








 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



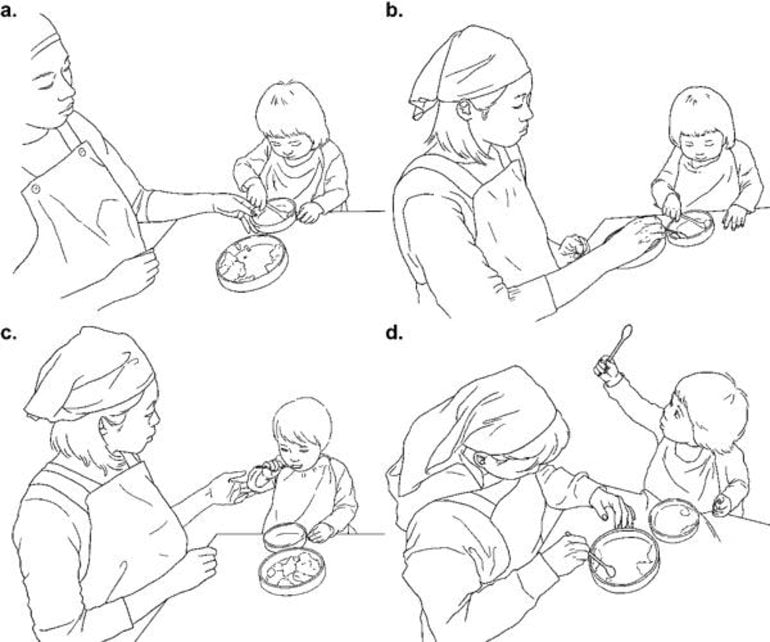
When toddlers begin to use a spoon to eat by themselves, what kind of interactions occur between them and their caregiver to facilitate this behavior?
An international research collaboration led by Kobe University’s Professor NONAKA Tetsushi (Graduate School of Human Development and Environment) and the University of Minnesota’s Professor Thomas A. Stoffregen investigated the interactions between toddlers learning to use a spoon and their caregivers during mealtimes at a daycare center in Japan.
The research findings were published in Developmental Psychobiology on December 11, 2020.
Research Findings
A 10-month longitudinal observation of 12 toddler-caregiver dyads during mealtimes was carried out at a daycare center in Japan. The onset of independent spoon-feeding was identified for each toddler (mean age: 17.88 months).
The researchers then investigated the temporal relationship between the following terms in the video data of mealtimes immediately after this onset:
- 1. The caregiver’s assistive actions,
- 2. The toddler’s spoon usage,
- 3. The toddler’s gaze towards the caregiver.
Analysis of the results showed that toddlers were more likely than chance to move their spoons towards the food immediately after the caregiver had changed the position of the plates or the food on them in order to give the toddler the opportunity to try to feed themselves.
The researchers also found that the amount of time that toddlers spent looking at the caregiver’s hands was significantly longer than the time spent looking at their face. Moreover, toddlers were 8 times more likely to look at the caregiver’s hands than perform any other action when the caregiver was moving items around on the table.
In addition, the researchers found a clear difference between the circumstances in which toddlers looked at the caregiver’s face and the circumstances in which they looked at the caregiver’s hands. Toddlers were most likely to look at the face in order to check whether or not the caregiver was watching their behavior, either after the toddler had fed themselves with the spoon or after they had played with the spoon in a manner unrelated to eating.
These incidences of toddlers’ checking caregiver reactions were too numerous to be chance occurrences.
These results show that during mealtimes, toddlers’ gazes towards the hands and gazes towards the face have different roles in communication. The emergence of the toddler’s ability to appropriately use a spoon to eat by themselves is the result of the following reciprocal interactions involving the caregiver’s behavior and the toddler’s attention:
- 1. The caregiver’s manipulation of the surroundings and the toddler’s attention to the caregiver’s hands,
- 2. The reaction of the caregiver to the toddler’s behavior and the toddler’s attention to the caregiver’s face.
Feeding experiences during the first year of life are recognised as playing an important role in laying down the foundations of weight and eating behaviour (Snethen, Hewitt, & Goretzke, 2007). Although research has typically focused on milk feeding (Bartok & Ventura, 2009), increasing recognition is being given to the latter part of infancy, in particular when and how infants are introduced to complementary foods (Brown, Jones, & Rowan, 2017; Daniels, Mallan, Fildes, & Wilson, 2015).
