










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A new therapy for influenza virus infections that may also prove effective against many other pathogenic virus infections, including HIV and COVID-19, has been developed by Purdue University scientists.
In an average year, more than 2 million people in the United States are hospitalized with the flu, and 30,000 to 80,000 of them die from the flu or related complications.
The Purdue team’s work is detailed in Nature Communications and uses a targeted therapy approach against the virus infections.
“We target all of the antiviral drugs we develop specifically to virus-infected cells,” said Philip S. Low, the Purdue Ralph C. Corley Distinguished Professor of Chemistry.
“That way, we treat the diseased cells without harming healthy cells. We use this capability to deliver immune-activating drugs selectively into flu-infected cells.
There is also the potential that this therapy will prove efficacious in people infected with COVID-19.”
The flu virus, like many other pathogenic viruses, exports its proteins into its host cell surface and then buds off nascent viruses in the process of spreading to adjacent host cells.
Because these exported viral proteins are not present in the membranes of healthy host cells, the Purdue team has exploited the presence of viral proteins in infected cells by designing homing molecules that target drugs specifically to virus-infected cells, thereby avoiding the collateral toxicity that occurs when antiviral drugs are taken up by uninfected cells.
“We chose to start our tests with influenza virus because the results can often be applied to other enveloped viruses,” Low said. “Our lab tests show that our process works in influenza infected mice that are inoculated with 100 times the lethal dose of virus.”
Low said the new therapy may prove effective against other pathogenic virus infections such as hepatitis B, HIV and respiratory syncytial virus (RSV).
Estimates from the centers for disease control and prevention (CDC) report that between 9 and 45 million new cases of influenza occur each year in the USA, leading to 140,000–810,000 hospitalizations/year and 12,000–61,000 deaths/year1. The annual financial burden associated with treating these illnesses has been estimated at $4.6 billion and costs stemming from the accompanying loss of work have been projected at $7 billion2.
While most influenza virus infections remain nonlethal and containable, their worldwide impact on morbidity and mortality remains one of the most adverse of any infectious disease.
Three general approaches have demonstrated efficacy in controlling influenza virus. First, vaccines against common influenza antigens have proven successful in limiting the severity and spread of the virus during years when the most aggressive viral strains are correctly predicted. Unfortunately, due to the rapid evolution of the virus, annual formulations of the vaccine often fail to match the most virulent strains, resulting in many vaccinated patients still contracting an infection3–5.
Second, neuraminidase inhibitors have been designed to block the viral neuraminidases required for release of the virus from its host cell surface6,7. Although four neuraminidase inhibitors (zanamivir, oseltamivir, peramivir, and laninamivir) have been approved for treatment of influenza in different parts of the world, they commonly provide little benefit when administered more than two days after symptoms appear, leaving a large fraction of infected individuals with no treatment to mitigate symptoms6.
Moreover, the emergence of low levels of variant viruses with reduced susceptibility to the above neuraminidase inhibitors has raised concerns that widespread circulation of viruses with reduced drug susceptibility can occur8–10.
Third, baloxavir marboxil (Xofluza) and related drugs impede the synthesis of viral mRNAs by suppressing the cap-dependent endonuclease of both influenza A and B viruses11,12.
However, although studies reveal that baloxavir can reduce the viral load and alleviate influenza symptoms, baloxavir-resistant strains have already been identified in patients13, suggesting that its efficacy as a broad-spectrum therapy may be affected.
In the study below, we explore a hybrid of the above two therapeutic approaches, where we take advantage of both the potent antiviral activity of a broad spectrum viral neuraminidase inhibitor and the powerful immunological function of a vaccine.
