











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A combination of robust vaccination programmes and strict physical distancing rules could avoid recurring peaks of COVID-19 without the need to rely on stay-at-home restrictions, according to a new study by epidemiologists and demographers from WorldPop at the University of Southampton, in collaboration with The Chinese University of Hong Kong.
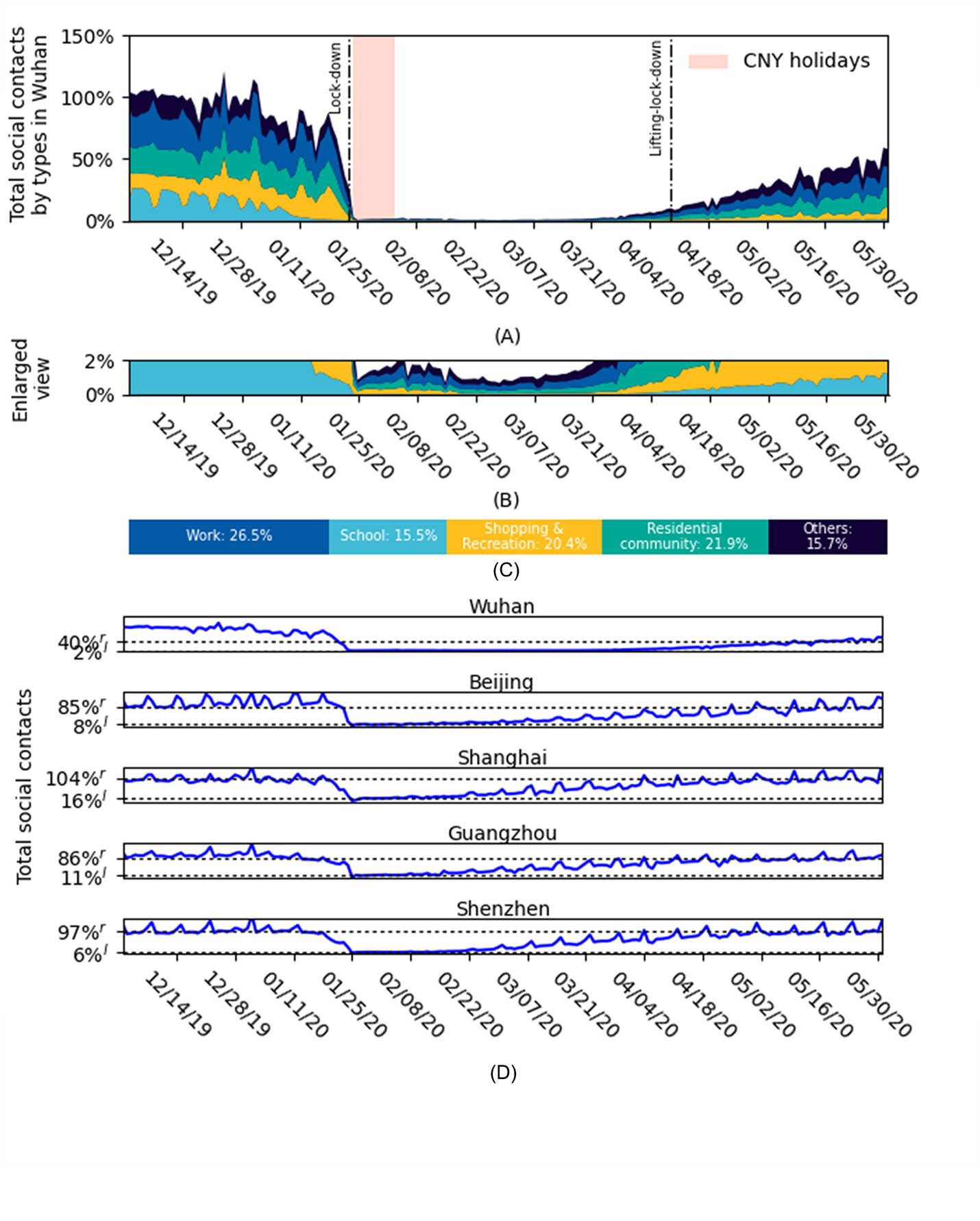
This research used anonymised mobile phone geolocation data with epidemiological and coronavirus case data from China to model the potential impact of vaccination and physical distancing on virus transmission.
They predicted the effect of different combinations of interventions on low, medium and high density cities in the country.
The impact of physical distancing in containing future resurgences of COVID-19 depends greatly on the intensity of measures, population density, and the availability of vaccines across geographical areas and time. The researchers set out to gain a greater understanding of the relationship between these factors.