In terms of how infants are introduced to complementary foods, a baby‐led weaning (BLW) approach, where infants self‐feed family foods, has been proposed to promote healthier weight gain trajectories than a traditional spoon‐feeding approach.
Research with mothers who follow BLW highlights a perception that infants have greater control over their intake of food and therefore demonstrate greater satiety responsiveness (regulation of food intake), supporting a healthy weight (Arden & Abbott, 2015; Brown & Lee, 2013; Rapley, 2015).
Research examining the impact of a baby‐led approach upon satiety responsiveness is mixed. In one study, infants aged 18–24 months who followed a baby‐led approach to starting solids were rated as more satiety responsive compared with those who had been spoon‐fed (Brown & Lee, 2015).
Conversely, in a more recent study, no significant difference was found between weaning approach groups (Komninou, Halford, Harold, 2019), and in a trial of a baby‐led versus standard weaning approach, BLW was actually associated with reduced satiety responsiveness at 24 months (Taylor et al., 2017).
Additionally, research examining the impact of weaning style upon infant and child weight is mixed. In two cross‐sectional studies based in the UK, a BLW approach was associated with a lower weight and reduced incidence of overweight among infants aged 18–24 months (Brown & Lee, 2015) and in preschool children (Townsend & Pitchford, 2012). However, in both studies, mothers who participated were self‐selecting, and both relied on maternal self‐report of infant weight of many of the infants.
Conversely, the New Zealand Baby‐Led Introduction to SolidS (BLISS) study—a trial that randomised mothers to either a baby‐led approach or traditional feeding approach using research‐led clinical measurements of infant growth—found no difference in infant weight at 12 or 24 months.
However, adaptations made to the specific baby‐led feeding approach encouraged may differ from how many families practice BLW in the community. Families were encouraged to offer their infants protein at every meal, with an emphasis on good fats, as there was concern that infants may not self‐feed sufficient calories (Taylor et al., 2017).
Infant growth is affected by many factors, and it is unlikely that any one behaviour in insolation will affect weight trajectories. As noted, considerable research has shown the protective impact of breastfeeding upon infant weight.
Although differences in milk content partly explain this, through breast milk having a lower protein content alongside bioactive properties that can support appetite regulation (Chan et al., 2017), differences in feeding style have also been identified.
Compared with bottle feeding, breastfeeding is associated with a more responsive feeding style (Brown, Raynor, & Lee, 2011), lower intake of milk (Hester, Hustead, Mackey, Singhal, & Marriage, 2012), and greater satiety responsiveness (Brown & Lee, 2012).
Research has not considered how milk feeding and method of introduction of complementary foods might interact to affect weight gain trajectories. In the BLISS trial, breastfeeding rates were higher than average, with New Zealand breastfeeding rates considerably higher than U.K. breastfeeding rates. In the cross‐sectional studies, breastfeeding duration was either used as a control variable (Brown & Lee, 2015; Komninou, Halford, & Harrold, 2019) or not considered (Townsend & Pitchford, 2012).
Milk feeding method has been shown to interact with timing of complementary feeding to affect weight. In the European IDEFICS (Identification and prevention of Dietary‐ and lifestyle‐induced health EFfects In Children and infantS) study, infants who were breastfed throughout the first year had a reduced risk of overweight compared with those who discontinued breastfeeding (Papoustou, Savva, Hunsberger, Jilani,, & Ahrens, 2018).
Similarly, in a U.S. birth cohort study of 847 children, infants who were introduced to complementary foods before 4 months had an increased risk of overweight but only if they were formula fed (Huh, Rifas‐Shiman, Taveras, Oken, & Gillman, 2011). This impact has been attributed to bottle‐fed infants being less likely to reduce their intake of milk when complementary foods are added to the diet (Heinig, Nommsen, Peerson, Lonnerdal, & Dewey, 1993; Noble & Emmett, 2006). Therefore, it is likely that milk feeding may interact with method of introducing complementary foods to affect infant growth.
