-2408. [PubMed] [Google Scholar]
60. Aune B, Øian P, Omsjø I, Østerud B. Hormone replacement therapy reduces the reactivity of monocytes and platelets in whole blood—a beneficial effect on atherogenesis and thrombus formation? Am J Obstet Gynecol. 1995;173(6):1816-1820. [PubMed] [Google Scholar]
61. Kim JH, Meyers MS, Khuder SS, et al. . Tissue-selective estrogen complexes with bazedoxifene prevent metabolic dysfunction in female mice. Mol Metab. 2014;3(2):177-190. [PMC free article] [PubMed] [Google Scholar]
62. Lovre D, Peacock E, Katalenich B, et al. . Conjugated estrogens and bazedoxifene improve β cell function in obese menopausal women. J Endocr Soc. 2019;3(8):1583-1594. [PMC free article] [PubMed] [Google Scholar]
63. Mauvais-Jarvis F, Manson JE, Stevenson JC, Fonseca VA. Menopausal hormone therapy and type 2 diabetes prevention: evidence, mechanisms, and clinical implications. Endocr Rev. 2017;38(3):173-188. [PMC free article] [PubMed] [Google Scholar]
64. Porter VR, Greendale GA, Schocken M, Zhu X, Effros RB. Immune effects of hormone replacement therapy in post-menopausal women. Exp Gerontol. 2001;36(2):311-326. [PubMed] [Google Scholar]
65. Levin ER, Hammes SR. Nuclear receptors outside the nucleus: extranuclear signalling by steroid receptors. Nat Rev Mol Cell Biol. 2016;17(12):783-797. [PMC free article] [PubMed] [Google Scholar]
*-*-*-
26a.Shastri A, Wheat J, Agrawal S, Chaterjee N, Pradhan K, Goldfinger M, et al. Delayed clearance of sars-cov2 in male compared to female patients: high ace2 expression in testes suggests possible existence of gender-specific viral reservoirs. MedRxiv. 2020; 2020.2004.2016.20060566.
51a.Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16:626–38.CAS PubMed Article Google Scholar
52a.Schurz H, Salie M, Tromp G, Hoal EG, Kinnear CJ, Moller M. The x chromosome and sex-specific effects in infectious disease susceptibility. Hum Genomics. 2019;13.CAS PubMed Article Google Scholar
55a. Olsen NJ, Kovacs WJ. Gonadal steroids and immunity. J Endocrin Rev. 1996;17:369–84.
63a.Channappanavar R, Fett C, Mack M, Ten Eyck PP, Meyerholz DK, Perlman S. Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection. J Immunol. 2017;198:4046–53.CAS PubMed PubMed Central Article Google Scholar
- 72a.Ghosh S, Klein RS. Sex drives dimorphic immune responses to viral infections. J Immunol. 2017;198:1782–90.CAS PubMed PubMed Central Article Google Scholar
- 73a.Phoenix CH, Goy RW, Gerall AA, Young WC. Organizing action of prenatally administered testosterone propionate on the tissues mediating mating behavior in the female guinea pig. Endocrinology. 1959;65:369–82.CAS PubMed Article Google Scholar
- 74a.Koopman P. Sex determination: a tale of two sox genes. Trends Genet. 2005;21:367–70.CAS PubMed Article Google Scholar
- 75a.Arnold AP, Burgoyne PS. Are xx and xy brain cells intrinsically different? Trends Endocrinol Metab. 2004;15:6–11.CAS PubMed Article Google Scholar
- 76a.Nilsson S, Makela S, Treuter E, Tujague M, Thomsen J, Andersson G, et al. Mechanisms of estrogen action. Physiol Rev. 2001;81:1535–65.CAS PubMed Article Google Scholar
- 77a.Kovats S. Estrogen receptors regulate innate immune cells and signaling pathways. Cell Immunol. 2015;294:63–9.CAS PubMed PubMed Central Article Google Scholar
- 78a.Phiel KL, Henderson RA, Adelman SJ, Elloso MM. Differential estrogen receptor gene expression in human peripheral blood mononuclear cell populations. Immunol Lett. 2005;97:107–13.CAS PubMed Article Google Scholar
- 79a.Pierdominici M, Maselli A, Colasanti T, Giammarioli AM, Delunardo F, Vacirca D, et al. Estrogen receptor profiles in human peripheral blood lymphocytes. Immunol Lett. 2010;132:79–85.CAS PubMed Article Google Scholar
- 80a.Nakada D, Oguro H, Levi BP, Ryan N, Kitano A, Saitoh Y, et al. Oestrogen increases haematopoietic stem-cell self-renewal in females and during pregnancy. Nature. 2014;505:555–8.CAS PubMed PubMed Central Article Google Scholar
- 81a.Kissick HT, Sanda MG, Dunn LK, Pellegrini KL, On ST, Noel JK, et al. Androgens alter t-cell immunity by inhibiting t-helper 1 differentiation. 2014;111:9887–92.