The findings are published in the journal Nature Human Behaviour.
The team predicts that in most cities, vaccination programmes and physical distancing combined will be enough to contain virus resurgence without the need to greatly restrict population mobility. Containment in this study was defined as maintaining a low transmission rate, or ‘R’ below one.
The researchers report cities with medium and high density populations will need both vaccination and distancing to prevent future intense waves of COVID-19, until herd immunity is reached. However, they suggest cities with low populations and effective vaccination could fully interrupt transmission without the need for physical distancing. In all cities, full ‘stay-at-home’ lockdowns would no longer be necessary.
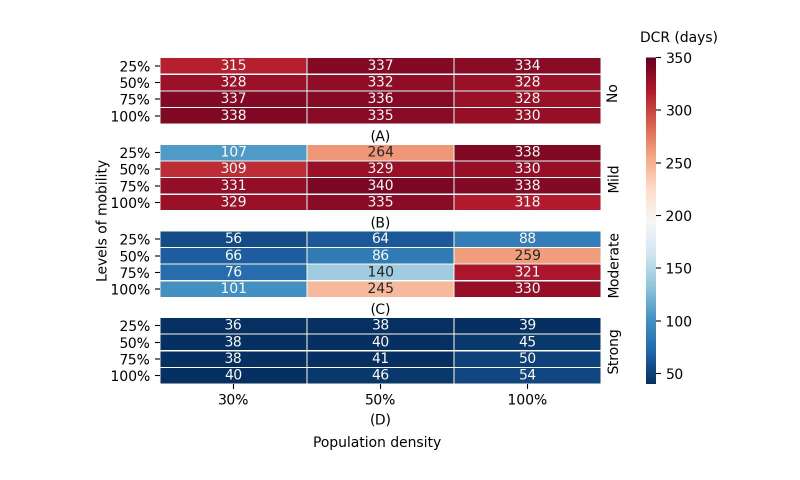
The team’s results also suggest strong physical distancing interventions implemented for short periods of time may be more effective than mild, longer term ones.
The author and spatial epidemiologist, Dr. Shengjie Lai, Senior Research Fellow in Geography and Environmental Sciences at the University of Southampton comments: “Our research provides a framework and set of outputs that can be used by policy-makers and public health authorities to identify appropriate levels of intervention to keep COVID-19 outbreaks in check over time.
Although our study was based on data from China, our methods and findings are applicable to cities worldwide with similar levels of population density and social contact patterns.”
Director of WorldPop, Professor Andy Tatem, added: “Previous studies have assumed that when people reduce mobility, they proportionately reduce their social contacts, but this isn’t necessarily the case and as more SARS-CoV-2 vaccines come online, there is an urgent need to understand the relationship between these factors, so we can adjust and tailor interventions and open up sections of society in a safer way.”
The researchers recognise some limitations to their study, for example, the absence of data on the contribution of handwashing and face masks and challenges of vaccine supply, but emphasise that their approach can be quickly adapted to provide near real-time data to address emerging, time critical needs.
The paper Integrated vaccination and physical distancing interventions to prevent future COVID-19 waves in Chinese cities is published in Nature Human Behaviour.
The 2019 novel coronavirus (COVID-19), known as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was recently identified as the causative agent of COVID-19 (1). The virus, originating from Wuhan, China, quickly spread throughout the world, leaving countries scrambling to assess the best containment methods (2).
Though the virus initially presented in the United States (U.S.) after infected individuals came into the country from international locations, the mode of transmission quickly became domestically person to person (3). Initially, some states, such as Washington, California, and New York were saw extremely high rates (4).
Throughout the pandemic, the states with the highest rates have changed (5). While states with large cities were initially disproportionately affected, with New York City (NYC), emerging as a “hotspot,” rates are now higher in states with larger rural populations (5, 6).
As the world started to learn more about the biology of SARS-CoV-2, proposals for containment measures attempted to address the modes of transmission. Spread of SARS-CoV-2 occurs primarily through respiratory droplets (7). However, the virus can also survive on hard surfaces for hours to days (8).
Because the spread of the virus is largely contingent upon proximity to one another, common containment measures included attempts to create physical distance (e.g. public health measures such as restrictions on gatherings) (9). As the U.S. federal government scrambled to establish containment measures, states and local governments laid out vastly heterogeneous rules on how individuals would prevent close contact (10,11).
In April of 2020, the Centers for Disease Control and Prevention (CDC) suggested that use of masks in public areas could be useful in addition to other physical distancing measures (12).
Analyses that have been reported on existing data show that mitigation efforts may be successful. A report from the CDC examined data from the metropolitan areas of San Francisco, Seattle, New Orleans and NYC in terms of the timing of policy measures, community mobility, and incidence rates.