The aim of this study was to conduct the first U.K.‐based study examining the impact of method of complementary feeding and how it interacts with milk feeding upon infant growth during the first year using solely researcher‐led measurements.
DISCUSSION
This study explored the impact of method of introducing complementary foods upon growth at 3–12 months, considering further how this might interact with milk feeding method. It found no significant differences in weight or BMI between infants introduced to complementary foods via spoon‐feeding or self‐feeding but found that infants who were spoon‐fed were significantly longer than those who were self‐feeding.
However, no significant differences were found for current method of introduction. Moreover, although no significant difference was seen in the growth of infants who were self‐feeding according to milk type, infants who were both spoon‐fed and fully formula fed were significantly heavier than those spoon‐fed alongside being breastfed.
The findings have important considerations for how responsive feeding may be a key aspect of growth in the latter part of infancy.
First, infants who were following a traditional complementary feeding approach were longer than those that were self‐feeding. It is possible that method of complementary feeding is affecting length gains due to differences in infant diet.
Spoon‐fed infants are more likely to consume fortified infant cereals when compared with self‐feeding infants, especially when introduced to solid foods at an earlier date (Roess et al., 2018). Iron fortified cereals have been linked to increased gains in length‐for‐age at 12 months in Indonesia (Diana et al., 2017), although this finding has not been replicated in developed regions (Pasricha, Hayes, Kalumba, & Biggs, 2013).
However, iron fortified infant foods also contain cow’s milk protein or are made up with further added cow’s milk or infant formula. High protein intake has been associated with rapid increases in weight and length during infancy (Heinig et al., 1993) and is a risk factor for later overweight and obesity (Hoppe, Mølgaard, Thomsen, Juul, & Michaelsen, 2004; Michaelsen & Greer, 2014).
Although many studies focus just on weight gains, or consider length only in relation to BMI (Rogers & Blissett, 2017), rapid length growth in itself can be a predictor of later obesity (Belfort, Gillman, Buka, Casey, & McCormick, 2013; Elks et al., 2010; Monteiro, Victora, Barros, & Monteiro, 2003). Therefore, it would be interesting for future research to consider the longer term growth trajectories of infants with greater length gains in the early months of life.
However, a number of aspects in the data suggest that infant length may be determining complementary feeding approach. The association we found between spoon‐feeding and longer length was not affected by longer exposure to spoon‐feeding nor was any difference in LAZ seen in the longitudinal analysis. LAZ was associated with method of introducing complementary food but not method at time of measurement.
It may be the “thinner” appearance of a longer baby may be prompting the decision to start complementary feeding earlier. Research has shown that concerns over infant weight and energy intake are associated with an earlier introduction of complementary foods (Arden, 2010; Brown & Rowan, 2016), which for infant developmental reasons would require a spoon‐feeding approach.
Indeed, in one study, mothers reported that one reason they chose to spoon‐feed was that they were worried their baby wouldn’t eat enough (Cameron et al., 2013), whereas mothers who chose a baby‐led approach are less concerned around intake of food (Brown & Lee, 2012).
Neither weight nor BMI differed between the complementary feeding groups, supporting the BLISS study findings (Taylor et al., 2017). There are a number of reasons why a baby‐led approach might not be affecting weight gain. First, the 6‐ to 12‐month period may be too early for differences to emerge, and the percentage of overweight children in the study was small.
This may change over time, and one study has shown that pre‐school children who followed a BLW approach were less likely to be overweight compared with those spoon‐fed, although retrospective recall and some self‐reporting of weight limit these findings (Townsend & Pitchford, 2012).
Indeed, although in this study longitudinal analysis did not reach significance, the difference in weight change and BMI change was greater in the spoon‐fed group. If these infants followed on the same trajectories, these differences are likely to become significant over time.
Second, as BLW grows in mainstream popularity, the approach may become less “healthy.” Critics of BLW have posited that there is a potential for BLW to allow babies to eat snacks as finger foods such as crisps and biscuits (Cameron, Heath, & Taylor, 2012), and research in larger samples exploring a “looser” version of BLW, where infants self‐fed most of the time, highlighted an increased intake of such snack foods in this group (Rowan, Lee, & Brown, 2019).