- 82a.Muehlenbein MP, Cogswell FB, James MA, Koterski J, Ludwig GV. Testosterone correlates with venezuelan equine encephalitis virus infection in macaques. Virol J. 2006;3:19.PubMed PubMed Central Article CAS Google Scholar
- 83a.Furman D, Hejblum BP, Simon N, Jojic V, Dekker CL, Thiébaut R, et al. Systems analysis of sex differences reveals an immunosuppressive role for testosterone in the response to influenza vaccination. Proc Natl Acad Sci U S A. 2014;111:869–74.CAS PubMed Article Google Scholar
- 84a.Drake CG, Doody AD, Mihalyo MA, Huang CT, Kelleher E, Ravi S, et al. Androgen ablation mitigates tolerance to a prostate/prostate cancer-restricted antigen. Cancer Cell. 2005;7:239–49.CAS PubMed PubMed Central Article Google Scholar
- 85a.Viselli SM, Stanziale S, Shults K, Kovacs WJ, Olsen NJ. Castration alters peripheral immune function in normal male mice. Immunology. 1995;84:337–42.CAS PubMed PubMed Central Google Scholar
- 86a.Montopoli M, Zumerle S, Vettor R, Rugge M, Zorzi M, Catapano CV, et al. Androgen-deprivation therapies for prostate cancer and risk of infection by sars-cov-2: a population-based study (n = 4532). Ann Oncol. 2020.
- 87a.Lucas JM, Heinlein C, Kim T, Hernandez SA, Malik MS, True LD, et al. The androgen-regulated protease tmprss2 activates a proteolytic cascade involving components of the tumor microenvironment and promotes prostate cancer metastasis. Cancer Discov. 2014;4:1310–25.CAS PubMed PubMed Central Article Google Scholar
- 88a.Sharifi N, Ryan CJ. Androgen hazards with covid-19. Endocr Relat Cancer. 2020;27:E1–3.PubMed Article Google Scholar
- 89a.Baratchian M, McManus J, Berk M, Nakamura F, Erzurum S, Mukhopadhyay S, et al. 2020. No evidence that androgen regulation of pulmonary tmprss2 explains sex-discordant covid-19 outcomes.2020.2004.2021.051201.
- 90a.Stopsack KH, Mucci LA, Antonarakis ES, Nelson PS, Kantoff PW. Tmprss2 and covid-19: serendipity or opportunity for intervention? Cancer Discov. 2020;10:779–82.PubMed Article Google Scholar
- 91a.Peretz J, Pekosz A, Lane AP, Klein SL. Estrogenic compounds reduce influenza A virus replication in primary human nasal epithelial cells derived from female, but not male, donors. Am J Phys Lung Cell Mol Phys. 2016;310:L415–25.Google Scholar
- 92a.Zhao ST, Zhu WW, Xue SP, Han DS. Testicular defense systems: immune privilege and innate immunity. Cell Mol Immunol. 2014;11:428–37.PubMed PubMed Central Article Google Scholar
- 93a.Dejucq N, Jegou B. Viruses in the mammalian male genital tract and their effects on the reproductive system. Microbiol Mol Biol R. 2001;65:208–31.CAS Article Google Scholar
- 94a.Salam AP, Horby PW. The breadth of viruses in human semen. Emerg Infect Dis. 2017;23:1922–4.PubMed PubMed Central Article Google Scholar
- 95a.Li D, Jin M, Bao P, Zhao W, Zhang S. Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA Netw Open. 2020;3:e208292.PubMed PubMed Central Article Google Scholar
- 96a.Fagerberg L, Hallstrom BM, Oksvold P, Kampf C, Djureinovic D, Odeberg J, et al. Analysis of the human tissue-specific expression by genome-wide integration of transcriptomics and antibody-based proteomics. Mol Cell Proteomics. 2014;13:397–406.CAS PubMed Article Google Scholar
- 97a.Ma L, Xie W, Li D, Shi L, Mao Y, Xiong Y, et al. Effect of sars-cov-2 infection upon male gonadal function: a single center-based study. MedRxiv. 2020; 2020.2003.2021.20037267.



{kind=link}