They found that the percentage of residents leaving home declined as the number of policies issued increased, with data trends suggested that physical distancing measures may decrease incidence rates. The analysis was limited by lack of information on confounders (e.g. age, gender, and race) and limited data on mobile phone coverage (13).
Another study examined the impact of several physical distancing measures on the growth rate of confirmed COVID-19 cases using county level data across the U.S. They reported that government-imposed physical distancing measures reduced the daily growth rate by 5.4 % after 1–5 days, 6.8 % after 6–10 days, 8.2% after 11–15 days, and 9.1% after 16–20 days, and suggested that failure to enact these types of restrictions would fuel exponential spread (14).
Most current published studies utilize mathematical modeling to make predictions based on hypothetical situations, yielding a variety of conclusions. One study modeled the effects of physical distancing measures on the progression of the COVID-19 epidemic in Wuhan, which showed that physical distancing measures may be most successful if their relaxation is gradual rather than done as a sudden lifting of interventions. However, they noted that results varied by the duration of infectiousness and the role of school children in the epidemic (15).
Another group created a model to study the impact of physical distancing and school closure on viral transmission while accounting for age differences. They reported that physical distancing in China during their outbreak was sufficient to control COVID-19, with a 40-60% reduction in peak incidence with proactive school closures (16).
A mathematical model used to investigate the value of physical distancing interventions in a mid-sized U.S. city (modeled after Seattle) showed that interventions that start earlier in the epidemic delay the epidemic curve while interventions initiated later flatten the epidemic curve (17). A meta-analysis of 172 observational studies across 16 countries found that viral transmission was reduced with physical distancing (18).
This same study found that face mask use reduced the odds of infection (adjusted odds ratio= 0•15, 95% CI: 0•07-0•3) (19). The benefits of using masks may work in tandem with physical distancing. It has also been estimated. the number of excess cases per 100,000 residents in states reopening indoor dining rooms without masks was ten times the number in states reopening with masks after 8 weeks (643.1 cases; 95% confidence interval (CI) = 406.9, 879.2 and 62.9 cases; CI = 12.6, 113.1, respectively) (20).
Moreover, an analysis of the impact of policy measures has suggested that nationally mandating face masks for employees early in the pandemic could have reduced the weekly growth rate of cases and deaths by more than 10 percentage points in late April and could have led to as much as 19 to 47 percent less deaths nationally by the end of May. Cases would have been larger by six to 63 percent without stay-at-home orders and larger by 17 to 78 percent without business closures (21).
Hypothetical mask models support these results and one such study suggested that even weak (ineffective) masks could be useful in curbing disease transmission (22). It has also been noted that widespread implementation and enforcement of sustained community mitigation measures helped with mitigation of COVID-19, noting a decline in rates once measures were implemented (23).
Similarly, a study looking at daily county-level COVID-19 growth rates in 15 states and Washington, D.C., estimated that more than 200,000 COVID-19 cases could have been averted by May 22, 2020 if utilizing masks in public had been mandatory in all locations (24). While some of the data that has been published show protective outcomes from mask usage, not all studies show this and some have shown that when used improperly, the mask can actually facilitate infection (25).
Much of the research that has been published has not been guided by statistics when assessing the influence of physical distancing and other infection mitigation techniques on the COVID-19 infection rates. Reports have largely been based either on charting existing data and making conclusions by visual inspection, or creating models based on simulated data.
Additionally, many studies compare rates between states by looking at set dates, rather than adjusting for where a location is in their epidemic cycle. Given that the date of the first COVID-19 case in a state was widely spread around the country, comparison would be more appropriate while placing all states at the same starting point of an epidemic curve.
Finally, most studies have not accounted for socio-demographic factors. While many have suggested that population density is a factor in infection rates, this only addresses how many people exist in a given square footage of land and does not account for the structure in which these individuals are spaced throughout the state. On December 11, 2020 the Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the first COVID-19 vaccine and the first vaccination in the U.S. was given on December 14, 2020, marking the date at which the trajectory of disease rates will be changed by this intervention (26).
The purpose of the present study was to examine the impact of school closures, stay at home orders and mask mandates on cumulative incidence rates of COVID-19 in states up until vaccination was introduced, while investigating whether controlling for a variety of socio-demographic variables would affect results. Additionally, the effects of controlling by population density as well as the percent of percent of population represented by an urban population were examined.
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7872858/
More information: Nature Human Behaviour (2021). DOI: 10.1038/s41562-021-01063-2 , www.nature.com/articles/s41562-021-01063-2



{kind=link}