However, it might also be that examining method of introducing complementary foods in isolation is not enough, and this is highlighted by differences in weight found in the sample when both milk feeding and method of complementary feeding were considered together. Although no significant difference in the overall sample for weight or BMI was seen between the approach groups, infants who were spoon‐fed and fully formula fed were significantly heavier than those exclusively or partially breastfed, but no impact of milk feeding was seen for self‐feeding infants.
Again, this relationship might be bidirectional. Potentially, experience of both spoon‐feeding and bottle feeding decreases infant opportunity to self‐regulate intake. Breastfed infants typically have more control over their intake of milk as the amount consumed is not visible, whereas formula‐fed infants can be encouraged to finish a bottle (Li, Magadia, Fein, & Grummer‐Strawn, 2012).
Mothers who breastfeed are more likely to adopt a responsive feeding approach, letting their infant set the pace of feeds and worrying less around monitoring intake of milk (Brown et al., 2011; Brown & Lee, 2013). Breastfed infants have been identified as better able to regulate their appetite as toddlers (Brown & Lee, 2012) and adolescents (Reyes et al., 2014), although not all studies are conclusive (Hathcock et al., 2014). Additionally, mothers who follow a BLW approach have been shown to be more responsive in their feeding style, showing lower control in terms of restriction, pressure to eat, and monitoring (Brown & Lee, 2011).
Therefore, infants who are both spoon‐fed and bottle fed may have lower opportunity to regulate their own intake compared with infants who can regulate over different meals even if one aspect of their feeding approach (e.g., spoon or bottle) is more “controlling.”
This may be affecting weight, although research examining the longer term impact of responsive feeding in infancy is sparse. However, a large body of literature suggests that for older children, a responsive feeding style is associated with the most positive weight outcomes. For example, in a 2015 systematic review of the literature, the authors concluded that restrictive and controlling feeding practices were associated with higher child BMI at ages 4–12 years (Shloim, Edelson, Martin, & Hetherington, 2015).
It is also possible that mothers who are formula feeding and whose infant is already at increased likelihood of being heavier (Dewey, Heinig, Nommsen, Peerson, & Lonnerdal, 1992; Li, Magadia & Grummer‐Strawn, 2012) are drawn to a spoon‐feeding approach. In this study and others, there is a strong association between spoon‐feeding and bottle feeding (Brown & Lee, 2010; Morison et al., 2016; Taylor et al., 2017; Townsend & Pitchford, 2012), potentially due to preferred overall maternal feeding style. Both bottle feeding (Brown et al., 2011) and spoon‐feeding (Cameron et al., 2013) are associated with maternal concerns around intake.
Maternal general feeding style appears to be stable over time (Black & Aboud, 2011) with longitudinal research showing that mothers who encouraged their infant to finish their bottle as a baby were more likely to use higher pressure to eat at age 6 (Li, Scanlon, May, Rose, & Birch, 2014). It would be interesting in future research to explore whether mothers who bottle feed but follow BLW were more responsive than average in their bottle feeding approach.
This study does have limitations; participants were older with a higher level of education, and breastfeeding rates were higher than within the general population, although this enabled stronger milk feeding group analyses. Infants were recruited to the research at different ages (around 6–12 months), and thus, the length of time for mothers to recall earlier information (e.g., birth feeding data) was variable, potentially affecting reliability.
However, infant feeding data are likely to be accurately recalled within a time period of 3 years (Li, Scanlon, and Serdula (2005), so variability of 6 months is unlikely to have been problematic. Additionally, most infants were considered a healthy BMI (albeit with a broad range of measurements), meaning that analysis of weight groups (underweight, normal, and overweight) would have been underpowered. The small group size of the subgroup with two measurements (longitudinal analyses) was also slightly underpowered, and so these results should be interpreted with caution.
Limitations aside, this study explored a so‐far under‐researched area, highlighting a possible cumulative effect of bottle feeding and spoon‐feeding. It is the first study in the United Kingdom considering method of introducing solid foods to provide prospective and longitudinal measurements. The findings have important implications for the responsive feeding literature and considering infant weight to be a consequence of a cumulation of experiences rather than just one aspect in isolation.
reference link: https://onlinelibrary.wiley.com/doi/full/10.1111/mcn.12941
Source: Kobe University



{kind=link}