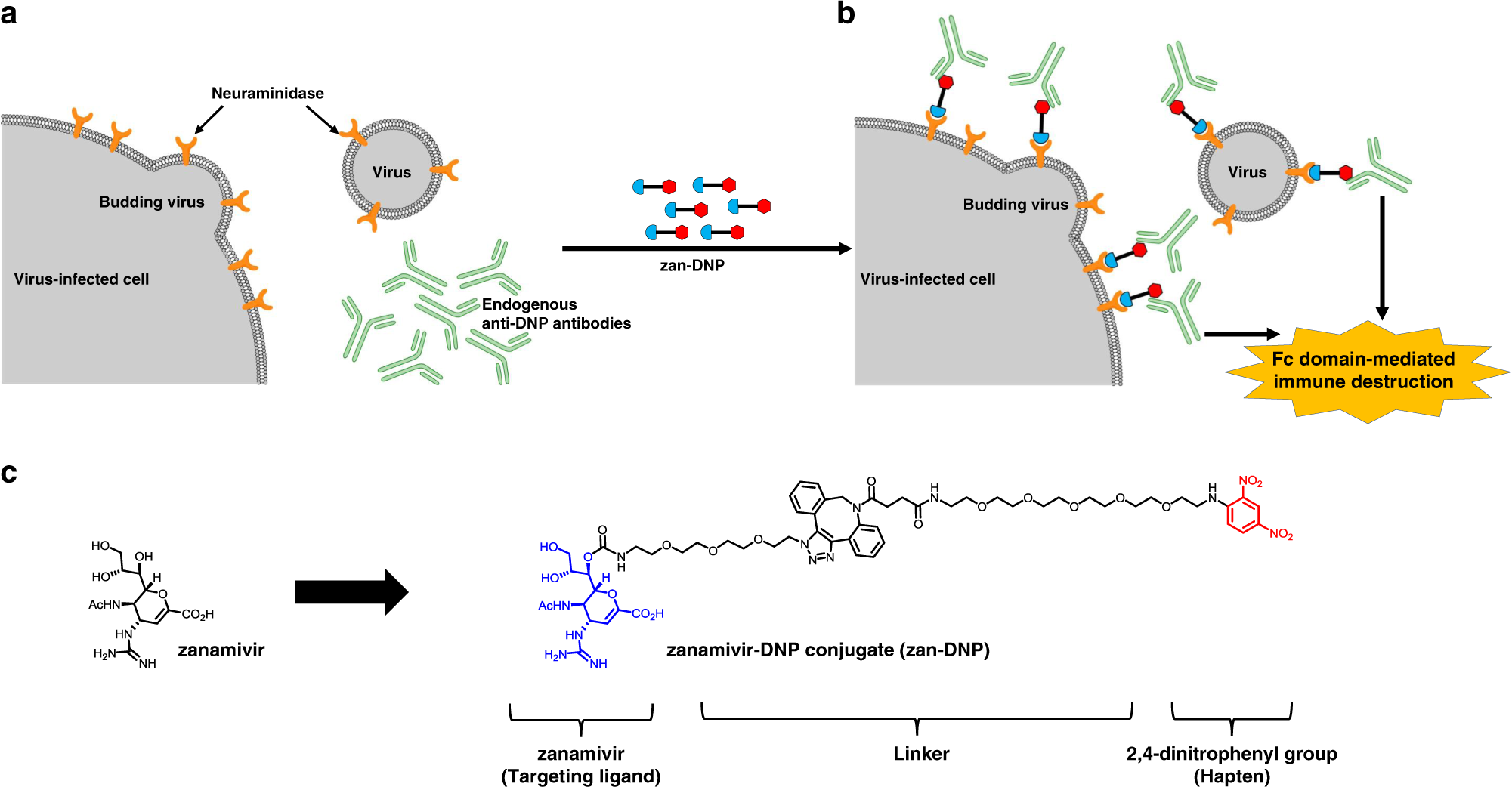
Briefly, we exploit the fact that influenza virus-infected cells express one or more viral proteins on their cell surfaces14, thereby distinguishing them from adjacent healthy cells (Fig. 1a).
While cell surface viral neuraminidases are intrinsically antigenic, we enhance their immunogenicity by decorating them with a potent hapten (i.e., in this case, a dinitrophenyl moiety; DNP) (Fig. 1b). Even though the origin of the antibodies against DNP and other nitroarenes is not known, they comprise ~1% of circulating antibodies in human serum and are competent to induce ligand-targeted cytotoxicity15–18.
Moreover, rather than using a functionally inert ligand to target this hapten, we deliver the DNP moiety attached to a potent neuraminidase inhibitor, namely zanamivir (Fig. 1c), since zanamivir binds to neuraminidases of all known subtypes/lineages of influenza A and B viruses19.
Because virtually all humans naturally express anti-DNP antibodies18, the resulting zanamivir-DNP conjugate (zan-DNP) can not only block the activity of an essential viral enzyme, but also recruit the immune system to attack the virus or virus-infected cells.
Here, we show that zan-DNP inhibits neuraminidases of both influenza A and B viruses and concurrently recruits anti-DNP antibodies to virus-infected cells. Because this anti-DNP binding mediates destruction of the opsonized virus and virus-infected cells, treatment with zan-DNP is observed to eradicate even the severe viral infections where mice are inoculated with 100× MLD50 of viral load and therapy is not initiated until 3 days post-infection. Considering that a single intranasal or intraperitoneal dose of zan-DNP yields a complete response, we suggest that further development of zan-DNP as a universal anti-influenza therapy is warranted.
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7645797/
More information: Xin Liu et al, A universal dual mechanism immunotherapy for the treatment of influenza virus infections, Nature Communications (2020). DOI: 10.1038/s41467-020-19386-5



{kind=link}